

Immediate Effect of a Kinesiotape Bandage on Knee Mechanics during Functional Tests in Female Rugby and Football Athletes: A Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Settings, and Ethical Aspects
2.2. Sample Size Calculation
2.3. Participants and Recruitment
2.4. Randomization
2.5. Variables
2.5.1. Anteroposterior Displacement of the Tibia Measured with Ultrasound
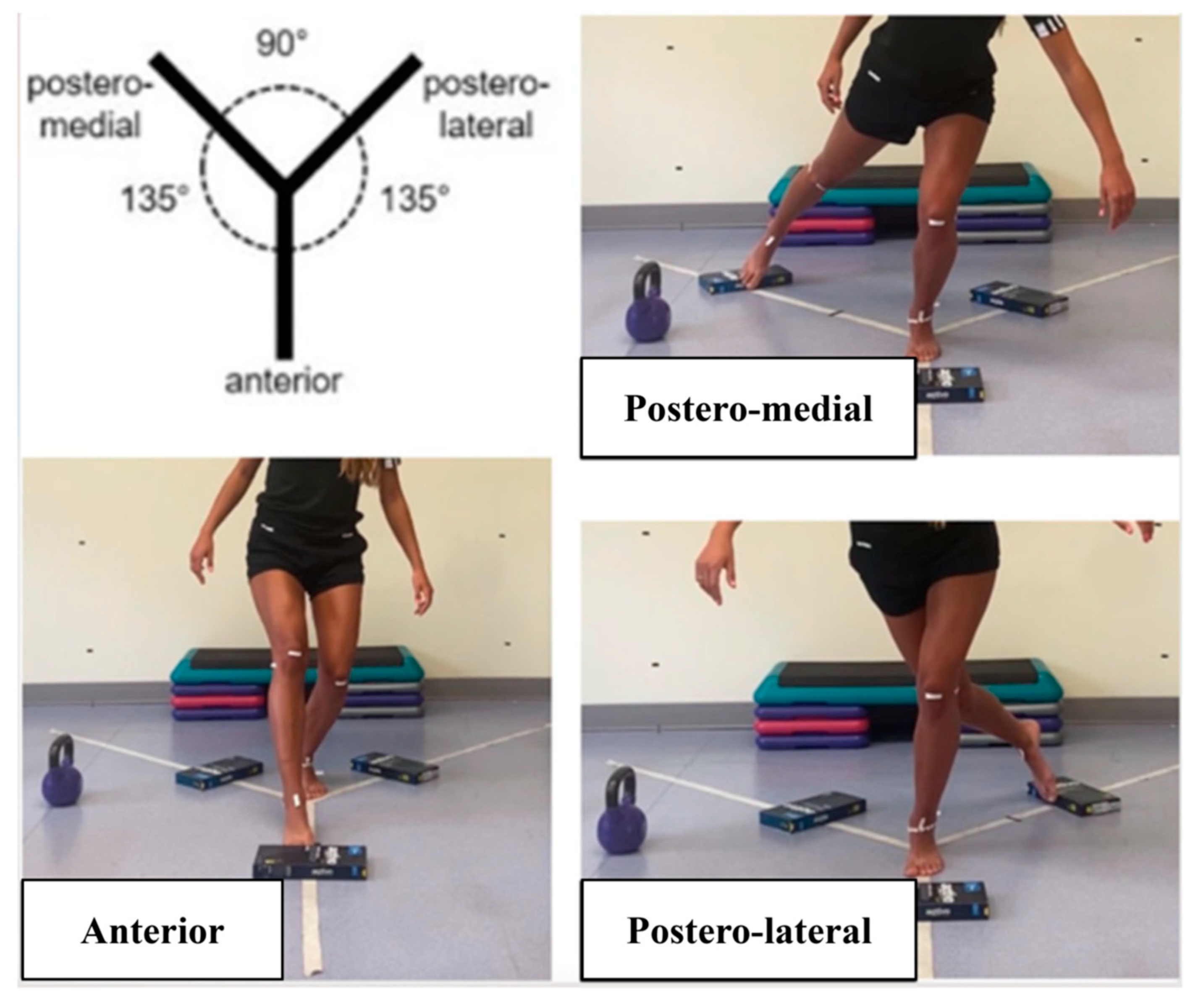
2.5.2. Y Balance Test (YBT)
2.5.3. Lateral Step Down (LSD)
2.5.4. Single Leg Squat (SLS)
2.5.5. Jump Landing Test (JLT)
2.6. Development of the Assessment Protocol and Intervention
2.7. Statistical Analysis
3. Results
3.1. Ultrasonographic Variables
3.2. Functional Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Markatos, K.; Kaseta, M.K.; Lallos, S.N.; Korres, D.S.; Efstathopoulos, N. The anatomy of the ACL and its importance in ACL reconstruction. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Acevedo, R.J.; Rivera-Vega, A.; Miranda, G.; Micheo, W. Anterior Cruciate Ligament Injury: Identification of Risk Factors and Prevention Strategies. Curr. Sports Med. Rep. 2014, 13, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Bisciotti, G.N.; Chamari, K.; Cena, E.; Bisciotti, A.; Bisciotti, A.; Corsini, A.; Volpi, P. Anterior cruciate ligament injury risk factors in football. J. Sports Med. Phys. Fit. 2019, 59, 1724–1738. [Google Scholar] [CrossRef] [PubMed]
- Griffin, L.Y.; Albohm, M.J.; Arendt, E.A.; Bahr, R.; Beynnon, B.D.; Demaio, M.; Dick, R.W.; Engebretsen, L.; Hannafin, J.A.; Hewett, T.E.; et al. Understanding and preventing noncontact anterior cruciate ligament injuries: A review of the Hunt Valley II meeting, January 2005. Am. J. Sports Med. 2006, 34, 1512–1532. [Google Scholar] [CrossRef] [PubMed]
- Bram, J.T.; Magee, L.C.; Mehta, N.N.; Patel, N.M.; Ganley, T.J. Anterior Cruciate Ligament Injury Incidence in Adolescent Athletes: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2021, 49, 1962–1972. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, A.M.; Schneider, D.K.; Yut, L.; Webster, K.E.; Beynnon, B.; Kocher, M.S.; Myer, G.D. “What’s my risk of sustaining an ACL injury while playing sports?” A systematic review with meta-analysis. Br. J. Sports Med. 2019, 53, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, A.M.; Schneider, D.K.; Webster, K.E.; Yut, L.; Galloway, M.T.; Heidt, R.S.; Kaeding, C.C.; Kremcheck, T.E.; Magnussen, R.A.; Parikh, S.N.; et al. Anterior Cruciate Ligament Injury Risk in Sport: A Systematic Review and Meta-Analysis of Injury Incidence by Sex and Sport Classification. J. Athl. Train. 2019, 54, 472–482. [Google Scholar] [CrossRef] [PubMed]
- Chia, L.; Silva, D.D.O.; Whalan, M.; McKay, M.J.; Sullivan, J.; Fuller, C.W.; Pappas, E. Non-contact Anterior Cruciate Ligament Injury Epidemiology in Team-Ball Sports: A Systematic Review with Meta-analysis by Sex, Age, Sport, Participation Level, and Exposure Type. Sports Med. 2022, 52, 2447–2467. [Google Scholar] [CrossRef]
- Waldén, M.; Hägglund, M.; Magnusson, H.; Ekstrand, J. ACL injuries in men’s professional football: A 15-year prospective study on time trends and return-to-play rates reveals only 65% of players still play at the top level 3 years after ACL rupture. Br. J. Sports Med. 2016, 50, 744–750. [Google Scholar] [CrossRef]
- Voskanian, N. ACL Injury prevention in female athletes: Review of the literature and practical considerations in implementing an ACL prevention program. Curr. Rev. Musculoskelet. Med. 2013, 6, 158–163. [Google Scholar] [CrossRef]
- Hewett, T.E.; Di Stasi, S.L.; Myer, G.D. Current concepts for injury prevention in athletes after anterior cruciate ligament reconstruction. Am. J. Sports Med. 2013, 41, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, A.; Francisco, R. Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: A prospective clinical investigation. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Silvers-Granelli, H.J.; Bizzini, M.; Arundale, A.; Mandelbaum, B.R.; Snyder-Mackler, L. Does the FIFA 11+ Injury Prevention Program Reduce the Incidence of ACL Injury in Male Soccer Players? Clin. Orthop. Relat. Res. 2017, 475, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Hewett, T.E. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J. Orthop. Res. 2018, 36, 2696–2708. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Whatman, C.; Hume, P.A.; Sheerin, K. Kinesio Taping in Treatment and Prevention of Sports Injuries. Sports Med. 2012, 42, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Howe, A.; Campbell, A.; Ng, L.; Hall, T.; Hopper, D. Effects of two different knee tape procedures on lower-limb kinematics and kinetics in recreational runners. Scand. J. Med. Sci. Sports 2015, 25, 517–524. [Google Scholar] [CrossRef]
- Villar, P.L.; Cabello, M.G.; Medigure, X.M.d.S.P.d.; Marne, P.S.C. Revisión del Kinesio Taping o vendaje neuromuscular como forma de tratamiento fisioterapéutico. Cuest. Fisioter. Rev. Univ. Inf. Investig. Fisioter. 2011, 40, 65–76. [Google Scholar]
- de Jesus, J.F.; Novello, A.d.A.; Nakaoka, G.B.; dos Reis, A.C.; Fukuda, T.Y.; Bryk, F.F. Kinesio taping effect on quadriceps strength and lower limb function of healthy individuals: A blinded, controlled, randomized, clinical trial. Phys. Ther. Sport 2016, 18, 27–31. [Google Scholar] [CrossRef]
- Lyman, K.J.; Keister, K.; Gange, K.; Mellinger, C.D.; A Hanson, T. Investigating the effectiveness of kinesio® taping space correction method in healthy adults on patellofemoral joint and subcutaneous space. Int. J. Sports Phys. Ther. 2017, 12, 250–257. [Google Scholar]
- Rajasekar, S.; Kumar, A.; Patel, J.; Ramprasad, M.; Samuel, A.J. Does Kinesio taping correct exaggerated dynamic knee valgus? A randomized double blinded sham-controlled trial. J. Bodyw. Mov. Ther. 2018, 22, 727–732. [Google Scholar] [CrossRef]
- Kielė, D.; Solianik, R. Four-Week Application of Kinesiotaping Improves Proprioception, Strength, and Balance in Individuals With Complete Anterior Cruciate Ligament Rupture. J. Strength Cond. Res. 2023, 37, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, L.; Babisch, C.; Babisch, J.; Layher, F.; Sander, K.; Matziolis, G.; Pietsch, S.; Röhner, E. Effects on proprioception by Kinesio taping of the knee after anterior cruciate ligament rupture. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Ogrodzka-Ciechanowicz, K.; Głąb, G.; Ślusarski, J.; Gądek, A.; Nawara, J. Does kinesiotaping can improve static stability of the knee after anterior cruciate ligament rupture? A randomized single-blind, placebo-controlled trial. BMC Sports Sci. Med. Rehabil. 2021, 13, 24. [Google Scholar] [CrossRef] [PubMed]
- Espí-López, G.V.; Serra-Añó, P.; Cobo-Pascual, D.; Zarzoso, M.; Suso-Martí, L.; Cuenca-Martínez, F.; Inglés, M. Effects of Taping and Balance Exercises on Knee and Lower-Extremity Function in Amateur Soccer Players: A Randomized Controlled Trial. J. Sport Rehabil. 2019, 29, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Sheikhi, B.; Letafatkar, A.; Hogg, J.; Naseri-Mobaraki, E. The influence of kinesio taping on trunk and lower extremity motions during different landing tasks: Implications for anterior cruciate ligament injury. J. Exp. Orthop. 2021, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Limroongreungrat, W.; Boonkerd, C. Immediate effect of ACL kinesio taping technique on knee joint biomechanics during a drop vertical jump: A randomized crossover controlled trial. BMC Sports Sci. Med. Rehabil. 2019, 11, 32. [Google Scholar] [CrossRef]
- Martonick, N.; Kober, K.; Watkins, A.; DiEnno, A.; Perez, C.; Renfro, A.; Chae, S.; Baker, R. The Effect of Kinesio Tape on Factors for Neuromuscular Control of the Lower-Extremity: A Critically Appraised Topic. J. Sport Rehabil. 2020, 29, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Haynes, A.B.; Haukoos, J.S.; Dimick, J.B. TREND Reporting Guidelines for Nonrandomized/Quasi-Experimental Study Designs. JAMA Surg. 2021, 156, 879–880. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short form (IPAQ-SF): A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef]
- Stoianov, A.G.; Pătrașcu, J.M.; Hogea, B.G.; Andor, B.; Mișcă, L.C.; Florescu, S.; Onofrei, R.R.; Pătrașcu, J.M. Dynamic Ultrasound Assessment of the Anterior Tibial Translation for Anterior Cruciate Ligament Tears Diagnostic. J. Clin. Med. 2022, 11, 2152. [Google Scholar] [CrossRef]
- Powden, C.J.; Dodds, T.K.; Gabriel, E.H. The Reliability of the Star Excursion Balance Test and Lower Quarter Y-Balance Test in Healthy Adults: A systematic review. Int. J. Sports Phys. Ther. 2019, 14, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, C.; Rethman, K.; Stephens, J.; Di Stasi, S.; Vanetten, L.; Briggs, M. The association and reliability of the frontal plane projection angle during the lateral step down test on knee function in patients with patellofemoral pain. Knee 2022, 36, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Ugalde, V.; Brockman, C.; Bailowitz, Z.; Pollard, C.D. Single leg squat test and its relationship to dynamic knee valgus and injury risk screening. PM&R 2015, 7, 229–235. [Google Scholar] [CrossRef]
- Mehl, J.; Diermeier, T.; Herbst, E.; Imhoff, A.B.; Stoffels, T.; Zantop, T.; Petersen, W.; Achtnich, A. Evidence-based concepts for prevention of knee and ACL injuries. 2017 guidelines of the ligament committee of the German Knee Society (DKG). Arch. Orthop. Trauma Surg. 2018, 138, 51–61. [Google Scholar] [CrossRef]
- Schroeder, A.B.; Dobson, E.T.A.; Rueden, C.T.; Tomancak, P.; Jug, F.; Eliceiri, K.W. The ImageJ ecosystem: Open-source software for image visualization, processing, and analysis. Protein Sci. 2021, 30, 234–249. [Google Scholar] [CrossRef]
- Munro, A.; Herrington, L.; Carolan, M. Reliability of 2-dimensional video assessment of frontal-plane dynamic knee valgus during common athletic screening tasks. J. Sport Rehabil. 2012, 21, 7–11. [Google Scholar] [CrossRef]
- Ogrodzka-Ciechanowicz, K.; Stolarz, M.; Gła̧b, G.; Ślusarski, J.; Ga̧dek, A. Biomechanical image of the knee motion in patients with chronic anterior instability of the knee joint before and after Kinesio Taping. J. Back Musculoskelet. Rehabil. 2020, 33, 169–177. [Google Scholar] [CrossRef]
- Kase, K.; Wallis, J.; Kase, T. Clinical Therapeutic Applications of the Kinesio Taping Method, 2nd ed.; Albuquerque, Kinesio Taping Assoc: Tokyo, Japan, 2003. [Google Scholar]
- Almazán-Polo, J.; López-López, D.; Romero-Morales, C.; Rodríguez-Sanz, D.; Becerro-De-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Bravo-Aguilar, M.; Calvo-Lobo, C. Quantitative Ultrasound Imaging Differences in Multifidus and Thoracolumbar Fasciae between Athletes with and without Chronic Lumbopelvic Pain: A Case-Control Study. J. Clin. Med. 2020, 9, 2647. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 62627. [Google Scholar] [CrossRef]
- Johnson, J.L.; Capin, J.J.; Arundale, A.J.; Zarzycki, R.; Smith, A.H.; Snyder-Mackler, L. A Secondary Injury Prevention Program May Decrease Contralateral Anterior Cruciate Ligament Injuries in Female Athletes: 2-Year Injury Rates in the ACL-SPORTS Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2020, 50, 523–530. [Google Scholar] [CrossRef]
- Moriceau, J.; Fevre, A.; Domínguez-Balmaseda, D.; González-De-La-Flor, Á.; Simón-Areces, J.; García-Pérez-De-Sevilla, G. The Influence of the Menstrual Cycle and Oral Contraceptives on Knee Laxity or Anterior Cruciate Ligament Injury Risk: A Systematic Review. Appl. Sci. 2022, 12, 12627. [Google Scholar] [CrossRef]
- Boden, B.P.; Sheehan, F.T.; Torg, J.S.; Hewett, T.E. Noncontact anterior cruciate ligament injuries: Mechanisms and risk factors. J. Am. Acad. Orthop. Surg. 2010, 18, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Sahabuddin, F.N.A.; Jamaludin, N.I.; Amir, N.H.; Shaharudin, S. The effects of hip- and ankle-focused exercise intervention on dynamic knee valgus: A systematic review. PeerJ 2021, 9, e11731. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D. The mechanistic connection between the trunk, hip, knee, and anterior cruciate ligament injury. Exerc. Sport Sci. Rev. 2011, 39, 161–166. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Min–Max | Mean (SD) |
|---|---|---|
| Age (years) | 18–31 | 21.90 ± 3.48 |
| Height (cm) | 159–171 | 165.00 ± 0.04 |
| Weight (kg) | 50–68 | 57.55 ± 5.63 |
| BMI (kg/m2) | 18.56–25.91 | 21.10 ± 2.55 |
| Physical activity level (MET/min/week) | 1653–4692 | 2861.10 ± 949.62 |
| Variables | GROUP | T1 | T2 | p-Time | p-txg | η2p txg |
|---|---|---|---|---|---|---|
| Anterior displacement (cm) | IG CG | 0.13 ± 0.11 0.10 ± 0.09 | 0.08 ± 0.04 0.08 ± 0.05 | 0.10 | 0.43 | 0.14 |
| Posterior displacement (cm) | IG CG | 0.08 ± 0.07 0.10 ± 0.05 | 0.05 ± 0.03 0.06 ± 0.05 | 0.10 | 0.43 | 0.04 |
| Total displacement (cm) | IG CG | 0.21 ± 0.17 0.20 ± 0.13 | 0.13 ± 0.05 0.15 ± 0.05 | 0.02 * | 0.67 | 0.01 |
| Variables | GROUP | T1 | T2 | p-Time | p-txg | η2p txg | |
|---|---|---|---|---|---|---|---|
| Y balance Test | ANT (cm) | IG CG | 61.95 ± 4.73 62.47 ± 4.55 | 60.03 ± 4.90 63.01 ± 3.74 | 0.01 * | 0.76 | 0.01 |
| MED (cm) | IG CG | 71.93 ± 6.31 73.38 ± 5.71 | 73.96 ± 6.91 75.21 ± 7.49 | 0.13 | 0.93 | 0.00 | |
| LAT (cm) | IG CG | 76.15 ± 8.58 76.22 ± 8.19 | 76.82 ± 6.09 78.76 ± 6.73 | 0.29 | 0.53 | 0.06 | |
| LSD (degrees) | IG CG | 151.40 ± 11.04 156.96 ± 5.44 | 157.10 ± 10.18 158.68 ± 6.12 | <0.01 * | 0.02 * | 0.26 | |
| SLS (degrees) | IG CG | 167.55 ± 12.03 169.27 ± 6.50 | 173.32 ± 10.50 172.75 ± 5.86 | <0.01 * | 0.17 | 0.10 | |
| JLT | P0 (degrees) | IG CG | 178.87 ± 7.40 180.10 ± 9.01 | 178.83 ± 6.29 181.90 ± 6.90 | 0.53 | 0.51 | 0.03 |
| P1 (degrees) | IG CG | 186.66 ± 10.96 185.95 ± 13.85 | 184.42 ± 12.59 188.50 ± 9.16 | 0.93 | 0.20 | 0.09 | |
| P2 (degrees) | IG CG | 185.68 ± 6.26 183.73± 4.57 | 185.77 ± 8.76 184.95 ± 7.70 | 0.57 | 0.63 | 0.01 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fevre, A.; Moriceau, J.; Almazán-Polo, J.; García-Pérez-de-Sevilla, G. Immediate Effect of a Kinesiotape Bandage on Knee Mechanics during Functional Tests in Female Rugby and Football Athletes: A Pilot Study. Appl. Sci. 2024, 14, 2839. https://doi.org/10.3390/app14072839
Fevre A, Moriceau J, Almazán-Polo J, García-Pérez-de-Sevilla G. Immediate Effect of a Kinesiotape Bandage on Knee Mechanics during Functional Tests in Female Rugby and Football Athletes: A Pilot Study. Applied Sciences. 2024; 14(7):2839. https://doi.org/10.3390/app14072839
Chicago/Turabian StyleFevre, Amandine, Juliette Moriceau, Jaime Almazán-Polo, and Guillermo García-Pérez-de-Sevilla. 2024. "Immediate Effect of a Kinesiotape Bandage on Knee Mechanics during Functional Tests in Female Rugby and Football Athletes: A Pilot Study" Applied Sciences 14, no. 7: 2839. https://doi.org/10.3390/app14072839