
Adjuvantation of Influenza Vaccines to Induce Cross-Protective Immunity


Biomedical & Pharmaceutical Sciences, College of Pharmacy, University of Rhode Island, 7 Greenhouse Road, Avedisian Hall, Room 480, Kingston, RI 02881, USA
*
Author to whom correspondence should be addressed.
Vaccines 2021, 9(2), 75; https://doi.org/10.3390/vaccines9020075
Submission received: 6 December 2020
/
Revised: 13 January 2021
/
Accepted: 15 January 2021
/
Published: 21 January 2021
(This article belongs to the Special Issue Antibodies in Influenza Vaccine and Therapeutic Design)
Abstract
:Influenza poses a huge threat to global public health. Influenza vaccines are the most effective and cost-effective means to control influenza. Current influenza vaccines mainly induce neutralizing antibodies against highly variable globular head of hemagglutinin and lack cross-protection. Vaccine adjuvants have been approved to enhance seasonal influenza vaccine efficacy in the elderly and spare influenza vaccine doses. Clinical studies found that MF59 and AS03-adjuvanted influenza vaccines could induce cross-protective immunity against non-vaccine viral strains. In addition to MF59 and AS03 adjuvants, experimental adjuvants, such as Toll-like receptor agonists, saponin-based adjuvants, cholera toxin and heat-labile enterotoxin-based mucosal adjuvants, and physical adjuvants, are also able to broaden influenza vaccine-induced immune responses against non-vaccine strains. This review focuses on introducing the various types of adjuvants capable of assisting current influenza vaccines to induce cross-protective immunity in preclinical and clinical studies. Mechanisms of licensed MF59 and AS03 adjuvants to induce cross-protective immunity are also introduced. Vaccine adjuvants hold a great promise to adjuvant influenza vaccines to induce cross-protective immunity.

1. Introduction
Influenza is a highly contagious viral infectious disease [1]. Based on the World Health Organization (WHO), influenza causes 3–5 million severe illnesses and 290,000–650,000 deaths each year worldwide. Influenza viruses are negative-sensed, single-stranded, segmented RNA viruses [2,3]. Influenza viruses belong to the virus family Orthomyxoviridae [2,3]. There are four types of influenza viruses: A, B, C, and D [4]. Human influenza is often caused by type A and B viruses [3]. Hemagglutinin (HA) and neuraminidase (NA) are highly abundant viral surface proteins with important roles in viral infection and release [3]. There are a total of 18 HA and 11 NA subtypes, giving rise to 198 possible influenza A subtypes [3]. Not all influenza A subtypes have been found in nature [4]. The natural hosts of influenza A viruses are wild aquatic birds, although influenza A viruses have also adapted to a variety of avian and mammalian species [5]. H1N1 and H3N2 are two major influenza A subtypes that cause annual influenza epidemics in humans [4]. Different from influenza A viruses, influenza B viruses have only two lineages (Victoria and Yamagata) and only infect humans and seals [3,6]. Influenza viruses have a high mutation rate due to the lack of proofreading of RNA-dependent RNA polymerase [7]. Based on reports, the annual mutation rates for the non-structural genes of influenza A and B viruses are about 2.0 × 10−3 and 0.6 × 10−3 nucleotide substitutions/site, respectively [8]. The high mutation rates of influenza A viruses cause frequent sequence changes of HA, leading to antigenic drift [3,9,10]. Antigenic drift enables influenza viruses to evade host immune surveillance and cause epidemics [3,9]. The co-infection of different influenza A subtypes can also cause reassortment, a process by which influenza viruses exchange gene segments and generate new viruses [9]. Due to the lack of preexisting immunity, the reassortant viruses have a high risk to cause influenza pandemics if sufficient human-to-human transmission can be established [9,11,12]. Four major influenza pandemics have occurred in human history: the 1918 H1N1 pandemic, the 1957 H2N2 pandemic, the 1968 H3N2 pandemic, and the 2009 H1N1 pandemic [13,14]. The 1918 influenza pandemic infected about one-third of the global population and claimed 50 million lives [15]. The 1957 H2N2 and 1968 H3N2 influenza pandemics each claimed about one million lives [13,16]. The most recent 2009 influenza pandemic claimed an estimated 151,700−575,400 lives [16,17]. The 1957 H2N2 influenza contains three genes from an avian influenza A virus, and the 1968 H3N2 influenza contains two genes from an avian influenza A virus [13], while the 2009 H1N1 influenza contains a unique combination of genes from avian, human, and swine influenza A viruses [18].
Influenza vaccines remain the most effective and cost-effective means to control influenza [19,20]. Yet, current influenza vaccines mainly induce strain-specific protection with little or no protection against drifted or shifted viruses. Universal influenza vaccines are under active development to induce broad cross-protective immunity [21,22,23]. In addition to a universal influenza vaccine approach, the incorporation of vaccine adjuvants has been found to broaden influenza vaccine-induced immune responses. This review focuses on introducing vaccine adjuvants that are capable of assisting current influenza vaccines to induce broad cross-protective immunity.
2. Current Influenza Vaccines and Limitations
Influenza vaccines are produced each year to mitigate influenza-caused morbidity and mortality [19,20]. Different types of influenza vaccines are available in the global market (Table 1). Based on the number of vaccine viral strains, influenza vaccines can be divided into trivalent or quadrivalent vaccines with the former containing two type A (H1N1, H3N2) and one type B (Victoria or Yamagata) strains and the latter containing two type A (H1N1, H3N2) and two type B (Victoria and Yamagata) strains [24,25]. Influenza vaccines can also be classified into inactivated or attenuated vaccines [26]. Inactivated vaccines can be further divided into subunit, split-virion, and virosome vaccines [26]. Live-attenuated influenza vaccines undergo limited proliferation in respiratory epithelial cells following intranasal (IN) delivery [26]. Inactivated subunit vaccines are prepared by the disruption of viruses by detergents followed by purification of HA and NA as the major vaccine antigens [26]. Inactivated split-virion vaccines are prepared by the disruption of viruses by detergents without further purification [26]. As a result, split-virion vaccines contain additional viral components as compared to subunit vaccines [26]. Virosome vaccines are prepared by the detergent solubilization of viral membrane followed by nucleocapsid removal and then detergent removal to allow the viral membrane to self-assemble into virus-like particles (VLPs) [27]. Influenza virosome vaccines simulate native viruses in cell binding and membrane fusion [27]. Influenza virosome vaccine (Inflexal V) is the only influenza vaccine that has been approved for all age groups [28]. Based on the production methods, influenza vaccines can be classified into egg, cell, or recombinant protein-based [26,29]. Embryonic eggs have a long history of being used to expand influenza viruses to produce influenza vaccines [30]. Yet, embryonic egg-based influenza vaccine manufacturing is a lengthy process and also depends on egg supply [29]. To overcome these limitations, cell-based influenza vaccine manufacturing has been developed, in which influenza viruses are propagated in mammalian cells, such as Madin–Darby Canine Kidney (MDCK) cells [31]. Cell-based influenza vaccine manufacturing is not limited by egg supply and less likely to introduce viral mutations [26]. Recombinant influenza vaccines have been developed based on recombinant DNA technologies [32]. One such vaccine (Flublok) is produced in insect cells using Baculovirus Expression Systems [33]. As compared to egg and cell-based vaccines, recombinant influenza vaccines can be more quickly produced without the use of live viruses [29]. Based on the delivery routes, influenza vaccines can be classified into intramuscular (IM), intradermal (ID), and IN vaccines [19,34]. Most of the inactivated influenza vaccines are delivered into the muscular tissue by hypodermic needles, while live-attenuated vaccines are delivered by Intranasal Sprayer to the upper respiratory tract [34]. IN influenza vaccination provides an important alternative to needle-based IM vaccination for those who have needle phobia [35]. Needle-free Jet Injectors, such as PharmaJet and Bioject ZetaJet, have been also developed for the IM delivery of inactivated influenza vaccines [36,37,38]. Due to the richness of antigen-presenting cells (APCs) in the skin [39,40], inactivated influenza vaccines are also approved for ID delivery by Intradermal Microinjection Systems and MicronJet600 to save vaccine dose and cost [41,42]. Based on the usage, influenza vaccines can be divided into seasonal, pre-pandemic, and pandemic vaccines [32]. Seasonal influenza vaccines are made based on viral strains predicted to circulate in the next flu season [20,43]. Pre-pandemic influenza vaccines are prepared based on viral strains with a high risk to cause influenza pandemics, such as highly pathogenic avian influenza (HPAI) H5N1 and H7N9 viruses [44,45]. Pre-pandemic influenza vaccines are stockpiled to facilitate a quick response in case of real pandemics [44]. Pandemic influenza vaccines are made based on pandemic viral stains to control the spread of pandemic influenza [46].
Current influenza vaccines mainly induce neutralizing antibodies against the globular head of HA, lacking cross-protection against drifted or shifted viral strains [21,26,29]. HA is a type I transmembrane glycoprotein and forms trimeric spikes on the influenza viral surface [47,48,49]. To form functional HA, HA precursor HA0 needs to be cleaved by cellular protease to form HA1 and HA2 linked by disulfide bonds [50]. Functional HA is composed of a globular head and a stem domain [47]. The globular head is comprised of part of HA1, and the stem domain is comprised of the remaining HA1 and part of HA2 [47]. The remaining HA2 is composed of a transmembrane domain and a cytosolic tail [47]. HA plays crucial roles in viral infection. HA binds to sialic acids on the host cell surface and mediates the fusion of viral envelop with the late endosomal membrane of host cells2. Based on the sequence and antigenic relatedness of HA, influenza A viruses can be divided into group 1 (H1, H2, H5, H6, H8, H9, H11, H12, H13, H16, H17, and H18) and group 2 viruses (H3, H4, H7, H10, H14, and H15) [47].
Due to the immune selection pressure, the globular head of HA undergoes constant antigenic drift [10,47], which requires influenza vaccines to be manufactured each year. Considering that influenza viruses to circulate in the next flu season are predicted based on surveillance [20,43], the selected vaccine viral strains may not exactly match circulating viral strains. Vaccine mismatch often leads to low vaccine effectiveness and surging influenza cases [20,43]. In the 2014–2015 flu season, influenza A H3N2 viruses drifted significantly after the selection of vaccine viral strains [51]. Consequently, influenza vaccine effectiveness against the drifted H3N2 strain was only 6%, and the overall vaccine effectiveness was only 19% [52]. There were also significant vaccine mismatches in the 2004–2005 and 2005–2006 flu seasons, which resulted in low vaccine effectiveness in the two flu seasons (10 and 21%, respectively) [53]. In contrast, vaccine effectiveness is usually between 40 and 60% with a good vaccine match [52]. Egg-based vaccine manufacturing sometimes introduces mutations in immunodominant regions of HA, leading to reduced vaccine effectiveness [26].
Due to the high risk of HPAI H5N1 and H7N9 viruses to cause influenza pandemics, pre-pandemic H5N1 and H7N9 vaccines have been stockpiled [44,54]. HPAI H5N1 viruses mainly infect birds and are highly contagious among them [11]. The first human infection of H5N1 was identified in 1997 amid a poultry outbreak in Hong Kong, China [45]. H5N1 viruses have infected about 700 people in primarily 15 countries in Asia, Africa, the Pacific, Europe and the Near East with ≈60% lethality rate [45]. The first human infection of H7N9 occurred in China in 2013 [45]. Ever since, H7N9 has caused almost annual epidemics in humans [55]. The largest epidemic caused about 766 human infections in 2016–2017 [55]. Overall, H7N9 caused more than 1500 human infections with a lethality rate of ≈39% [55]. Although most H5N1 and H7N9 infections in humans were due to the close contact with poultry, human-to-human transmission may occur as a result of viral gene reassortment [45]. Different types of H5N1 and H7N9 vaccines have been developed and evaluated in clinical studies that include subunit, split-virion, and whole-inactivated vaccines [54,56]. H5N1 and H7N9 vaccines often require two immunizations and high antigen amounts (45 or 90 µg) to induce protective immune responses due to their low immunogenicity [57,58,59,60]. Molecular epidemiology studies found that H5N1 viruses had evolved into different clades and subclades, and H7N9 viruses had evolved into distinct lineages [61,62]. Similar to the seasonal influenza vaccine, H5N1 and H7N9 vaccines alone lack the ability to induce cross-clade or cross-lineage immunity [59,63].
3. Vaccine Adjuvants
Adjuvants(Latin word “adjuvare”, meaning to “help”) are traditionally defined as chemicals added to vaccine preparations to help vaccines to work better [64,65]. Considering vaccines are mainly given to healthy populations, adjuvants need to have a high level of safety to be approved for human use [64,66,67]. Experimental adjuvants, such as complete and incomplete Freund’s adjuvants, lipopolysaccharide (LPS), and a variety of cytokines, possess potent vaccine adjuvant effects and yet are less likely to be approved for human use due to their high risk to induce significant local or systemic adverse reactions [64,68,69].
Aluminum salt-based Alum adjuvant represents the first and most widely used adjuvant in the globe [70,71,72]. Alum adjuvant was discovered in 1920s by Raman and Glenny based on the observation that the precipitation of vaccines on insoluble aluminum salts could enhance vaccine-induced immune responses [70,71,72]. Then, Alum adjuvant was incorporated into tetanus and diphtheria vaccines and broadly used in humans [70,71,72]. Interestingly, Alum adjuvant was ineffective to enhance seasonal, pre-pandemic, or pandemic influenza vaccine efficacy [73,74,75,76]. Alum adjuvant mainly induces type 2 T helper (Th2)-biased immune responses and was originally thought to act through an “antigen depot”. In 2012, Hutchison et al. found that the removal of Alum depot as early as 2 h after administration had no significant impact on antigen-specific T and B cell responses [77]. Instead, Kool et al. found that Alum adjuvant could induce uric acid release and activate inflammatory dendritic cells (DCs) to mediate its adjuvant effects [78]. Several studies also found that Alum adjuvant could activate the Nod-like receptor (NLR) family pyrin domain containing 3 (NALP3) inflammasome, leading to Caspase-1 activation and interleukin 1β (IL-1β) release [79,80,81]. Yet, the depletion of NALP3 only affected antigen-specific IgE but not IgG1 or IgG2 antibody production [81,82,83]. More work is needed to elucidate how Th2-biased immune responses are induced by Alum-adjuvanted vaccines [83,84]. Alum adjuvant remained the only adjuvant for more than half a century until squalene emulsion-based MF59 adjuvant was approved by European Authorities in 1997 to enhance seasonal influenza vaccine efficacy in the elderly [85,86,87]. MF59 was approved in 2015 to enhance seasonal influenza vaccine efficacy in the elderly in the United States [88,89]. MF59 has been also licensed to boost seasonal influenza vaccine efficacy in children aged 6 months to 2 years old in Canada since 2015 [90]. In addition to seasonal influenza vaccines, MF59 has been also incorporated into pre-pandemic H5N1 and H7N9 vaccines to spare vaccine doses [91,92]. Overall, millions of MF59-containing influenza vaccine doses have been administered in humans with a good safety profile [85,86,87]. After MF59, several adjuvant system (AS)-based adjuvants, such as AS01, AS03, and AS04, were approved for human use [93,94]. AS04 is prepared by the adsorption of monophosphoryl lipid A (MPL) onto Alum adjuvant and was approved to improve human papillomavirus (HPV) vaccine efficacy in 2009 [95,96]. MPL is a non-toxic derivative of LPS and a potent Toll-like receptor (TLR) 4 agonist [66,97]. AS03 represents another squalene emulsion-based adjuvant [98,99]. AS03 was incorporated into the influenza pandemic 2009 H1N1 vaccine in Europe [100,101]. AS03 was also incorporated into the pre-pandemic H5N1 vaccine stockpiled in the United States [102]. AS01 and AS02 are MPL and QS21-containing liposome and water-in-oil emulsion, respectively [93,103,104]. AS01 was approved to boost pre-erythrocytic RTS, S malaria vaccine efficacy in 2015 [94,105,106]. Recently, CpG 1018 was approved to boost hepatitis B VLP vaccine efficacy [107,108]. CpG 1018 is a 22-mer oligonucleotide and activates TLR9 [107,109]. An overview of currently approved vaccine adjuvants is summarized in Table 2.
Adjuvant development lagged behind vaccine development for a long time. This trend is gradually changing with increasing understanding of adjuvant mechanisms and more investments in adjuvant research and development. The various benefits of adjuvants include enhancing vaccine-induced immune responses, improving vaccine efficacy in the elderly, sparing vaccine doses, inducing early-onset and long-lasting immune responses, and eliciting cross-protective immunity [64,66]. Different types of adjuvants have been explored to increase seasonal, pre-pandemic, and pandemic influenza vaccine efficacy, spare vaccine doses, and broaden vaccine-induced immune responses. This review focuses on introducing vaccine adjuvants capable of assisting current influenza vaccines to induce cross-protective immunity.
4. Vaccine Adjuvants Assist Influenza Vaccines to Induce Cross-Protective Immunity
Licensed adjuvants, such as MF59 and AS03, are incorporated into seasonal, pre-pandemic, and pandemic influenza vaccines to enhance vaccine efficacy in the elderly or spare vaccine doses. MF59 and AS03-adjuvanted influenza vaccines were found to induce cross-protective immunity in humans (Table 3). In addition to licensed adjuvants, various types of experimental adjuvants were found to also assist influenza vaccines to induce cross-protective immunity, such as TLR agonists (e.g., MPL, Imiquimod, CpG), saponin-containing adjuvants, and non-traditional physical adjuvants (Table 4).
4.1. MF59
4.1.1. Induction of Cross-Protective Immunity against Seasonal Influenza Vaccine
Minutello et al. conducted a small-scale study to compare the relative immunogenicity of MF59-adjuvanted seasonal influenza vaccine with non-adjuvanted vaccine in elderly ambulatory patients in the 1992–1995 flu seasons [110]. MF59-adjuvanted vaccine induced higher hemagglutination inhibition (HI) geometric mean titer (GMT) and higher seroconversion rates than the non-adjuvanted vaccine in each flu season [110]. Interestingly, the MF59-adjuvanted but not the non-adjuvanted vaccine in the 1992–1993 flu season induced significant HI GMT against heterologous viruses used to produce seasonal influenza vaccines for the 1993–1994 flu season [110]. This study hinted that MF59 might broaden influenza vaccine-induced antibody responses against non-vaccine viral strains. This hypothesis was confirmed in a later study, in which Ansaldi et al. compared HI GMT and seroconversion rates of MF59-adjuvanted and non-adjuvanted vaccines in the 2004–2005 flu season against heterologous H3N2 viruses circulated in four prior and two subsequent flu seasons in the elderly [111]. The MF59-adjuvanted vaccine induced significantly higher HI GMT against heterologous H3N2 strains circulated in subsequent flu seasons and significantly higher seroconversion rates against heterologous H3N2 strains circulated in prior and subsequent flu seasons as compared to non-adjuvanted vaccine [111]. In addition to the elderly, MF59-adjuvanted seasonal influenza vaccine also induced heterologous immunity in young children. Nolan et al. found that the MF59-adjuvanted seasonal influenza vaccine induced significantly higher HI GMT and seroconversion rates against heterologous type A and B viruses in infants and young children than the non-adjuvanted vaccine [112].
4.1.2. Induction of Cross-Clade Immunity against Pre-Pandemic Influenza Vaccine
MF59 adjuvant was explored to spare pre-pandemic H5N1 vaccine doses and induce cross-clade protection. Banzhoff et al. found that two priming doses of MF59-adjuvanted H5N1 vaccine based on clade 1 strain (A/Vietnam/1194/2004) could induce HI titer of at least 40 in 81–86% non-elderly adults and 76–79% elderly adults [113]. Moreover, two priming doses of MF59-adjuvanted H5N1 vaccine also induced significant neutralizing antibody titer against clade 2 strain (A/Turkey/Turkey/1/05) [113]. The cross-clade antibody responses significantly dropped 6 months later and yet could be boosted to above the protective levels by a single dose of the same vaccine [113]. In addition to adults, the MF59-adjuvanted H5N1 vaccine could also induce cross-clade antibody responses in pediatrics. Vesikari et al. found that two priming doses of MF59-adjuvanted H5N1 vaccine based on clade 1 strain (A/Vietnam/1194/2004) could induce significant microneutralization (MN) antibody titer against clade 2 strains (A/Indonesia/5/2005 and A/Anhui/1/2005) in pediatrics [114]. Despite significantly reduced antibody levels one year later, MN antibody titer against clade 2 strains could be boosted to more than 40 in most of the pediatrics by a single dose of the same vaccine [114]. These studies found that MF59 adjuvant was crucial to induce cross-clade antibody responses in homologous prime/boost immunizations. MF59 was also explored in heterologous prime/boost immunizations to induce cross-clade immunity. Galli et al. found MF59-adjuvanted clade 0-like H5N3 (A/duck/Singapore/1997) vaccine prime followed by MF59-adjuvanted clade 1 H5N1 (A/Vietnam/1194/2004) vaccine boost 6 years later could induce more rapid, higher, and longer duration of cross-reactive antibody responses against clade 0, 1, and 2 strains as compared to non-adjuvanted vaccine prime and MF59-adjuvanted clade 1 H5N1 vaccine boost [115]. This study indicated crucial roles of MF59 adjuvant in the H5N1 vaccine prime to induce cross-clade antibody responses after boost with heterologous H5N1 vaccine years later. The above studies support the incorporation of MF59 adjuvant in stockpiled H5N1 vaccines to facilitate the induction of cross-clade antibody responses following homologous and heterologous prime/boost immunizations.
In addition to the H5N1 vaccine, MF59-like SWE adjuvant was found to significantly increase the immunogenicity of the H7N9 vaccine, spare vaccine dose, and induce cross-protective immune responses against H7 viral strains of different lineages in ferrets [116]. Hatta et al. found that the MF59-like AddaVax adjuvant could significantly increase H7N9 vaccine efficacy and induce cross-protection against an antigenically distinct and highly pathogenic H7N9 viruses in ferrets [117].
4.1.3. Safety
MF59-adjuvanted seasonal and pre-pandemic influenza vaccines were well tolerated in different age groups in humans [110,112,113,114,115]. No severe adverse events were related to MF59-adjuvanted influenza vaccination [110,112,113,114,115]. Yet, MF59-adjuvanted influenza vaccines were observed to induce more frequent local and systemic adverse reactions than non-adjuvanted vaccines [110,112,113,114,115]. The most common local adverse reaction was injection-site pain, and the most common systemic adverse reactions were myalgia and headache [112,113,115]. Most of the local and systemic adverse reactions were mild to moderate without the need for medical treatments.
4.1.4. Mechanistic Insights
Khurana el al. looked into the cross-protective mechanisms of the MF59-adjuvanted H5N1 vaccine [118]. Whole-genome-fragment phage display libraries were used to map HA and NP epitopes capable of binding polyclonal antibodies of immune sera [118]. It was found that MF59-adjuvanted H5N1 vaccine induced a high frequency (60%) of anti-HA1 antibodies and broad anti-NA antibodies [118]. In contrast, non-adjuvanted and Alum-adjuvanted H5N1 vaccines induced a low frequency of anti-HA1 antibodies (23% and 32%, respectively) and rare anti-NA antibodies [118]. Moreover, MF59-adjuvanted H5N1 vaccine induced antibodies capable of binding long HA1 epitopes encompassing the receptor-binding domain (RBD), which is similar to those bound by broadly neutralizing antibodies [118]. In contrast, non-adjuvanted and Alum-adjuvanted vaccines mainly induced antibodies capable of binding short HA1 epitopes [118]. This study indicated that MF59 adjuvant could expand antibody repertoires to target protective HA sites and increase antibody avidities to properly folded HA1 [118]. In a different study [119], Khurana et al. found that MF59 adjuvant similarly enhanced influenza pandemic 2009 H1N1 vaccine-induced antibody diversity and affinity, more significantly expanded anti-HA1 than anti-HA2 antibodies, and induced antibodies capable of binding properly folded HA1 globular head. These studies provide important insights on how MF59 adjuvant broadens influenza vaccine-induced antibody responses against non-vaccine viral strains.
4.2. AS03
4.2.1. Cross-Clade Protection against Pre-Pandemic H5N1 Vaccine
AS03 was also incorporated in the pre-pandemic H5N1 vaccine to spare vaccine doses [125]. Chu et al. found that two doses of AS03-adjuvanted H5N1 vaccine based on clade 1 strain (A/Vietnam/1194/2004) induced a 91.4% seroconversion rate against clade 2 strain (A/Indonesia/05/2005), while the non-adjuvanted vaccine only induced a 5.6% seroconversion rate against the same clade 2 strain [120]. Langley et al. found that two doses of AS03-adjuvanted H5N1 vaccine based on clade 2 strain (A/Indonesia/05/2005) induced significant neutralizing antibody titer against clade 1 strain (A/Vietnam/1194/2004) [121]. These studies support the incorporation of AS03 adjuvant in H5N1 vaccines to induce cross-clade antibody responses following a two-dose regimen.
AS03 adjuvant was also explored in prime/boost immunizations to induce cross-clade immunity. Schwarz et al. found that heterologous prime/boost immunization of AS03-adjuvanted H5N1 vaccine based on clade 1 (A/Vietnam/1194/2004) and clade 2 (A/Indonesia/05/2005) strains induced a 92.5% seroprotection rate against the clade 2 vaccine strain and a 98.1% seroprotection rate against the clade 1 vaccine strain [122]. This study also found that heterologous prime/boost immunization was superior to homologous prime/boost immunization to induce cross-clade immunity [122]. In support, homologous prime/boost immunization of the AS03-adjuvanted H5N1 vaccine based on the clade 1 strain (A/Vietnam/1194/2004) induced an 83.3% seroprotection rate against the clade 2 strain (A/Indonesia/05/2005) if the vaccines were given 6 months apart and a 41.5-54.5% seroprotection rate against the same clade 2 strain if the vaccines were given 21 days apart [122]. In another study, Leroux-Roels et al. found that two-dose priming of the AS03-adjuvanted H5N1 vaccine based on the clade 1 strain (A/Vietnam/1194/2004) and a single dose boost of AS03-adjuvanted H5N1 vaccine based on the clade 2 strain (A/Indonesia/5/2005) could induce rapid immune responses against the clade 2 vaccine strain [123]. In contrast, non-adjuvanted vaccine priming seemed to inhibit the induction of cross-clade immune responses [123]. Sun et al. found that homologous or heterologous prime/boost immunization of AS03-adjuvanted H5N1 vaccine based on the clade 1 (A/Vietnam/1203/2004) or clade 2 strain (A/Anhui/1/2005) could induce significant heterologous protection against antigenically distinct and highly pathogenic H5N2 viruses in ferrets [126].
4.2.2. Safety
AS03-adjuvanted H5N1 vaccines were well tolerated in human subjects with no serious adverse events related to vaccination [120,121,122,123]. AS03-adjuvanted H5N1 vaccines also induced more frequent local and systemic adverse reactions than non-adjuvanted vaccines [120,121,122,123]. The most common local reaction was injection-site pain, and the most common systemic adverse reactions were myalgia and fatigue [120,121,122,123]. Most of the local and systemic adverse reactions were mild to moderate and self-resolved in days without the need for medical treatments [120,121,122,123]. It is also worth mentioning that the AS03-adjuvanted influenza pandemic 2009 H1N1 vaccine (Pandemrix) caused increased cases of narcolepsy in adolescents in Sweden and Finland 3-6 months after vaccination [127,128], while the non-adjuvanted vaccine failed to increase narcolepsy cases in the United States [129]. One study found that the HA peptide (275–287) of the pandemic virus could stimulate proliferation of hypocretin-responsive CD4+ T cells in narcolepsy patients [130]. Since the pathologic hallmark of narcolepsy is the loss of hypocretin neurons [130], immune responses against hypocretin might be responsible to the increased cases of narcolepsy following Pandemrix vaccination. Although MF59 and AS03 are both squalene emulsion-based adjuvants, the MF59-adjuvanted influenza pandemic 2009 H1N1 vaccine and seasonal influenza vaccine failed to increase narcolepsy cases [131,132]. Therefore, the unique combination of AS03 adjuvant and the pandemic influenza vaccine likely caused the increased cases of narcolepsy following Pandemrix vaccination.
4.2.3. Mechanistic Insights
Khurana et al. used whole-genome-fragment phage display libraries to map antibody-binding regions of immune sera [125]. The AS03-adjuvanted H5N1 vaccine induced 10-fold higher anti-HA2 antibodies targeting the conserved H1/H5 region and also expanded antibody repertoires against the HA1 domain, especially against the long HA1 epitopes encompassing RBD [125]. The HA1 to HA2 ratio of bound clones was increased by 7-fold with the use of AS03 adjuvant, hinting the induction of anti-HA1 dominant antibody responses [125]. The AS03-adjuvanted H5N1 vaccine also induced anti-NA antibodies targeting the C-terminal region of NA, which is close to the sialic acid binding enzymatic site [125]. The AS03-adjuvanted H5N1 vaccine also increased antibody affinity against properly folded HA1 but not HA2 domains [125]. Moris et al. found that the AS03-adjuvanted H5N1 vaccine based on the clade 1 strain (A/Vietnam/1194/2004) could induce higher levels of long-lived memory B cells and cross-reactive and polyfunctional CD4+ T cells than the non-adjuvanted vaccine in young adults (18–60 years old) [124]. Due to the crucial roles of helper CD4+ T cells in stimulating antigen-specific B cell responses [133], cross-reactive and polyfunctional CD4+ T cells might contribute to the expanded antibody repertoires and the production of broadly cross-protective antibodies following the AS03-adjuvanted H5N1 vaccination [124].
4.3. TLR4 Agonists
MPL is a TLR4 agonist and has been a major component of several licensed adjuvants (e.g., AS01 and AS04) [93,154]. Glucopyranosyl lipid adjuvant (GLA) is a synthetic TLR4 agonist, and two major formulations of GLA have been explored as vaccine adjuvants: GLA-SE (stable emulsion) and GLA-AF (aqueous formulation) [135,136,155,156,157]. Studies found that TLR4 agonist-based adjuvants could assist influenza vaccines to induce cross-protective immunity. Pillet et al. found that GLA-SE could boost the plant-derived H5-VLP vaccine to induce protective HI titer in healthy adults [134]. Furthermore, the GLA-SE-adjuvanted H5-VLP vaccine induced significant polyfunctional and sustained heterologous CD4+ T cell responses against the influenza H2 protein [134]. Clegg et al. found that GLA-AF could boost the recombinant H5N1 hemagglutinin protein (rH5) based on the clade 1 strain to induce significant HI titer against heterologous clade 1 and clade 2 viruses and confer significant protection against clade 2 viral challenges in murine models [136]. GLA-AF also boosted rH5 based on the clade 2 strain to induce significant HI titer and protection against clade 1 strain in ferrets [136]. Although the majority of adjuvants have been licensed to boost IM vaccination, GLA-AF was explored to boost ID H5N1 vaccination. Carter et al. found that GLA-AF could assist the plant-produced H5-VLP vaccine to induce -higher HI titer against heterologous H5N1 viruses in murine models [135]. Furthermore, a single dose of the ID H5-VLP vaccine based on the clade 2 strain in the presence of GLA-AF conferred complete protection against lethal challenges of clade 1 strain in ferrets [135]. In human studies, the ID H5-VLP vaccine in the presence of GLA-AF induced more potent HI titer against heterologous clade 2 strain or clade 1 strain as compared to the IM H5-VLP vaccine in the presence of the same adjuvant or ID H5-VLP vaccine alone [135]. This study indicated that properly stimulated dermal APCs had a better ability than IM APCs to induce cross-protective immune responses [135]. Ko et al. found that a combination of MPL and CpG adjuvants could assist the influenza pandemic 2009 H1N1 vaccine to induce cross-protective immune responses against heterosubtypic H5N1 viruses in murine models [136]. Goff et al. found that a combination of synthetic TLR4 and TLR7 agonists could assist rHA or chimeric rHA to induce significant cross-protection against heterologous and heterosubtypic viruses in murine models [138]. Furthermore, the heterosubtypic protection was mainly due to the broadly cross-protective antibodies against HA stalks [138].
4.4. TLR7 Agonists
Imiquimod is a synthetic TLR7 agonist, and its topical 5% cream (Aldara) has been approved to treat genital warts, basal cell carcinoma, and actinic keratosis [158]. Topical imiquimod treatment (Aldara) followed by ID TIV was found to induce much higher seroconversion rates against all vaccine strains than ID TIV alone in young healthy adults [139]. Topical imiquimod followed by ID TIV also induced significant seroconversion against non-vaccine viral strains such as the antigenically drifted H3N2 strain [139]. 3M-052 was a synthesized TLR7 agonist containing an 18-carbon chain to limit its systemic distribution and induce more prominent local adjuvant effects [140]. Hoeven et al. found that one dose of rHA (H5N1, A/Vietnam/1203/04) in the presence of 3M-052 in stable emulsions induced 100% protection against homologous viral challenges in murine and ferret models, while rHA alone only induced partial protection [140]. Furthermore, rHA in the presence of 3M-052 in stable emulsions or liposomes induced significant neutralizing antibodies against clade 2 strains [140].
4.5. Flagellin
Flagellin is the major structural protein of bacterial flagellum and contains four domains (D0, D1, D2, and D3) [159]. D0/D1 domains are comprised of highly conserved N- and C-termini of flagellin [159]. D2/D3 domains are composed of highly variable internal region of flagellin [159]. Extracellular flagellin can be recognized by TLR5, and intracellular flagellin can be recognized by the cytosolic NLR family caspase recruitment domain (CARD)-containing protein 4 (NLRC4) inflammasome [160,161]. The D1 domain contributes to TLR5 binding [159,162,163], while the D0 domain contributes to NLRC4 inflammasome activation [164]. Foreign antigens can replace the highly variable D3 domain of flagellin or insert to its N or C-terminus without affecting its TLR5 activation ability [161]. Flagellin has been broadly explored as a highly immunogenic carrier for vaccine development against bacterial, viral, parasitic diseases, and cancer [161]. Wang et al. produced influenza PR8 HA-displayed M1 VLPs (HA/M1 VLPs) incorporating membrane-anchored flagellin (flagellin/HA/M1 VLPs) and found that the IM immunization of flagellin/HA/M1 VLPs could induce significant protection against heterosubtypic H3N2 viruses in murine models [141]. Due to the strong induction of respiratory epithelial cells with TLR5 expression to release cytokines and chemokines [161], flagellin has been also explored as a mucosal adjuvant [160]. Wang et al. found that IN immunization of flagellin/HA/M1 VLPs induced complete protection against heterosubtypic H3N2 viral challenges in murine models, while HA/M1 VLPs alone or in the presence of soluble flagellin showed little or no protection [142]. The above two studies indicated the importance of co-delivery of flagellin and HA/M1 VLPs in the induction of heterosubtypic immunity.
4.6. Saponin-containing Adjuvants
QS-21 is a highly purified saponin product from the bark extract of the South American tree, Quillaja saponaria Molina [165,166]. QS-21 has potent vaccine adjuvant effects if used alone at high doses [165]. Yet, a high-dose of QS-21 has the risk of inducing hemolysis in humans [165]. To improve its safety, QS-21 has been formulated with MPL in several adjuvant systems [93,167]. Other saponin-containing adjuvants have been also developed. Immunostimulating complexes (ISCOMs) are particulate antigen delivery systems comprised of vaccine antigens, phospholipids, cholesterol, and saponin [168,169]. ISCOMs are able to augment vaccine-induced humoral and cellular immune responses [168,170,171]. ISCOMs were explored to boost influenza vaccination and induce cross-protective immunity. Sambhara et al. found that ISCOMs could significantly increase H1N1 vaccine-induced HI titer and fully protect mice from heterosubtypic H2N2 viral challenges [143]. Further studies found that ISCOMs-induced heterosubtypic protection was correlated with CTL responses against a shared major histocompatibility complex (MHC) I epitope within HA of influenza H1 and H2 viruses [143]. ISCOM technology-based Matrix-M adjuvant was found to significantly increase trivalent virosomal vaccine-induced HI titer and protection against heterologous influenza type B but not type A viruses [144]. Matrix-M adjuvant also significantly increased HA nanoparticle-induced HI titer and protection against drifted H3N2 viruses in ferrets [145]. In another study, Cox et al. found that the Matrix-M-adjuvanted trivalent virosomal vaccine induced cross-protective immunity against highly pathogenic H5N1 and H7N7 viruses in mice and ferrets [146]. In addition to the seasonal influenza vaccine, the Matrix-M-adjuvanted virosomal H5N1 vaccine induced significant MN antibody titer against heterologous viruses in human subjects [147].
4.7. Enterotoxin Adjuvants
Cholera toxin (CT) of various strains of Vibrio cholerae, heat-labile enterotoxin (LT) of enterotoxigenic E. Coli, and their derivatives are the mostly studied mucosal adjuvants [172]. CT and LT belong to AB5 toxins composed of one A and five B subunits [172,173]. The A subunit catalyzes specific targets and is responsible for cell toxicity [172,173]. The B subunit forms a five-membered ring structure capable of binding to GM1-ganglioside receptors on target cells [172,173]. Quan et al. found that CT could significantly increase IN whole-inactivated PR8 (PR8i) vaccine-induced HI titer against heterologous and heterosubtypic viruses in murine models [148]. The CT-adjuvanted PR8i vaccine was found to confer complete protection against heterosubtypic H3N2 viruses, while the PR8i vaccine alone induced partial protection [148]. Furthermore, the heterosubtypic protection was mainly due to cross-reactive antibodies but not CD4+ or CD8+ T cells [148]. In an earlier study, Tamura et al. found that the CT B subunit (CTB) could significantly increase IN TIV-induced cross-protection against a drifted virus in murine models, while subcutaneous delivery of the same vaccine failed to induce similar levels of cross-protection [149]. An LT-adjuvanted influenza vaccine was approved for IN delivery in Switzerland (Nasalflu, Berna Biotech) during the 2000-2001 flu season [174]. However, it was pulled off the market due to the 19-fold increased risks of Bell’s palsy or facial paralysis in vaccine recipients [174]. Therefore, different LT mutants were developed to reduce the enterotoxicity of LT-based adjuvants, such as single-mutant LT (R192G) and double-mutant LT (R192G/L211A) [175,176]. Tumpey et al. found that the IN H3N2 vaccine in the presence of LT (R192G) adjuvant conferred complete protection against highly pathogenic H5N1 viruses in murine models, while the IN vaccine alone induced partial protection [150]. Furthermore, a subcutaneous vaccine in the presence of LT (R192G) or incomplete Freund’s adjuvant failed to confer protection against lethal H5N1 viral challenges [150]. B cells rather than CD8+ T cells were vital for the heterosubtypic protection [150].
4.8. CAF01
CAF01 is a two-component adjuvant comprised of cationic liposome dimethyl dioctadecyl ammonium bromide (DDA) and an immunomodulator trehalose 6,6′-dibeheneate (TDB) [177]. DDA is a quaternary ammonium compound comprised of one positively charged hydrophilic head and two hydrophobic 18-carbon tails and can self-assemble into liposome structures [178]. TDB is a glycolipid that is used to increase the stability and adjuvant effects of DDA liposomes [178]. Rosenkrands et al. found that the CAF01 adjuvant could significantly enhance TIV-induced humoral and cellular immune responses in BALB/c mice [151]. Furthermore, CAF01-adjuvanted TIV induced complete protection against heterologous H1N1 viral challenges, while TIV alone induced partial protection [151]. Christensen et al. found that CAF01 adjuvant significantly enhanced TIV-induced HI titer against homologous but not heterologous H1N1 viruses in ferrets [152]. Yet, CAF01-adjuvanted TIV more significantly reduced viral load and fever after heterologous H1N1 viral challenges as compared to TIV alone [152]. This study indicated that CAF01-adjuvanted TIV induced HI-independent cross-protective mechanisms in ferrets [152].
4.9. Physical Adjuvants
As an alternative to chemical adjuvants, physical adjuvants have been also explored to boost vaccination without introducing any chemicals or biological molecules into the body. Physical adjuvants utilize physical energies (e.g., laser, radiofrequency) to stimulate skin stress and alert innate immune systems to boost ID or transdermal vaccination. Due to the brief application of non-invasive or minimally invasive physical energies, physical adjuvants often induce minimal local or systemic adverse reactions and are less likely to induce long-term side effects. Laser adjuvants have been the mostly explored physical adjuvants so far and have been explored to boost influenza, nicotine, and cancer vaccination in preclinical animal models [179,180,181,182,183,184]. A near-infrared laser adjuvant was recently advanced to the clinical test and was found to stimulate significant cutaneous immune cell trafficking with good safety and tolerability in humans [185]. The intentional induction of microscopic photothermal damage by non-ablative fractional laser (NAFL) was found to safely boost ID influenza vaccination in murine models [186]. Interestingly, the NAFL significantly increased dissolving microneedle-based PR8i vaccine-induced immune responses and cross-protection against heterologous influenza H1N1 and H3N2 viruses in murine models [153]. We recently explored the use of radiofrequency energy to boost ID influenza vaccination and found that the radiofrequency adjuvant (RFA) could simultaneously augment influenza vaccine-induced humoral and cellular immune responses in murine models [187]. The RFA effects were comparable to MF59-like AddaVax adjuvant at 0.3 µg vaccine dose and superior to AddaVax adjuvant at 0.06 µg vaccine dose [187]. We recently found that the RFA-adjuvanted influenza pandemic 2009 H1N1 vaccine could induce heterologous protection against PR8 viruses, while the vaccine alone failed to induce heterologous protection in murine models (Li et al., manuscript in preparation).
5. Conclusions
Seasonal and pandemic influenza pose a huge threat to global public health. Current influenza vaccines mainly induce strain-specific protection. Better influenza vaccines are highly demanded to induce cross-protective immunity. In addition to the development of universal influenza vaccines, the incorporation of vaccine adjuvants into current influenza vaccines represents an attractive approach to induce cross-protective immunity. Squalene emulsion-based MF59 and AS03 adjuvants have been used to boost seasonal influenza vaccine efficacy in the elderly or spare pre-pandemic or pandemic influenza vaccine doses. MF59 and AS03 adjuvants have been found to also broaden influenza vaccine-induced immune responses against non-vaccine viral strains in human subjects. Different types of experimental adjuvants have been found to also assist current influenza vaccines to induce cross-protective immunity. Vaccine adjuvants hold a great promise to adjuvant current influenza vaccines to induce cross-protective immunity.
Author Contributions
X.C. conceived the review; X.C., Z.L., Y.L., and Y.Z. wrote the manuscript; X.C. edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work is supported by the National Institutes of Health grant AI139473 (to X.Y.C.).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interests.
References
- Clayville, L.R. Influenza update: A review of currently available vaccines. P & T 2011, 36, 659–684. [Google Scholar]
- Bouvier, N.M.; Palese, P. The biology of influenza viruses. Vaccine 2008, 26 (Suppl. 4), D49–D53. [Google Scholar] [CrossRef] [Green Version]
- Petrova, V.N.; Russell, C.A. The evolution of seasonal influenza viruses. Nat. Rev. Microbiol. 2018, 16, 47–60. [Google Scholar] [CrossRef]
- Long, J.S.; Mistry, B.; Haslam, S.M.; Barclay, W.S. Host and viral determinants of influenza A virus species specificity. Nat. Rev. Microbiol. 2019, 17, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Taubenberger, J.K.; Kash, J.C. Influenza virus evolution, host adaptation, and pandemic formation. Cell Host Microbe 2010, 7, 440–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodewes, R.; Morick, D.; De Mutsert, G.; Osinga, N.; Bestebroer, T.; Van Der Vliet, S.; Smits, S.L.; Kuiken, T.; Rimmelzwaan, G.F.; Fouchier, R.A.; et al. Recurring influenza B virus infections in seals. Emerg. Infect Dis. 2013, 19, 511–512. [Google Scholar] [CrossRef] [PubMed]
- Boivin, S.; Cusack, S.; Ruigrok, R.W.; Hart, D.J. Influenza A virus polymerase: Structural insights into replication and host adaptation mechanisms. J. Biol. Chem. 2010, 285, 28411–28417. [Google Scholar] [CrossRef] [Green Version]
- Nobusawa, E.; Sato, K. Comparison of the mutation rates of human influenza A and B viruses. J. Virol. 2006, 80, 3675–3678. [Google Scholar] [CrossRef] [Green Version]
- Shao, W.; Li, X.; Goraya, M.U.; Wang, S.; Chen, J.L. Evolution of Influenza A Virus by Mutation and Re-Assortment. Int. J. Mol. Sci. 2017, 18, 1650. [Google Scholar] [CrossRef] [Green Version]
- Wu, N.C.; Wilson, I.A. A Perspective on the Structural and Functional Constraints for Immune Evasion: Insights from Influenza Virus. J. Mol. Biol. 2017, 429, 2694–2709. [Google Scholar] [CrossRef]
- Taubenberger, J.K.; Morens, D.M. Pandemic influenza--including a risk assessment of H5N1. Rev. Sci. Tech. 2009, 28, 187–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowen, A.C. Constraints, Drivers, and Implications of Influenza A Virus Reassortment. Annu. Rev. Virol. 2017, 4, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, E.D. Influenza pandemics of the 20th century. Emerg. Infect Dis. 2006, 12, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Rambhia, K.J.; Watson, M.; Sell, T.K.; Waldhorn, R.; Toner, E. Mass vaccination for the 2009 H1N1 pandemic: Approaches, challenges, and recommendations. Biosecur. Bioterror. 2010, 8, 321–330. [Google Scholar] [CrossRef]
- Taubenberger, J.K.; Kash, J.C.; Morens, D.M. The 1918 influenza pandemic: 100 years of questions answered and unanswered. Sci. Transl. Med. 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Saunders-Hastings, P.R.; Krewski, D. Reviewing the History of Pandemic Influenza: Understanding Patterns of Emergence and Transmission. Pathogens 2016, 5, 66. [Google Scholar] [CrossRef] [Green Version]
- Fineberg, H.V. Pandemic preparedness and response—Lessons from the H1N1 influenza of 2009. N. Engl. J. Med. 2014, 370, 1335–1342. [Google Scholar] [CrossRef] [Green Version]
- Trifonov, V.; Khiabanian, H.; Rabadan, R. Geographic dependence, surveillance, and origins of the 2009 influenza A (H1N1) virus. N. Engl. J. Med. 2009, 361, 115–119. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.S.; Webby, R.J. Traditional and new influenza vaccines. Clin. Microbiol. Rev. 2013, 26, 476–492. [Google Scholar] [CrossRef] [Green Version]
- Tosh, P.K.; Jacobson, R.M.; Poland, G.A. Influenza vaccines: From surveillance through production to protection. Mayo Clin. Proc. 2010, 85, 257–273. [Google Scholar] [CrossRef] [Green Version]
- Paules, C.I.; Sullivan, S.G.; Subbarao, K.; Fauci, A.S. Chasing Seasonal Influenza-The Need for a Universal Influenza Vaccine. N. Engl. J. Med. 2018, 378, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Berlanda Scorza, F.; Tsvetnitsky, V.; Donnelly, J.J. Universal influenza vaccines: Shifting to better vaccines. Vaccine 2016, 34, 2926–2933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estrada, L.D.; Schultz-Cherry, S. Development of a Universal Influenza Vaccine. J. Immunol. 2019, 202, 392–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, P.T.; Crépey, P.; Pitman, R.J.; Macabeo, B.; Chit, A.; Postma, M.J. Cost-Effectiveness of Quadrivalent versus Trivalent Influenza Vaccine in the United States. Value Health 2016, 19, 964–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrose, C.S.; Levin, M.J. The rationale for quadrivalent influenza vaccines. Hum. Vaccines Immunother. 2012, 8, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Soema, P.C.; Kompier, R.; Amorij, J.P.; Kersten, G.F. Current and next generation influenza vaccines: Formulation and production strategies. Eur. J. Pharm. Biopharm. Off. J. Arb. Fur Pharm. Verfahr. E.V 2015, 94, 251–263. [Google Scholar] [CrossRef] [Green Version]
- Huckriede, A.; Bungener, L.; Stegmann, T.; Daemen, T.; Medema, J.; Palache, A.M.; Wilschut, J.C. The virosome concept for influenza vaccines. Vaccine 2005, 23 (Suppl. 1), S26–S38. [Google Scholar] [CrossRef]
- Herzog, C.; Hartmann, K.; Künzi, V.; Kürsteiner, O.; Mischler, R.; Lazar, H.; Glück, R. Eleven years of Inflexal V-a virosomal adjuvanted influenza vaccine. Vaccine 2009, 27, 4381–4387. [Google Scholar] [CrossRef]
- Chen, J.R.; Liu, Y.M.; Tseng, Y.C.; Ma, C. Better influenza vaccines: An industry perspective. J. Biomed. Sci. 2020, 27, 33. [Google Scholar] [CrossRef]
- Kon, T.C.; Onu, A.; Berbecila, L.; Lupulescu, E.; Ghiorgisor, A.; Kersten, G.F.; Cui, Y.-Q.; Amorij, J.-P.; Van Der Pol, L. Influenza Vaccine Manufacturing: Effect of Inactivation, Splitting and Site of Manufacturing. Comparison of Influenza Vaccine Production Processes. PLoS ONE 2016, 11, e0150700. [Google Scholar] [CrossRef] [Green Version]
- Milián, E.; Kamen, A.A. Current and Emerging Cell Culture Manufacturing Technologies for Influenza Vaccines. Biomed. Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamayoshi, S.; Kawaoka, Y. Current and future influenza vaccines. Nat. Med. 2019, 25, 212–220. [Google Scholar] [CrossRef]
- Cox, M.M.; Izikson, R.; Post, P.; Dunkle, L. Safety, efficacy, and immunogenicity of Flublok in the prevention of seasonal influenza in adults. Adv. Vaccines 2015, 3, 97–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, H.J. Alternative routes of influenza vaccine delivery. Expert. Opin. Drug Deliv. 2006, 3, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Amorij, J.P.; Hinrichs, W.; Frijlink, H.W.; Wilschut, J.C.; Huckriede, A. Needle-free influenza vaccination. Lancet Infect Dis. 2010, 10, 699–711. [Google Scholar] [CrossRef]
- McAllister, L.; Anderson, J.; Werth, K.; Cho, I.; Copeland, K.; Bouveret, N.L.C.; Plant, D.; Mendelman, P.M.; Cobb, D.K. Needle-free jet injection for administration of influenza vaccine: A randomised non-inferiority trial. Lancet (Lond. Engl.) 2014, 384, 674–681. [Google Scholar] [CrossRef]
- Ravi, A.D.; Sadhna, D.; Nagpaal, D.; Chawla, L. Needle free injection technology: A complete insight. Int. J. Pharm. Investig. 2015, 5, 192–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kis, E.E.; Winter, G.; Myschik, J. Devices for intradermal vaccination. Vaccine 2012, 30, 523–538. [Google Scholar] [CrossRef]
- Romani, N.; Flacher, V.; Tripp, C.H.; Sparber, F.; Ebner, S.; Stoitzner, P. Targeting Skin Dendritic Cells to Improve Intradermal Vaccination. Curr. Top. Microbiol. Immunol. 2011, 351, 113–138. [Google Scholar] [CrossRef] [Green Version]
- Sticchi, L.; Alberti, M.; Alicino, C.; Crovari, P. The intradermal vaccination: Past experiences and current perspectives. J. Prev. Med. Hyg. 2010, 51, 7–14. [Google Scholar]
- Icardi, G.; Orsi, A.; Ceravolo, A.; Ansaldi, F. Current evidence on intradermal influenza vaccines administered by Soluvia licensed micro injection system. Hum. Vaccin. Immunother. 2012, 8, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Levin, Y.; Kochba, E.; Hung, I.; Kenney, R. Intradermal vaccination using the novel microneedle device MicronJet600: Past, present, and future. Hum. Vaccines Immunother. 2015, 11, 991–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Who Writing Group; Ampofo, W.K.; Baylor, N.; Cobey, S.; Cox, N.J.; Daves, S.; Edwards, S.; Ferguson, N.; Grohmann, G.; Hay, A.; et al. Improving influenza vaccine virus selection: Report of a WHO informal consultation held at WHO headquarters, Geneva, Switzerland, 14-16 June 2010. Influenza Other Respir. Viruses 2012, 6, 142–152, e141–e145. [Google Scholar] [CrossRef] [Green Version]
- Jennings, L.C.; Monto, A.S.; Chan, P.K.; Szucs, T.D.; Nicholson, K.G. Stockpiling prepandemic influenza vaccines: A new cornerstone of pandemic preparedness plans. Lancet Infect. Dis. 2008, 8, 650–658. [Google Scholar] [CrossRef]
- Poovorawan, Y.; Pyungporn, S.; Prachayangprecha, S.; Makkoch, J. Global alert to avian influenza virus infection: From H5N1 to H7N9. Pathog. Glob. Health 2013, 107, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichol, K.L.; Treanor, J.J. Vaccines for seasonal and pandemic influenza. J. Infect. Dis. 2006, 194 (Suppl. 2), S111–S118. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, E.; Qiu, X.; Wilson, P.C.; Bahl, J.; Krammer, F. The influenza virus hemagglutinin head evolves faster than the stalk domain. Sci. Rep. 2018, 8, 10432. [Google Scholar] [CrossRef]
- Raymond, D.D.; Bajic, G.; Ferdman, J.; Suphaphiphat, P.; Settembre, E.C.; Moody, M.A.; Schmidt, A.G.; Harrison, S.C. Conserved epitope on influenza-virus hemagglutinin head defined by a vaccine-induced antibody. Proc. Natl. Acad. Sci. USA 2018, 115, 168–173. [Google Scholar] [CrossRef] [Green Version]
- Wiley, D.C.; Skehel, J.J. The structure and function of the hemagglutinin membrane glycoprotein of influenza virus. Annu. Rev. Biochem. 1987, 56, 365–394. [Google Scholar] [CrossRef]
- Mair, C.M.; Ludwig, K.; Herrmann, A.; Sieben, C. Receptor binding and pH stability-how influenza A virus hemagglutinin affects host-specific virus infection. Biochim. Biophys. Acta 2014, 1838, 1153–1168. [Google Scholar] [CrossRef] [Green Version]
- Xie, H.; Wan, X.-F.; Ye, Z.; Plant, E.P.; Zhao, Y.; Xu, Y.; Li, X.; Finch, C.; Zhao, N.; Kawano, T.; et al. H3N2 Mismatch of 2014-15 Northern Hemisphere Influenza Vaccines and Head-to-head Comparison between Human and Ferret Antisera derived Antigenic Maps. Sci. Rep. 2015, 5, 15279. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, R.K.; Nowalk, M.P.; Chung, J.; Jackson, M.L.; Jackson, L.A.; Petrie, J.G.; Monto, A.S.; McLean, H.Q.; Belongia, E.A.; Gaglani, M.; et al. 2014-2015 Influenza Vaccine Effectiveness in the United States by Vaccine Type. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, 1564–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belongia, E.A.; Kieke, B.A.; Donahue, J.G.; Greenlee, R.T.; Balish, A.; Foust, A.; Lindstrom, S.; Shay, D.K.; Marshfield Influenza Study Group. Effectiveness of inactivated influenza vaccines varied substantially with antigenic match from the 2004-2005 season to the 2006–2007 season. J. Infect. Dis. 2009, 199, 159–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Z.; Jiao, X.; Liu, X. Antibody Immunity Induced by H7N9 Avian Influenza Vaccines: Evaluation Criteria, Affecting Factors, and Implications for Rational Vaccine Design. Front. Microbiol. 2017, 8, 1898. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, P.; Pei, Y.; Tsang, T.K.; Gu, D.; Wang, W.; Zhang, J.; Horby, P.W.; Uyeki, T.M.; Cowling, B.J.; et al. Assessment of Human-to-Human Transmissibility of Avian Influenza A(H7N9) Virus Across 5 Waves by Analyzing Clusters of Case Patients in Mainland China, 2013-2017. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 68, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Baz, M.; Luke, C.J.; Cheng, X.; Jin, H.; Subbarao, K. H5N1 vaccines in humans. Virus Res. 2013, 178, 78–98. [Google Scholar] [CrossRef] [Green Version]
- Clegg, C.H.; Rininger, J.A.; Baldwin, S.L. Clinical vaccine development for H5N1 influenza. Expert Rev. Vaccines 2013, 12, 767–777. [Google Scholar] [CrossRef]
- Mulligan, M.J.; I Bernstein, D.; Winokur, P.L.; E Rupp, R.; Anderson, E.; Rouphael, N.; Dickey, M.; Stapleton, J.T.; Edupuganti, S.; Spearman, P.; et al. Serological responses to an avian influenza A/H7N9 vaccine mixed at the point-of-use with MF59 adjuvant: A randomized clinical trial. JAMA 2014, 312, 1409–1419. [Google Scholar] [CrossRef] [Green Version]
- Koutsakos, M.; Kedzierska, K.; Subbarao, K. Immune Responses to Avian Influenza Viruses. J. Immunol. 2019, 202, 382–391. [Google Scholar] [CrossRef] [Green Version]
- El Sahly, H.M.; Keitel, W.A. Pandemic H5N1 influenza vaccine development: An update. Expert Rev. Vaccines 2008, 7, 241–247. [Google Scholar] [CrossRef]
- Guan, Y.; Smith, G.J.; Webby, R.; Webster, R.G. Molecular epidemiology of H5N1 avian influenza. Rev. Sci. Tech. 2009, 28, 39–47. [Google Scholar] [CrossRef]
- Lu, J.; Raghwani, J.; Pryce, R.; Bowden, T.A.; Thézé, J.; Huang, S.; Song, Y.; Zou, L.; Liang, L.; Bai, R.; et al. Molecular Evolution, Diversity, and Adaptation of Influenza A(H7N9) Viruses in China. Emerg. Infect Dis. 2018, 24, 1795–1805. [Google Scholar] [CrossRef]
- Kwon, H.-I.; Kim, Y.-I.; Park, S.-J.; Song, M.-S.; Kim, E.-H.; Kim, S.M.; Si, Y.-J.; Lee, I.-W.; Song, B.-M.; Lee, Y.-J.; et al. Evaluation of the Immune Responses to and Cross-Protective Efficacy of Eurasian H7 Avian Influenza Viruses. J. Virol. 2017, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrovsky, N.; Aguilar, J.C. Vaccine adjuvants: Current state and future trends. Immunol. Cell Biol. 2004, 82, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Di Pasquale, A.; Preiss, S.; Tavares Da Silva, F.; Garcon, N. Vaccine Adjuvants: From 1920 to 2015 and Beyond. Vaccines 2015, 3, 320–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coffman, R.L.; Sher, A.; Seder, R.A. Vaccine adjuvants: Putting innate immunity to work. Immunity 2010, 33, 492–503. [Google Scholar] [CrossRef] [Green Version]
- Gavillet, B.M.; Ahmed, S.; Egan, W.M.; Del Giudice, G.; Golding, H.; Gust, I.; Neels, P.; Reed, S.G.; Sheets, R.L.; Siegrist, C.; et al. Mode of action of adjuvants: Implications for vaccine safety and design. Biologicals 2010, 38, 594–601. [Google Scholar] [CrossRef]
- Rizza, P.; Ferrantini, M.; Capone, I.; Belardelli, F. Cytokines as natural adjuvants for vaccines: Where are we now? Trends Immunol. 2002, 23, 381–383. [Google Scholar] [CrossRef]
- McKee, A.S.; Marrack, P. Old and new adjuvants. Curr. Opin. Immunol. 2017, 47, 44–51. [Google Scholar] [CrossRef]
- Kool, M.; Fierens, K.; Lambrecht, B.N. Alum adjuvant: Some of the tricks of the oldest adjuvant. J. Med. Microbiol. 2012, 61, 927–934. [Google Scholar] [CrossRef] [Green Version]
- HogenEsch, H.; O’Hagan, D.T.; Fox, C.B. Optimizing the utilization of aluminum adjuvants in vaccines: You might just get what you want. Npj Vaccines 2018, 3, 51. [Google Scholar] [CrossRef]
- Lindblad, E.B. Aluminium compounds for use in vaccines. Immunol. Cell Biol. 2004, 82, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Powers, D.C.; Smith, G.E.; Anderson, E.L.; Kennedy, D.J.; Hackett, C.S.; Wilkinson, B.E.; Volvovitz, F.; Belshe, R.B.; Treanor, J.J. Influenza A virus vaccines containing purified recombinant H3 hemagglutinin are well tolerated and induce protective immune responses in healthy adults. J. Infect. Dis. 1995, 171, 1595–1599. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, H.J.; Müller, M.; Oh, H.M.; Tambyah, P.A.; Joukhadar, C.; Montomoli, E.; Fisher, D.; Berezuk, G.; Fritsch, S.; Löw-Baselli, A.; et al. A clinical trial of a whole-virus H5N1 vaccine derived from cell culture. N. Engl. J. Med. 2008, 358, 2573–2584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.J.; Shih, Y.J.; Chen, C.H.; Fang, C.T. Aluminum salts as an adjuvant for pre-pandemic influenza vaccines: A meta-analysis. Sci. Rep. 2018, 8, 11460. [Google Scholar] [CrossRef]
- Yin, D.P.; Zhu, B.P.; Wang, H.Q.; Cao, L.; Di Wu, W.; Jiang, K.Y.; Xia, W.; Zhang, G.M.; Zheng, J.-S.; Cao, L.S.; et al. Effect of aluminum hydroxide adjuvant on the immunogenicity of the 2009 pandemic influenza A/H1N1 vaccine: Multi-level modeling of data with repeated measures. Biomed. Env. Sci. 2011, 24, 624–629. [Google Scholar] [CrossRef]
- Hutchison, S.; Benson, R.A.; Gibson, V.B.; Pollock, A.H.; Garside, P.; Brewer, J.M. Antigen depot is not required for alum adjuvanticity. FASEB J. 2012, 26, 1272–1279. [Google Scholar] [CrossRef] [Green Version]
- Kool, M.; Soullié, T.; van Nimwegen, M.; Willart, M.A.; Muskens, F.; Jung, S.; Hoogsteden, H.C.; Hammad, H.; Lambrecht, B.N. Alum adjuvant boosts adaptive immunity by inducing uric acid and activating inflammatory dendritic cells. J. Exp. Med. 2008, 205, 869–882. [Google Scholar] [CrossRef] [Green Version]
- Eisenbarth, S.C.; Colegio, O.R.; O’Connor, W.; Sutterwala, F.S.; Flavell, R.A. Crucial role for the Nalp3 inflammasome in the immunostimulatory properties of aluminium adjuvants. Nature 2008, 453, 1122–1126. [Google Scholar] [CrossRef]
- Li, H.; Willingham, S.B.; Ting, J.P.; Re, F. Cutting edge: Inflammasome activation by alum and alum’s adjuvant effect are mediated by NLRP3. J. Immunol. 2008, 181, 17–21. [Google Scholar] [CrossRef] [Green Version]
- Kool, M.; Pétrilli, V.; De Smedt, T.; Rolaz, A.; Hammad, H.; Van Nimwegen, M.; Bergen, I.M.; Castillo, R.; Lambrecht, B.N.; Tschopp, J. Cutting edge: Alum adjuvant stimulates inflammatory dendritic cells through activation of the NALP3 inflammasome. J. Immunol. 2008, 181, 3755–3759. [Google Scholar] [CrossRef] [Green Version]
- Franchi, L.; Nunez, G. The Nlrp3 inflammasome is critical for aluminium hydroxide-mediated IL-1beta secretion but dispensable for adjuvant activity. Eur. J. Immunol. 2008, 38, 2085–2089. [Google Scholar] [CrossRef]
- Wen, Y.; Shi, Y. Alum: An old dog with new tricks. Emerg. Microbes Infect 2016, 5, e25. [Google Scholar] [CrossRef] [PubMed]
- Marrack, P.; McKee, A.S.; Munks, M.W. Towards an understanding of the adjuvant action of aluminium. Nat. Rev. Immunol. 2009, 9, 287–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Hagan, D.T.; Tsai, T.F.; Brito, L.A. Emulsion based vaccine adjuvants. Hum. Vaccin. Immunother. 2013, 9, 1698–1700. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.F. Fluad(R)-MF59(R)-Adjuvanted Influenza Vaccine in Older Adults. Infect Chemother 2013, 45, 159–174. [Google Scholar] [CrossRef] [Green Version]
- O’Hagan, D.T.; Ott, G.S.; Nest, G.V.; Rappuoli, R.; Giudice, G.D. The history of MF59((R)) adjuvant: A phoenix that arose from the ashes. Expert Rev. Vaccines 2013, 12, 13–30. [Google Scholar] [CrossRef]
- Weir, J.P.; Gruber, M.F. An overview of the regulation of influenza vaccines in the United States. Influenza Other Respir. Viruses 2016, 10, 354–360. [Google Scholar] [CrossRef] [Green Version]
- Schaffner, W.; Chen, W.H.; Hopkins, R.H.; Neuzil, K. Effective Immunization of Older Adults against Seasonal Influenza. Am. J. Med. 2018, 131, 865–873. [Google Scholar] [CrossRef]
- Wilkins, A.L.; Kazmin, D.; Napolitani, G.; Clutterbuck, E.A.; Pulendran, B.; Siegrist, C.-A.; Pollard, A.J. AS03- and MF59-Adjuvanted Influenza Vaccines in Children. Front. Immunol. 2017, 8, 1760. [Google Scholar] [CrossRef] [Green Version]
- Jackson, L.A.; Campbell, J.D.; Frey, S.E.; Edwards, K.M.; Keitel, W.A.; Kotloff, K.L.; Berry, A.A.; Atmar, R.L.; Creech, C.B.; Thomsen, I.P.; et al. Effect of Varying Doses of a Monovalent H7N9 Influenza Vaccine With and Without AS03 and MF59 Adjuvants on Immune Response: A Randomized Clinical Trial. JAMA 2015, 314, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, D.I.; Edwards, K.M.; Dekker, C.L.; Belshe, R.; Talbot, H.K.B.; Graham, I.L.; Noah, D.L.; He, F.; Hill, H. Effects of adjuvants on the safety and immunogenicity of an avian influenza H5N1 vaccine in adults. J. Infect. Dis. 2008, 197, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Garcon, N.; Di Pasquale, A. From discovery to licensure, the Adjuvant System story. Hum. Vaccines Immunother. 2017, 13, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Laupeze, B.; Herve, C.; Di Pasquale, A.; Tavares Da Silva, F. Adjuvant Systems for vaccines: 13years of post-licensure experience in diverse populations have progressed the way adjuvanted vaccine safety is investigated and understood. Vaccine 2019, 37, 5670–5680. [Google Scholar] [CrossRef]
- Di, M.S.; Basevi, V.; Borsari, S.; Balduzzi, S.; Magrini, N. Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine. Lancet Oncol. 2012, 13, e50. [Google Scholar] [CrossRef]
- Garcon, N.; Morel, S.; Didierlaurent, A.; Descamps, D.; Wettendorff, M.; Van Mechelen, M. Development of an AS04-adjuvanted HPV vaccine with the adjuvant system approach. BioDrugs 2011, 25, 217–226. [Google Scholar] [CrossRef]
- Thompson, B.S.; Chilton, P.M.; Ward, J.R.; Evans, J.T.; Mitchell, T.C. The low-toxicity versions of LPS, MPL adjuvant and RC529, are efficient adjuvants for CD4+ T cells. J. Leukoc. Biol. 2005, 78, 1273–1280. [Google Scholar] [CrossRef]
- Brito, L.A.; Malyala, P.; O’Hagan, D.T. Vaccine adjuvant formulations: A pharmaceutical perspective. Semin. Immunol. 2013, 25, 130–145. [Google Scholar] [CrossRef]
- Garcon, N.; Vaughn, D.W.; Didierlaurent, A.M. Development and evaluation of AS03, an Adjuvant System containing alpha-tocopherol and squalene in an oil-in-water emulsion. Expert Rev. Vaccines 2012, 11, 349–366. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Russell, R.F.; Kinnear, E. Adjuvanted influenza vaccines. Hum. Vaccines Immunother. 2018, 14, 550–564. [Google Scholar] [CrossRef] [Green Version]
- Johansen, K.; Nicoll, A.; Ciancio, B.C.; Kramarz, P. Pandemic influenza A(H1N1) 2009 vaccines in the European Union. Euro Surveill 2009, 14, 19361. [Google Scholar] [PubMed]
- Leroux-Roels, G. Prepandemic H5N1 influenza vaccine adjuvanted with AS03: A review of the pre-clinical and clinical data. Expert Opin. Biol. 2009, 9, 1057–1071. [Google Scholar] [CrossRef] [PubMed]
- Garcon, N.; Chomez, P.; Van Mechelen, M. GlaxoSmithKline Adjuvant Systems in vaccines: Concepts, achievements and perspectives. Expert Rev. Vaccines 2007, 6, 723–739. [Google Scholar] [CrossRef] [PubMed]
- Garcon, N.; Van Mechelen, M. Recent clinical experience with vaccines using MPL- and QS-21-containing adjuvant systems. Expert Rev. Vaccines 2011, 10, 471–486. [Google Scholar] [CrossRef] [PubMed]
- Gosling, R.; von Seidlein, L. The Future of the RTS,S/AS01 Malaria Vaccine: An Alternative Development Plan. PLoS Med. 2016, 13, e1001994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Didierlaurent, A.M.; Laupèze, B.; Di Pasquale, A.; Hergli, N.; Collignon, C.; Garçon, N. Adjuvant system AS01: Helping to overcome the challenges of modern vaccines. Expert Rev. Vaccines 2017, 16, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.D. Development of the CpG Adjuvant 1018: A Case Study. Methods Mol. Biol. 2017, 1494, 15–27. [Google Scholar] [CrossRef]
- Schillie, S.H.A.; Link-Gelles, R.; Romero, J.; Ward, J.; Nelson, N. Recommendations of the Advisory Committee on Immunization Practices for Use of a Hepatitis B Vaccine with a Novel Adjuvant. Mmwr. Morb. Mortal. Wkly Rep. 2018, 67, 455–458. [Google Scholar] [CrossRef]
- Bode, C.; Zhao, G.; Steinhagen, F.; Kinjo, T.; Klinman, D.M. CpG DNA as a vaccine adjuvant. Expert. Rev. Vaccines 2011, 10, 499–511. [Google Scholar] [CrossRef] [Green Version]
- Minutello, M.; Senatore, F.; Cecchinelli, G.; Bianchi, M.; Andreani, T.; Podda, A.; Crovari, P. Safety and immunogenicity of an inactivated subunit influenza virus vaccine combined with MF59 adjuvant emulsion in elderly subjects, immunized for three consecutive influenza seasons. Vaccine 1999, 17, 99–104. [Google Scholar] [CrossRef]
- Ansaldi, F.; Bacilieri, S.; Durando, P.; Sticchi, L.; Valle, L.; Montomoli, E.; Icardi, G.; Gasparini, R.; Crovari, P. Cross-protection by MF59-adjuvanted influenza vaccine: Neutralizing and haemagglutination-inhibiting antibody activity against A(H3N2) drifted influenza viruses. Vaccine 2008, 26, 1525–1529. [Google Scholar] [CrossRef]
- Nolan, T.; Bravo, L.; Ceballos, A.; Mitha, E.; Gray, G.; Quiambao, B.; Patel, S.S.; Bizjajeva, S.; Bock, H.; Nazaire-Bermal, N.; et al. Enhanced and persistent antibody response against homologous and heterologous strains elicited by a MF59-adjuvanted influenza vaccine in infants and young children. Vaccine 2014, 32, 6146–6156. [Google Scholar] [CrossRef] [PubMed]
- Banzhoff, A.; Gasparini, R.; Laghi-Pasini, F.; Staniscia, T.; Durando, P.; Montomoli, E.; Capecchi, P.; Di Giovanni, P.; Sticchi, L.; Gentile, C.; et al. MF59-adjuvanted H5N1 vaccine induces immunologic memory and heterotypic antibody responses in non-elderly and elderly adults. PLoS ONE 2009, 4, e4384. [Google Scholar] [CrossRef]
- Vesikari, T.; Forstén, A.; Borkowski, A.; Gaitatzis, N.; Banzhoff, A.; Clemens, R. Homologous and heterologous antibody responses to a one-year booster dose of an MF59((R)) adjuvanted A/H5N1 pre-pandemic influenza vaccine in pediatric subjects. Hum. Vaccines Immunother. 2012, 8, 921–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galli, G.; Hancock, K.; Hoschler, K.; Devos, J.; Praus, M.; Bardelli, M.; Malzone, C.; Castellino, F.; Gentile, C.; McNally, T.; et al. Fast rise of broadly cross-reactive antibodies after boosting long-lived human memory B cells primed by an MF59 adjuvanted prepandemic vaccine. Proc. Natl. Acad. Sci. USA 2009, 106, 7962–7967. [Google Scholar] [CrossRef] [Green Version]
- De Jonge, J.; Van Dijken, H.; De Heij, F.; Spijkers, S.; Mouthaan, J.; De Jong, R.; Roholl, P.; Adami, E.A.; Akamatsu, M.A.; Ho, P.L.; et al. H7N9 influenza split vaccine with SWE oil-in-water adjuvant greatly enhances cross-reactive humoral immunity and protection against severe pneumonia in ferrets. Npj Vaccines 2020, 5, 38. [Google Scholar] [CrossRef]
- Hatta, M.; Zhong, G.; Chiba, S.; Lopes, T.J.; Neumann, G.; Kawaoka, Y. Effectiveness of Whole, Inactivated, Low Pathogenicity Influenza A(H7N9) Vaccine against Antigenically Distinct, Highly Pathogenic H7N9 Virus. Emerg. Infect Dis. 2018, 24, 1910–1913. [Google Scholar] [CrossRef]
- Khurana, S.; Chearwae, W.; Castellino, F.; Manischewitz, J.; King, L.R.; Honorkiewicz, A.; Rock, M.T.; Edwards, K.M.; Del Giudice, G.; Rappuoli, R.; et al. Vaccines with MF59 adjuvant expand the antibody repertoire to target protective sites of pandemic avian H5N1 influenza virus. Sci. Transl. Med. 2010, 2, 15ra5. [Google Scholar] [CrossRef]
- Khurana, S.; Verma, N.; Yewdell, J.W.; Hilbert, A.K.; Castellino, F.; Lattanzi, M.; Del Giudice, G.; Rappuoli, R.; Golding, H. MF59 adjuvant enhances diversity and affinity of antibody-mediated immune response to pandemic influenza vaccines. Sci. Transl. Med. 2011, 3, 85ra48. [Google Scholar] [CrossRef] [Green Version]
- Chu, D.W.S.; Hwang, S.-J.; Lim, F.S.; Oh, H.M.L.; Thongcharoen, P.; Yang, P.-C.; Bock, H.L.; Dramé, M.; Gillard, P.; Hutagalung, Y.; et al. Immunogenicity and tolerability of an AS03(A)-adjuvanted prepandemic influenza vaccine: A phase III study in a large population of Asian adults. Vaccine 2009, 27, 7428–7435. [Google Scholar] [CrossRef]
- Langley, J.M.; Frenette, L.; Ferguson, L.; Riff, D.; Sheldon, E.; Risi, G.; Johnson, C.; Li, P.; Kenney, R.; Innis, B.L.; et al. Safety and cross-reactive immunogenicity of candidate AS03-adjuvanted prepandemic H5N1 influenza vaccines: A randomized controlled phase 1/2 trial in adults. J. Infect. Dis. 2010, 201, 1644–1653. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, T.F.; Horacek, T.; Knuf, M.; Damman, H.-G.; Roman, F.; Dramé, M.; Gillard, P.; Jilg, W. Single dose vaccination with AS03-adjuvanted H5N1 vaccines in a randomized trial induces strong and broad immune responsiveness to booster vaccination in adults. Vaccine 2009, 27, 6284–6290. [Google Scholar] [CrossRef] [PubMed]
- Leroux-Roels, I.; Roman, F.; Forgus, S.; Maes, C.; De Boever, F.; Dramé, M.; Gillard, P.; Van Der Most, R.; Van Mechelen, M.; Hanon, E.; et al. Priming with AS03 A-adjuvanted H5N1 influenza vaccine improves the kinetics, magnitude and durability of the immune response after a heterologous booster vaccination: An open non-randomised extension of a double-blind randomised primary study. Vaccine 2010, 28, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Moris, P.; Van Der Most, R.; Leroux-Roels, I.; Clement, F.; Dramé, M.; Hanon, E.; Leroux-Roels, G.G.; Van Mechelen, M. H5N1 influenza vaccine formulated with AS03 A induces strong cross-reactive and polyfunctional CD4 T-cell responses. J. Clin. Immunol. 2011, 31, 443–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khurana, S.; and the CHI Consortium; Coyle, E.M.; Manischewitz, J.; King, L.R.; Gao, J.; Germain, R.N.; Schwartzberg, P.L.; Tsang, J.S.; Golding, H. AS03-adjuvanted H5N1 vaccine promotes antibody diversity and affinity maturation, NAI titers, cross-clade H5N1 neutralization, but not H1N1 cross-subtype neutralization. NPJ Vaccines 2018, 3, 40. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Belser, J.A.; Pulit-Penaloza, J.A.; Creager, H.M.; Guo, Z.; Jefferson, S.N.; Liu, F.; York, I.A.; Stevens, J.; Maines, T.R.; et al. Stockpiled pre-pandemic H5N1 influenza virus vaccines with AS03 adjuvant provide cross-protection from H5N2 clade 2.3.4.4 virus challenge in ferrets. Virology 2017, 508, 164–169. [Google Scholar] [CrossRef]
- Miller, E.; Andrews, N.; Stellitano, L.; Stowe, J.; Winstone, A.; Shneerson, J.; Verity, C. Risk of narcolepsy in children and young people receiving AS03 adjuvanted pandemic A/H1N1 2009 influenza vaccine: Retrospective analysis. BMJ 2013, 346, f794. [Google Scholar] [CrossRef] [Green Version]
- Nohynek, H.; Jokinen, J.J.; Partinen, M.; Vaarala, O.; Kirjavainen, T.; Sundman, J.; Himanen, S.-L.; Hublin, C.; Julkunen, I.; Olsén, P.; et al. AS03 adjuvanted AH1N1 vaccine associated with an abrupt increase in the incidence of childhood narcolepsy in Finland. PLoS ONE 2012, 7, e33536. [Google Scholar] [CrossRef]
- Han, F.; Lin, L.; Warby, S.C.; Faraco, J.; Li, J.; Dong, S.X.; An, P.; Zhao, L.; Wang, L.H.; Li, Q.Y.; et al. Narcolepsy onset is seasonal and increased following the 2009 H1N1 pandemic in China. Ann. Neurol. 2011, 70, 410–417. [Google Scholar] [CrossRef]
- De La Herrán-Arita, A.K.; Kornum, B.R.; Mahlios, J.; Jiang, W.; Lin, L.; Hou, T.; Macaubas, C.; Einen, M.; Plazzi, G.; Crowe, C.; et al. CD4+ T cell autoimmunity to hypocretin/orexin and cross-reactivity to a 2009 H1N1 influenza A epitope in narcolepsy. Sci. Transl. Med. 2013, 5, 216ra176. [Google Scholar] [CrossRef]
- Tsai, T.F.; Crucitti, A.; Nacci, P.; Nicolay, U.; Della Cioppa, G.; Ferguson, J.; Clemens, R. Explorations of clinical trials and pharmacovigilance databases of MF59(R)-adjuvanted influenza vaccines for associated cases of narcolepsy. Scand J. Infect Dis. 2011, 43, 702–706. [Google Scholar] [CrossRef]
- Kim, W.J.; Lee, S.D.; Lee, E.; Namkoong, K.; Choe, K.-W.; Song, J.Y.; Cheong, H.J.; Jeong, H.W.; Heo, J.Y. Incidence of narcolepsy before and after MF59-adjuvanted influenza A(H1N1)pdm09 vaccination in South Korean soldiers. Vaccine 2015, 33, 4868–4872. [Google Scholar] [CrossRef] [PubMed]
- Crotty, S. A brief history of T cell help to B cells. Nat. Rev. Immunol. 2015, 15, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Pillet, S.; Aubin, Éric; Trépanier, S.; Poulin, J.-F.; Yassine-Diab, B.; Ter Meulen, J.; Ward, B.J.; Landry, N. Humoral and cell-mediated immune responses to H5N1 plant-made virus-like particle vaccine are differentially impacted by alum and GLA-SE adjuvants in a Phase 2 clinical trial. Npj Vaccines 2018, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, D.; Van Hoeven, N.; Baldwin, S.; Levin, Y.; Kochba, E.; Magill, A.; Charland, N.; Landry, N.; Nu, K.; Frevol, A.; et al. The adjuvant GLA-AF enhances human intradermal vaccine responses. Sci. Adv. 2018, 4, eaas9930. [Google Scholar] [CrossRef] [Green Version]
- Clegg, C.H.; Roque, R.; Perrone, L.A.; Rininger, J.A.; Bowen, R.; Reed, S.G. GLA-AF, an emulsion-free vaccine adjuvant for pandemic influenza. PLoS ONE 2014, 9, e88979. [Google Scholar] [CrossRef] [Green Version]
- Ko, E.-J.; Lee, Y.; Lee, Y.-T.; Kim, Y.-J.; Kim, K.-H.; Kang, S.-M. MPL and CpG combination adjuvants promote homologous and heterosubtypic cross protection of inactivated split influenza virus vaccine. Antivir. Res. 2018, 156, 107–115. [Google Scholar] [CrossRef]
- Goff, P.H.; Hayashi, T.; Martínez-Gil, L.; Corr, M.; Crain, B.; Yao, S.; Cottam, H.B.; Chan, M.; Ramos, I.; Eggink, D.; et al. Synthetic Toll-like receptor 4 (TLR4) and TLR7 ligands as influenza virus vaccine adjuvants induce rapid, sustained, and broadly protective responses. J. Virol. 2015, 89, 3221–3235. [Google Scholar] [CrossRef] [Green Version]
- Hung, I.F.-N.; Zhang, A.J.; To, K.K.-W.; Chan, J.F.-W.; Li, P.; Wong, T.-L.; Zhang, R.; Chan, T.-C.; Chan, B.C.-Y.; Wai, H.H.; et al. Topical imiquimod before intradermal trivalent influenza vaccine for protection against heterologous non-vaccine and antigenically drifted viruses: A single-centre, double-blind, randomised, controlled phase 2b/3 trial. Lancet Infect Dis. 2016, 16, 209–218. [Google Scholar] [CrossRef]
- Van Hoeven, N.; Fox, C.B.; Granger, B.; Evers, T.; Joshi, S.W.; Nana, G.I.; Evans, S.C.; Lin, S.; Liang, H.; Liang, L.; et al. A Formulated TLR7/8 Agonist is a Flexible, Highly Potent and Effective Adjuvant for Pandemic Influenza Vaccines. Sci. Rep. 2017, 7, 46426. [Google Scholar] [CrossRef]
- Wang, B.-Z.; Quan, F.-S.; Kang, S.-M.; Bozja, J.; Skountzou, I.; Compans, R.W. Incorporation of membrane-anchored flagellin into influenza virus-like particles enhances the breadth of immune responses. J. Virol. 2008, 82, 11813–11823. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.-Z.; Xu, R.; Quan, F.-S.; Kang, S.-M.; Wang, L.; Compans, R.W. Intranasal immunization with influenza VLPs incorporating membrane-anchored flagellin induces strong heterosubtypic protection. PLoS ONE 2010, 5, e13972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambhara, S.; Woods, S.; Arpino, R.; Kurichh, A.; Tamane, A.; Underdown, B.; Klein, M.; Bengtsson, K.L.; Morein, B.; Burt, D. Heterotypic protection against influenza by immunostimulating complexes is associated with the induction of cross-reactive cytotoxic T lymphocytes. J. Infect. Dis. 1998, 177, 1266–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, F.; Saeland, E.; Baart, M.; Koldijk, M.; Tolboom, J.T.; Dekking, L.; Koudstaal, W.; Lovgren-Bengtsson, K.; Goudsmit, J.; Radošević, K. Matrix-M adjuvation broadens protection induced by seasonal trivalent virosomal influenza vaccine. Virol. J. 2015, 12, 210. [Google Scholar] [CrossRef]
- Smith, G.; Liu, Y.V.; Flyer, D.C.; Massare, M.J.; Zhou, B.; Patel, N.; Ellingsworth, L.R.; Lewis, M.; Cummings, J.F.; Glenn, G. Novel hemagglutinin nanoparticle influenza vaccine with Matrix-M adjuvant induces hemagglutination inhibition, neutralizing, and protective responses in ferrets against homologous and drifted A(H3N2) subtypes. Vaccine 2017, 35, 5366–5372. [Google Scholar] [CrossRef] [PubMed]
- Cox, F.; Roos, A.; Hafkemeijer, N.; Baart, M.; Tolboom, J.; Dekking, L.; Stittelaar, K.; Goudsmit, J.; Radošević, K.; Saeland, E. Matrix-M Adjuvated Seasonal Virosomal Influenza Vaccine Induces Partial Protection in Mice and Ferrets against Avian H5 and H7 Challenge. PLoS ONE 2015, 10, e0135723. [Google Scholar] [CrossRef] [Green Version]
- Cox, R.J.; Major, D.; Pedersen, G.K.; Pathirana, R.D.; Hoschler, K.; Guilfoyle, K.; Roseby, S.; Bredholt, G.; Assmus, J.; Breakwell, L.; et al. Matrix M H5N1 Vaccine Induces Cross-H5 Clade Humoral Immune Responses in a Randomized Clinical Trial and Provides Protection from Highly Pathogenic Influenza Challenge in Ferrets. PLoS ONE 2015, 10, e0131652. [Google Scholar] [CrossRef] [Green Version]
- Quan, F.S.; Compans, R.W.; Nguyen, H.H.; Kang, S.M. Induction of heterosubtypic immunity to influenza virus by intranasal immunization. J. Virol. 2008, 82, 1350–1359. [Google Scholar] [CrossRef] [Green Version]
- Tamura, S.; Ito, Y.; Asanuma, H.; Hirabayashi, Y.; Suzuki, Y.; Nagamine, T.; Aizawa, C.; Kurata, T. Cross-protection against influenza virus infection afforded by trivalent inactivated vaccines inoculated intranasally with cholera toxin B subunit. J. Immunol. 1992, 149, 981–988. [Google Scholar]
- Tumpey, T.M.; Renshaw, M.; Clements, J.D.; Katz, J.M. Mucosal delivery of inactivated influenza vaccine induces B-cell-dependent heterosubtypic cross-protection against lethal influenza A H5N1 virus infection. J. Virol. 2001, 75, 5141–5150. [Google Scholar] [CrossRef] [Green Version]
- Rosenkrands, I.; Vingsbo-Lundberg, C.; Bundgaard, T.J.; Lindenstrøm, T.; Enouf, V.; Van Der Werf, S.; Andersen, P.; Agger, E.M. Enhanced humoral and cell-mediated immune responses after immunization with trivalent influenza vaccine adjuvanted with cationic liposomes. Vaccine 2011, 29, 6283–6291. [Google Scholar] [CrossRef]
- Christensen, D.; Christensen, J.P.; Korsholm, K.S.; Isling, L.K.; Erneholm, K.; Thomsen, A.R.; Andersen, P. Seasonal Influenza Split Vaccines Confer Partial Cross-Protection against Heterologous Influenza Virus in Ferrets When Combined with the CAF01 Adjuvant. Front. Immunol. 2017, 8, 1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Li, B.; Wu, M.X. Effective and lesion-free cutaneous influenza vaccination. Proc. Natl. Acad. Sci. USA 2015, 112, 5005–5010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mata-Haro, V.; Cekic, C.; Martin, M.; Chilton, P.M.; Casella, C.R.; Mitchell, T.C. The vaccine adjuvant monophosphoryl lipid A as a TRIF-biased agonist of TLR4. Science 2007, 316, 1628–1632. [Google Scholar] [CrossRef] [PubMed]
- Pantel, A.; Cheong, C.; Dandamudi, D.; Shrestha, E.; Mehandru, S.; Brane, L.; Ruane, D.; Teixeira, A.; Bozzacco, L.; Steinman, R.M.; et al. A new synthetic TLR4 agonist, GLA, allows dendritic cells targeted with antigen to elicit Th1 T-cell immunity in vivo. Eur. J. Immunol. 2012, 42, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Coler, R.N.; Bertholet, S.; Moutaftsi, M.; Guderian, J.A.; Windish, H.P.; Baldwin, S.L.; Laughlin, E.M.; Duthie, M.S.; Fox, C.B.; Carter, D.; et al. Development and characterization of synthetic glucopyranosyl lipid adjuvant system as a vaccine adjuvant. PLoS ONE 2011, 6, e16333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behzad, H.; Huckriede, A.L.W.; Haynes, L.; Gentleman, B.; Coyle, K.; Wilschut, J.C.; Kollmann, T.R.; Reed, S.G.; McElhaney, J.E. GLA-SE, a synthetic toll-like receptor 4 agonist, enhances T-cell responses to influenza vaccine in older adults. J. Infect. Dis. 2012, 205, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Wagstaff, A.J.; Perry, C.M. Topical imiquimod: A review of its use in the management of anogenital warts, actinic keratoses, basal cell carcinoma and other skin lesions. Drugs 2007, 67, 2187–2210. [Google Scholar] [CrossRef]
- Smith, K.D.; Andersen-Nissen, E.; Hayashi, F.; Strobe, K.; A Bergman, M.; Barrett, S.L.R.; Cookson, B.T.; Aderem, A. Toll-like receptor 5 recognizes a conserved site on flagellin required for protofilament formation and bacterial motility. Nat. Immunol. 2003, 4, 1247–1253. [Google Scholar] [CrossRef]
- Mizel, S.B.; Bates, J.T. Flagellin as an adjuvant: Cellular mechanisms and potential. J. Immunol. 2010, 185, 5677–5682. [Google Scholar] [CrossRef] [Green Version]
- Hajam, I.A.; Dar, P.A.; Shahnawaz, I.; Jaume, J.C.; Lee, J.H. Bacterial flagellin-a potent immunomodulatory agent. Exp. Mol. Med. 2017, 49, e373. [Google Scholar] [CrossRef]
- Song, W.S.; Jeon, Y.J.; Namgung, B.; Hong, M.; Yoon, S.I. A conserved TLR5 binding and activation hot spot on flagellin. Sci. Rep. 2017, 7, 40878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, F.; Smith, K.D.; Ozinsky, A.; Hawn, T.R.; Yi, E.C.; Goodlett, D.R.; Eng, J.K.; Akira, S.; Underhill, D.M.; Aderem, A. The innate immune response to bacterial flagellin is mediated by Toll-like receptor 5. Nature 2001, 410, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Halff, E.F.; Diebolder, C.A.; Versteeg, M.; Schouten, A.; Brondijk, T.H.C.; Huizinga, E.G. Formation and structure of a NAIP5-NLRC4 inflammasome induced by direct interactions with conserved N- and C-terminal regions of flagellin. J. Biol. Chem. 2012, 287, 38460–38472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, D.; Tuo, W. QS-21: A Potent Vaccine Adjuvant. Nat. Prod. Chem. Res. 2016, 3. [Google Scholar] [CrossRef] [Green Version]
- Kensil, C.R.; Patel, U.; Lennick, M.; Marciani, D. Separation and characterization of saponins with adjuvant activity from Quillaja saponaria Molina cortex. J. Immunol. 1991, 146, 431–437. [Google Scholar] [PubMed]
- Kensil, C.R.; Kammer, R. QS-21: A water-soluble triterpene glycoside adjuvant. Expert Opin. Investig. Drugs 1998, 7, 1475–1482. [Google Scholar] [CrossRef]
- Lovgren Bengtsson, K.; Morein, B.; Osterhaus, A.D. ISCOM technology-based Matrix M adjuvant: Success in future vaccines relies on formulation. Expert Rev. Vaccines 2011, 10, 401–403. [Google Scholar] [CrossRef]
- Cox, J.C.; Sjolander, A.; Barr, I.G. ISCOMs and other saponin based adjuvants. Adv. Drug Deliv. Rev. 1998, 32, 247–271. [Google Scholar] [CrossRef]
- Sun, H.X.; Xie, Y.; Ye, Y.P. ISCOMs and ISCOMATRIX. Vaccine 2009, 27, 4388–4401. [Google Scholar] [CrossRef]
- Temizoz, B.; Kuroda, E.; Ishii, K.J. Vaccine adjuvants as potential cancer immunotherapeutics. Int. Immunol. 2016, 28, 329–338. [Google Scholar] [CrossRef]
- Pizza, M.; Giuliani, M.; Fontana, M.; Monaci, E.; Douce, G.; Dougan, G.; Mills, K.; Rappuoli, R.; Del Giudice, G. Mucosal vaccines: Non toxic derivatives of LT and CT as mucosal adjuvants. Vaccine 2001, 19, 2534–2541. [Google Scholar] [CrossRef]
- Beddoe, T.; Paton, A.W.; Le Nours, J.; Rossjohn, J.; Paton, J.C. Structure, biological functions and applications of the AB5 toxins. Trends Biochem. Sci. 2010, 35, 411–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valli, E.; Harriett, A.J.; Nowakowska, M.K.; Baudier, R.L.; Provosty, W.B.; McSween, Z.; Lawson, L.B.; Nakanishi, Y.; Norton, E.B. LTA1 is a safe, intranasal enterotoxin-based adjuvant that improves vaccine protection against influenza in young, old and B-cell-depleted (muMT) mice. Sci. Rep. 2019, 9, 15128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clements, J.D.; Norton, E.B. The Mucosal Vaccine Adjuvant LT(R192G/L211A) or dmLT. mSphere 2018, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Hora, V.P.; Conceicao, F.R.; Dellagostin, O.A.; Doolan, D.L. Non-toxic derivatives of LT as potent adjuvants. Vaccine 2011, 29, 1538–1544. [Google Scholar] [CrossRef]
- Agger, E.M.; Rosenkrands, I.; Hansen, J.; Brahimi, K.; Vandahl, B.S.; Aagaard, C.; Werninghaus, K.; Kirschning, C.; Lang, R.; Christensen, D.; et al. Cationic liposomes formulated with synthetic mycobacterial cordfactor (CAF01): A versatile adjuvant for vaccines with different immunological requirements. PLoS ONE 2008, 3, e3116. [Google Scholar] [CrossRef] [Green Version]
- Davidsen, J.; Rosenkrands, I.; Christensen, D.; Vangala, A.; Kirby, D.; Perrie, Y.; Agger, E.M.; Andersen, P. Characterization of cationic liposomes based on dimethyldioctadecylammonium and synthetic cord factor from M. tuberculosis (trehalose 6,6’-dibehenate)-a novel adjuvant inducing both strong CMI and antibody responses. Biochim. Biophys. Acta 2005, 1718, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Lopes, P.P.; Todorov, G.; Pham, T.T.; Nesburn, A.B.; Bahraoui, E.; Benmohamed, L. Laser Adjuvant-Assisted Peptide Vaccine Promotes Skin Mobilization of Dendritic Cells and Enhances Protective CD8(+) TEM and TRM Cell Responses against Herpesvirus Infection and Disease. J. Virol. 2018, 92. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Pravetoni, M.; Bhayana, B.; Pentel, P.R.; Wu, M.X. High immunogenicity of nicotine vaccines obtained by intradermal delivery with safe adjuvants. Vaccine 2012, 31, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Zeng, Q.; Wu, M.X. Improved efficacy of dendritic cell-based immunotherapy by cutaneous laser illumination. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2012, 18, 2240–2249. [Google Scholar] [CrossRef] [Green Version]
- Morse, K.; Kimizuka, Y.; Chan, M.P.K.; Shibata, M.; Shimaoka, Y.; Takeuchi, S.; Forbes, B.; Nirschl, C.J.; Li, B.; Zeng, Y.; et al. Near-Infrared 1064 nm Laser Modulates Migratory Dendritic Cells To Augment the Immune Response to Intradermal Influenza Vaccine. J. Immunol. 2017, 199, 1319–1332. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Kim, P.; Farinelli, B.; Doukas, A.; Yun, S.-H.; Gelfand, J.A.; Anderson, R.R.; Wu, M.X. A novel laser vaccine adjuvant increases the motility of antigen presenting cells. PLoS ONE 2010, 5, e13776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashiwagi, S.; Yuan, J.; Forbes, B.; Hibert, M.L.; Lee, E.L.Q.; Whicher, L.; Goudie, C.; Yang, Y.; Chen, T.; Edelblute, B.; et al. Near-infrared laser adjuvant for influenza vaccine. PLoS ONE 2013, 8, e82899. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.A.; Nazarian, R.M.; Kashiwagi, S.; Brauns, T.; Martin, B.; Kimizuka, Y.; Korek, S.; Botvinick, E.; Elkins, K.; Thomas, L.; et al. A pilot clinical trial of a near-infrared laser vaccine adjuvant: Safety, tolerability, and cutaneous immune cell trafficking. FASEB J. 2019, 33, 3074–3081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Shah, D.; Chen, X.; Anderson, R.R.; Wu, M.X. A micro-sterile inflammation array as an adjuvant for influenza vaccines. Nat. Commun. 2014, 5, 4447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Y.; Zhu, X.; Hossen, N.; Kakar, P.; Zhao, Y.; Chen, X. Augmentation of vaccine-induced humoral and cellular immunity by a physical radiofrequency adjuvant. Nat. Commun. 2018, 9, 3695. [Google Scholar] [CrossRef]

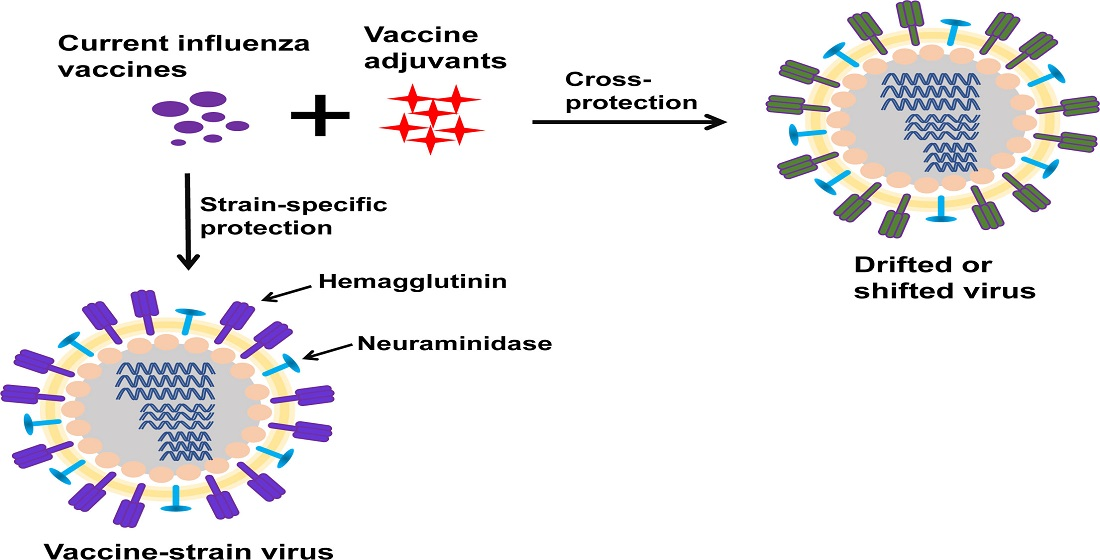{kind=link}
Table 1.
Influenza vaccine types.
| Categories | Vaccine Types | ||
|---|---|---|---|
| Number of viral strains | Trivalent (two type A, one type B) | Quadrivalent (two type A, two type B) | |
| Live-attenuated or inactivated | Inactivated (subunit, split-virion, virosome) | Live-attenuated | |
| Production method | Egg-based | Cell-based | Recombinant protein-based |
| Delivery routes (devices) | IM (traditional needles, needle-free Jet Injectors) | IN (Intranasal Sprayer) | ID (Intradermal Microinjection Systems, MicronJet600) |
| Usage | Seasonal | Pre-pandemic | Pandemic |
Table 2.
List of licensed vaccine adjuvants.
| Adjuvants | Formulation and Type | Year of Approval | Vaccines |
|---|---|---|---|
| Alum | Aluminum salts | 1930s | A number of vaccines (e.g., tetanus and diphtheria vaccines) |
| MF59 | Squalene emulsion (Novartis) | 1997 | Seasonal influenza vaccine |
| AS04 | MPL adsorbed on Alum adjuvant | 2009 | HPV vaccine |
| AS03 | Squalene emulsion (GlaxoSmithKline) | 2013 | Pre-pandemic H5N1 vaccine |
| AS01 | MPL/QS21 in liposome | 2015 | RTS,S malaria vaccine |
| CpG 1018 | 22-mer oligonucleotide | 2017 | Hepatitis B VLP vaccine |
Table 3.
Licensed adjuvants assist influenza vaccines to induce cross-protective immunity in human subjects.
Table 3.
Licensed adjuvants assist influenza vaccines to induce cross-protective immunity in human subjects.
| Adjuvant | Vaccine and Immunization Regimen | Age Group | Cross-Protective Immunity | Safety | Reference |
|---|---|---|---|---|---|
| MF59 | Trivalent influenza vaccine (TIV), subunit, single dose | Elderly | Heterologous HI GMT against seasonal influenza strains | More local and systemic adverse reactions. No serious adverse events related to vaccination | [110] |
| MF59 | TIV, subunit, single dose | Elderly | Heterologous HI GMT against H3N2 | Not studied | [111] |
| MF59 | TIV, subunit, two doses (28 days apart) | Infants and young children | Heterologous HI GMT and seroconversion rates against all strains after the first and second dose | Higher rates of solicited adverse reactions. No serious adverse events related to vaccination | [112] |
| MF59 | H5N1 vaccine (A/Vietnam/1194/2004, clade 1); subunit, two-dose prime (21 days apart) and one-dose boost (6 months later) | Non-elderly adults and elderly | HI GMT against clade 2 strain A/turkey/Turkey/1/05 detectable after two-dose priming and increased after boost | Common solicited adverse reactions, such as myalgia and headache. No serious adverse events related to vaccination | [113] |
| MF59 | H5N1 vaccine (A/Vietnam/1194/2004, clade 1); two-dose prime (21 days apart) and one-dose boost (12 months later) | Pediatrics | HI GMT against clade 2 strains A/Indonesia/5/2005 and A/Anhui/1/2005 after prime and significantly enhanced after boost | Common mild–moderate local and systemic adverse reactions. No serious adverse events related to vaccination | [114] |
| MF59 | H5N3 vaccine prime (A/duck/Singapore/97, clade 0); H5N1 vaccine boost (A/Vietnam/1194/ 2004, clade 1); two-dose prime (21 days apart) or three-dose prime with the third dose given 16 months later, two-dose boost 6 years later (21 days apart) | Non-elderly adults | Heterologous immunity against clade 0 strain A/Hong Kong/156/97, clade 1 strain A/Cambodia/R04050550/2007, and clade 2 strains A/Indonesia/5/2005, A/Turkey/15/2006, and A/Anhui/1/2005 | Common mild–moderate local and systemic adverse reactions. No serious adverse events related to vaccination | [115] |
| AS03 | Split-virion H5N1 vaccine (A/Vietnam/1194/2004, clade 1); two doses (21 days apart) | Non-elderly adults | HI GMT against clade 2 strain A/Indonesia/05/2005 after second dose | Higher rates of mild–moderate adverse reactions. No serious adverse events related to vaccination | [120] |
| AS03 | Split-virion H5N1 vaccine (A/Indonesia/5/2005, clade 2); two doses (21 days apart) | Non-elderly adults | HI GMT against clade 1 strain A/Vietnam/1194/04 after second dose | More common adverse events. No serious adverse events related to vaccination | [121] |
| AS03 | Split-virion H5N1 vaccine prime (A/Vietnam/1194/2004, clade 1); same strain or clade 2 strain boost (A/Indonesia/05/2005); One or two-dose prime (21 days apart) and one-dose boost 6 or 12 months later | Non-elderly adults | Seroconversion against clade 2 strain A/Indonesia/05/2005 after two-dose prime | No vaccine-related serious adverse events | [122] |
| AS03 | Split-virion H5N1 vaccine prime (A/Vietnam/1194/2004, clade 1) and clade 2 strain boost (A/Indonesia/5/2005); two-dose prime (21 days apart); one or two-dose boost 14 months later (21 days apart) | Non-elderly adults | Rapid induction of HI GMT against clade 2 strain in adjuvanted vaccine-primed subjects | No vaccine-related serious adverse events | [123] |
| AS03 | Split-virion H5N1 vaccine (A/Vietnam/1194/2004, clade 1); two doses (21 days apart) | Non-elderly adults | Cross-reactive CD4+ T cells against clade 2 strains A/Indonesia/5/2005 and A/Anhui/1/2005 | Not studied | [124] |
Table 4.
Experimental adjuvants assist influenza vaccines to induce cross-protective immunity.
| Adjuvant | Vaccine and Immunization Regimen | Study Subjects | Cross-Protective Immunity | Safety | Reference |
|---|---|---|---|---|---|
| SWE | Split virion vaccine of A/Shanghai/2/2013 (H7N9)-A/Puerto Rico/8/34 (PR8)-IDCDC-RG32A.3; two doses (21 days apart); IM | Ferrets | HI titer against heterologous Eurasian and North American Lineages of H7N2, H7N3, H7N7, and H7N9 viruses, Heterologous protection against A/Anhui/1/2013 (H7N9) virus | Not studied | [116] |
| AddaVax | Inactivated whole virus vaccine of reassortant A/Hong Kong/125/2017 (H7N9) and PR8 backbone; two doses (28 days apart); IM | Ferrets | HI titer and protection against highly pathogenic heterologous H7N9 rGD/3-NA294R virus | Not studied | [117] |
| GLA-SE | Plant-produced H5-VLP (A/Indonesia/05/2005, clade 2); two doses (21 days apart); IM | Non-elderly adults | Polyfunctional and sustained heterologous CD4+ T cell responses against influenza H2 protein | Higher incidences of solicited symptoms and mostly mild or moderate | [134] |
| GLA-AF | Plant-produced H5-VLP (A/Indonesia/05/2005, clade 2); two doses (21 days apart); ID | Non-elderly adults | HI GMI and seroconversion against heterologous clade 2 virus A/Anhui/1/2005 and HI GMI and seroconversion against clade 1 virus A/Vietnam/1203/2004 | Transient erythema; no serious adverse events related to vaccination | [135] |
| GLA-AF | Plant-produced H5-VLP (A/Indonesia/5/05, clade 2); two doses (21 days apart) in mice and guinea pigs; one dose in ferrets; IM or ID | Mice, guinea pig, and ferrets | HI titer and protection against heterologous virus A/Duck/Hunan/795/2002 in mice and protection against clade 1 strain A/Vietnam/1203/04 in ferrets | Guinea pigs: no temperature spikes or body weight decrease; Ferrets: no local reactions or body temperature increase | [135] |
| GLA-AF | Recombinant HA (rHA) of H5N1 A/Vietnam/1203/04 or A/Indonesia /05/05 viruses; one dose in mice and one or two doses (21 days apart) in ferrets; IM | Mice and ferrets | Cross-clade HI titer and protection | Not studies | [136] |
| MPL and CPG combination | Split virion vaccine of A/California/04/2009 H1N1; one or two doses (21 days apart); IM | Mice | HI titer and protection against heterosubtypic reassortant H5N1 A/Vietnam/1203/2004 virus | Not studied | [137] |
| TLR4 and TLR7 agonist combination | rHA of PR8 H1N1; chimeric rHA (same stalk region); one dose (rHA) or 3 doses (chimeric rHA); IM | Mice | Heterologous protection against A/California/04/2009 H1N1 virus; Heterologous protection against B/Florida/04/2006 (Yamagata lineage); Heterosubtypic protection against reassortant A/Vietnam/1203/2004 H5N1 virus | Not studied | [138] |
| Imiquimod (Aldara) | TIV (Intanza); one dose; ID | Healthy student volunteers | Heterologous HI and MN titer against non-vaccine strains | More common redness and swelling; no serious adverse events related to vaccination | [139] |
| 3M-052 | rHA of A/Vietnam/1203/04 H5N1; two doses with 28 days apart in mice; one dose in ferrets; IM | Mice and ferrets | Cross-clade antibody binding in mice and heterologous protection against A/Whooper Swan/Mongolia/ 244/05 H5N1 virus in ferrets | Not studied | [140] |
| Membrane-anchored flagellin | HA/M1VLPs based on PR8 virus; two doses (28 days apart); IM or IN | Mice | Heterosubtypic protection against A/Philippines/82 (H3N2) virus | Not studied | [141,142] |
| ISCOMs | Fluzone® monovalent subunit vaccine of A/Taiwan/1/86 H1N1; two doses (21 days apart); subcutaneous | Mice | Heterosubtypic protection against A/Japan/305/57 (H2N2) virus due to CTL but not antibody responses | Not studied | [143] |
| Matrix-M | Trivalent virosomal vaccine; one to three doses (21 days apart); IM | Mice | Heterologous protection against influenza A and B strains | Not studied | [144] |
| Matrix-M | TIV; two doses (21 days apart); IM | Mice and ferrets | Heterologous protection against H3N2 strain A/Texas/71/2007; Heterosubtypic protection against H5N1 and H7N7 viruses | Not studied | [145,146] |
| Matrix-M | Inactivated virosomal H5N1 vaccine of A/Vietnam/1194/2004 (clade 1); two doses (21 days apart); IM | Non-elderly adults | HI titer against heterologous clade 1 virus (A/Cambodia/R0405050/2007) and cross-clade HI titer against clade 2 viruses (A/Indonesia/5/2005 and A/turkey/Turkey/1/2005) | Not studied | [147] |
| Cholera toxin | Inactivated PR8 vaccine; two doses (14 days apart); IN | Mice | Heterologous protection against H1N1 and heterosubtypic protection against H3N2 virus (A/Philippines/82) | Not studied | [148] |
| Cholera toxin B subunit | HA of A/Fukuoka /C29/85 (H3N2) or A/Sichuan/2/87 (H3N2); one dose; IN | Mice | Heterologous protection against H3N2 virus (A/Guizhou/54/89-X) | Not studied | [149] |
| LT (R192G) | Whole-inactivated X-31 (H3N2) vaccine; three doses (7 days apart); IN | Mice | Heterosubtypic protection against H5N1 virus | Not studied | [150] |
| CAF01 | TIV; two doses (3-4 weeks apart); subcutaneous | Mice and ferrets | Heterologous protection against H1N1 viruses | Not studied | [151,152] |
| NAFL | Inactivated PR8 vaccine; one dose; transdermal | Mice and miniature pigs | Heterologous and heterosubtypic protection against H1N1 and H3N2 viruses in mice | Minimal local reactions in miniature pigs | [153] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Li, Z.; Zhao, Y.; Li, Y.; Chen, X. Adjuvantation of Influenza Vaccines to Induce Cross-Protective Immunity. Vaccines 2021, 9, 75. https://doi.org/10.3390/vaccines9020075
AMA Style
Li Z, Zhao Y, Li Y, Chen X. Adjuvantation of Influenza Vaccines to Induce Cross-Protective Immunity. Vaccines. 2021; 9(2):75. https://doi.org/10.3390/vaccines9020075
Chicago/Turabian StyleLi, Zhuofan, Yiwen Zhao, Yibo Li, and Xinyuan Chen. 2021. "Adjuvantation of Influenza Vaccines to Induce Cross-Protective Immunity" Vaccines 9, no. 2: 75. https://doi.org/10.3390/vaccines9020075
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.