
Pharmacokinetics and Safety of Doripenem in Healthy Chinese Subjects and Monte Carlo Dosing Simulations

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Demographics of Subjects and Safety
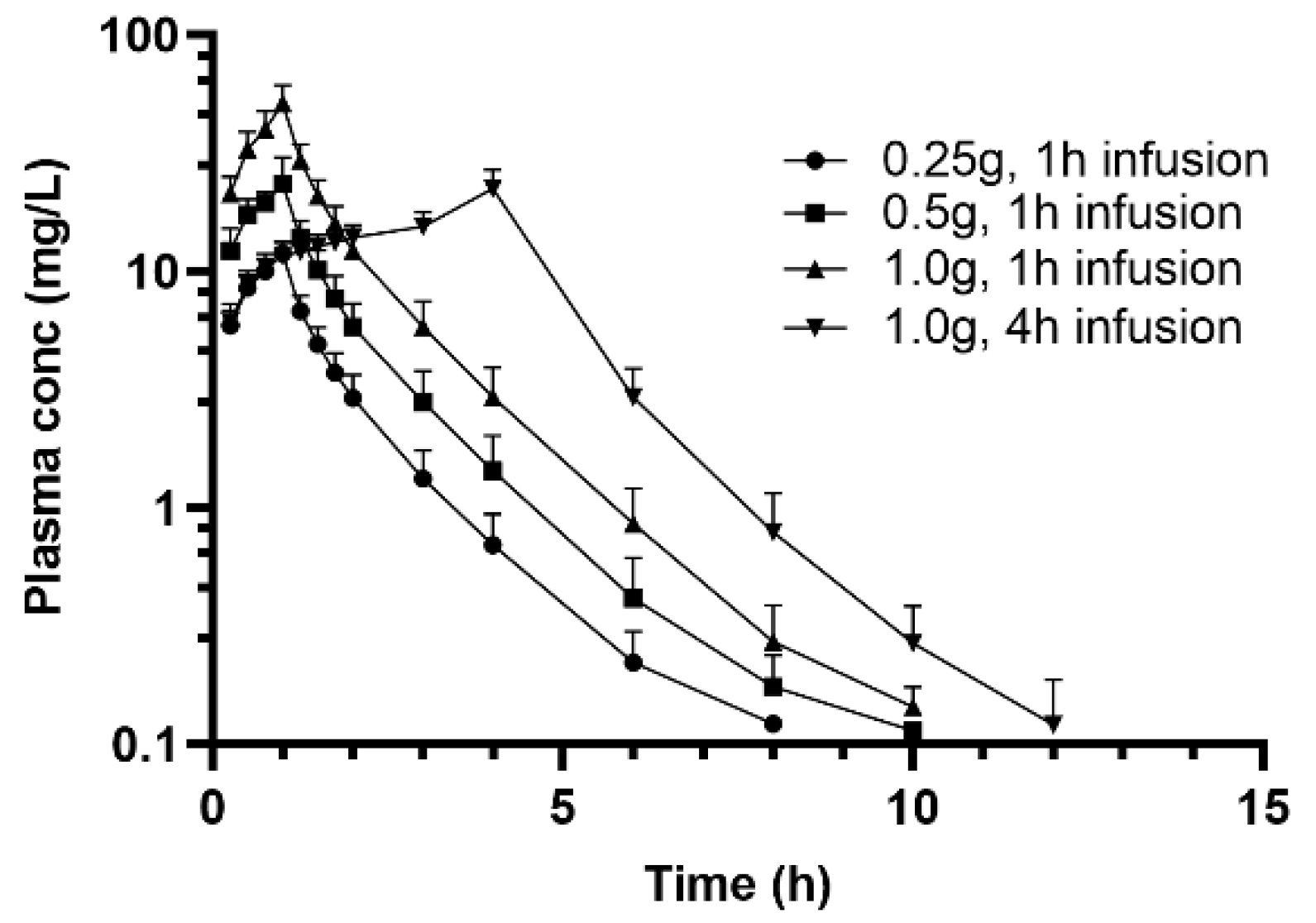
2.2. Non-Compartmental Analysis of Plasma Concentrations
2.3. Urinary Recovery
2.4. Population Pharmacokinetic Analysis
2.5. Pharmacokinetics/Pharmacodynamics
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Investigational Drug and Reference Standard Products
4.3. Pharmacokinetic Sampling
4.4. Determination of Doripenem Concentration in Plasma and Urine Samples
4.5. Pharmacokinetic and Pharmacokinetic/Pharmacodynamic Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ge, Y.; Wikler, M.A.; Sahm, D.F.; Blosser-Middleton, R.S.; Karlowsky, J.A. In vitro antimicrobial activity of doripenem, a new carbapenem. Antimicrob. Agents Chemother. 2004, 48, 1384–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chahine, E.B.; Ferrill, M.J.; Poulakos, M.N. Doripenem: A new carbapenem antibiotic. Am. J. Health Syst. Pharm. 2010, 67, 2015–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzei, T. The pharmacokinetics and pharmacodynamics of the carbapanemes: Focus on doripenem. J. Chemother. 2010, 22, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lv, Y.; Xue, F.; Zheng, B.; Liu, J.; Zhang, J. Antimicrobial resistance surveillance of doripenem in China. J. Antibiot. 2015, 68, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ko, K.S.; Song, J.H.; Peck, K.R. Antimicrobial activity of doripenem and other carbapenems against gram-negative pathogens from Korea. Microb. Drug Resist. 2011, 17, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Fritsche, T.R.; Stilwell, M.G.; Jones, R.N. Antimicrobial activity of doripenem (S-4661): A global surveillance report (2003). Clin. Microbiol. Infect. 2005, 11, 974–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betriu, C.; Gomez, M.; Lopez-Fabal, F.; Culebras, E.; Rodriguez-Avial, I.; Picazo, J.J. Activity of doripenem against extended-spectrum beta-lactamase-producing Enterobacteriaceae and Pseudomonas aeruginosa isolates. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1179–1181. [Google Scholar] [CrossRef]
- Nicola, F.; Garcia, R.D.; Arduino, S.; Di Chiara, M.; Smayevsky, J. In vitro activity of doripenem and other carbapenems against Pseudomonas aeruginosa. Rev. Argent. Microbiol. 2010, 42, 193–198. [Google Scholar]
- Lai, C.C.; Cheng, I.L.; Chen, Y.H.; Tang, H.J. The Efficacy and Safety of Doripenem in the Treatment of Acute Bacterial Infections—A Systemic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 958. [Google Scholar] [CrossRef] [Green Version]
- Lo, T.S.; Borchardt, S.M.; Welch, J.M.; Rohrich, M.A.; Alonto, A.M.; Alonto, A.V. Doripenem in hospital infections: A focus on nosocomial pneumonia, complicated intra-abdominal infections, and complicated urinary tract infections. Infect. Drug Resist. 2009, 2, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Shionogi, C. Finibax® for Injection, 2013-04 ed. Available online: https://www.shionogi.co.jp/med/interview/img/pdf/FBX.pdf (accessed on 15 January 2022).
- Cirillo, I.; Vaccaro, N.; Turner, K.; Solanki, B.; Natarajan, J.; Redman, R. Pharmacokinetics, safety, and tolerability of doripenem after 0.5-, 1-, and 4-hour infusions in healthy volunteers. J. Clin. Pharm. 2009, 49, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Choe, S.; Kim, D.J.; Zang, D.Y.; Lee, D.H. Pharmacokinetics of Doripenem in Healthy Koreans and Monte Carlo Simulations to Explore Optimal Dosage Regimens in Patients With Normal and Enhanced Renal Function. Drug Monit. 2018, 40, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Bhavnani, S.M.; Hammel, J.P.; Cirincione, B.B.; Wikler, M.A.; Ambrose, P.G. Use of pharmacokinetic-pharmaco dynamic target attainment analyses to support phase 2 and 3 dosing strategies for doripenem. Antimicrob. Agents Chemother. 2005, 49, 3944–3947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, I.; Mannens, G.; Janssen, C.; Vermeir, M.; Cuyckens, F.; Desai-Krieger, D.; Vaccaro, N.; Kao, L.M.; Devineni, D.; Redman, R.; et al. Disposition, metabolism, and excretion of [14C]doripenem after a single 500-milligram intravenous infusion in healthy men. Antimicrob. Agents Chemother. 2008, 52, 3478–3483. [Google Scholar] [CrossRef] [Green Version]
- Ikawa, K.; Morikawa, N.; Uehara, S.; Monden, K.; Yamada, Y.; Honda, N.; Kumon, H. Pharmacokinetic-pharmacodynamic target attainment analysis of doripenem in infected patients. Int. J. Antimicrob. Agents 2009, 33, 276–279. [Google Scholar] [CrossRef]
- Samtani, M.N.; Flamm, R.; Kaniga, K.; Nandy, P. Pharmacokinetic-pharmacodynamic-model-guided doripenem dosing in critically ill patients. Antimicrob. Agents Chemother. 2010, 54, 2360–2364. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Qin, Y.P.; Wang, Y.; Zheng, J.; Zhang, L.; Shu, S.Q.; Miao, J. Pharmacokinetics study of injected doripenemin healthy volunteers. Sichuan Da Xue Xue Bao Yi Xue Ban 2015, 46, 140–144. [Google Scholar]
- Harada, M.; Inui, N.; Suda, T.; Nakamura, Y.; Wajima, T.; Matsuo, Y.; Chida, K. Pharmacokinetic analysis of doripenem in elderly patients with nosocomial pneumonia. Int. J. Antimicrob. Agents 2013, 42, 149–154. [Google Scholar] [CrossRef]
- He, J.; Song, M.; Hang, T.; Li, K.; Zhang, A.; Luo, L.; Yang, L.; Wen, A. Pharmacokinetics of doripenem for injection in Chinese healthy volunteers. Chin. J. Antibiot. 2013, 38, 866–870. [Google Scholar] [CrossRef]
- Nandy, P.; Samtani, M.N.; Lin, R. Population pharmacokinetics of doripenem based on data from phase 1 studies with healthy volunteers and phase 2 and 3 studies with critically ill patients. Antimicrob. Agents Chemother. 2010, 54, 2354–2359. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, R.; Sato, Y.; Goto, K.; Yasuda, N.; Ohchi, Y.; Suzuki, Y.; Ueno, T.; Ito, K.; Kaneko, T.; Kurogi, S.; et al. Pharmacokinetic/Pharmacodynamic Analysis for Do.oripenem Regimens in Intensive Care Unit Patient. Biol. Pharm. Bull. 2017, 40, 1226–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, E.K.; Fleming, M.R.; Cheatham, S.C.; Kays, M.B. Population Pharmacokinetics and Pharmacodynamics of Doripenem in Obese, Hospitalized Patients. Ann. Pharm. 2017, 51, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Kays, M.B.; Fleming, M.R.; Cheatham, S.C.; Chung, E.K.; Juenke, J.M. Comparative pharmacokinetics and pharmacodynamics of doripenem and meropenem in obese patients. Ann. Pharm. 2014, 48, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Bhalodi, A.A.; Keel, R.A.; Quintiliani, R.; Lodise, T.P.; Nicolau, D.P.; Kuti, J.L. Pharmacokinetics of doripenem in infected patients treated within and outside the intensive care unit. Ann. Pharm. 2013, 47, 617–627. [Google Scholar] [CrossRef] [PubMed]
- FDA. DORIBAX® (Doripenem for Injection), 2015-08 ed. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/022106s015lbl.pdf (accessed on 15 January 2022).
- Wagenlehner, F.M.; Wagenlehner, C.; Redman, R.; Weidner, W.; Naber, K.G. Urinary bactericidal activity of Doripenem versus that of levofloxacin in patients with complicated urinary tract infections or pyelonephritis. Antimicrob. Agents Chemother. 2009, 53, 1567–1573. [Google Scholar] [CrossRef] [Green Version]
- Redman, R.; Damiao, R.; Kotey, P.; Kaniga, K.; Davies, T.; Naber, K.G. Safety and efficacy of intravenous doripenem for the treatment of complicated urinary tract infections and pyelonephritis. J. Chemother. 2010, 22, 384–391. [Google Scholar] [CrossRef]
- Cannavino, C.R.; Castaneda-Ruiz, B.; Redman, R.; Go, O.; Cirillo, I.; Barauskas, V.; Senatorova, G.; Emeryk, A.; Bradley, J.S. Safety and Tolerability of Doripenem in Hospitalized Children With Complicated Intra-Abdominal Infection, Complicated Urinary Tract Infections and Pneumonia. Pediatr. Infect. Dis. J. 2015, 34, 1264–1267. [Google Scholar] [CrossRef]
- Naber, K.G.; Llorens, L.; Kaniga, K.; Kotey, P.; Hedrich, D.; Redman, R. Intravenous doripenem at 500 milligrams versus levofloxacin at 250 milligrams, with an option to switch to oral therapy, for treatment of complicated lower urinary tract infection and pyelonephritis. Antimicrob. Agents Chemother. 2009, 53, 3782–3792. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.; Guo, Y.; Yang, Y.; Zheng, Y.; Wu, S.; Jiang, X.; Zhu, D.; Wang, F. Resistance reported from China antimicrobial surveillance network (CHINET) in 2018. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2275–2281. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | SD | |
|---|---|---|
| Gender | Male (n = 6), Female (n = 6) | |
| Age (years) | 30.5 | 7.17 |
| Height (cm) | 164 | 9.59 |
| Weight (kg) | 61.3 | 9.71 |
| BMI (kg/m2) | 22.8 | 2.08 |
| Ccr (mL/min) | 120 | 17.3 |
| Parameter | Unit | Doripenem Dose Group | |||
|---|---|---|---|---|---|
| 0.25 g, 1 h Infusion | 0.5 g, 1 h Infusion | 1.0 g, 1 h Infusion | 1.0 g, 4 h Infusion | ||
| Cmax | mg/L | 11.9 (1.43) | 23.9 (6.31) | 51.3 (9.82) | 22.3 (4.53) |
| Tmax | h | 0.975 (0.0716) | 0.932 (0.153) | 0.993 (0.0132) | 4 (0) |
| AUC0–8 h | h·mg/L | 17.5 (2.95) | 35.4 (7.18) | 72.4 (13.1) | 82.9 (12.1) |
| AUC0–24 h | h·mg/L | 17.3 (3.02) | 35.3 (7.38) | 72.7 (13.3) | 84.1 (12.5) |
| AUC0-inf | h·mg/L | 17.6 (2.99) | 35.6 (7.29) | 72.9 (13.3) | 84.4 (12.5) |
| AUCext | % | 2.13 (1.07) | 0.989 (0.862) | 0.405 (0.187) | 0.338 (0.0739) |
| T1/2 | h | 1.06 (0.127) | 1.10 (0.255) | 1.15 (0.147) | 1.14 (0.213) |
| MRT | h | 1.04 (0.16) | 1.05 (0.2) | 1.1 (0.152) | 1.23 (0.115) |
| CL | L/h | 14.5 (2.26) | 14.5 (2.60) | 14.1 (2.38) | 12.1 (1.76) |
| Vd | L | 22.1 (3.18) | 22.8 (6.56) | 23.1 (4.14) | 19.9 (4.85) |
| CLr | L | 9.87 (1.75) | 10.4 (1.76) | 9.87 (2.46) | 8.21 (1.48) |
| Time | Doripenem Concentration (mg/L) | |||
|---|---|---|---|---|
| 0.25 g, 1 h Infusion | 0.5 g, 1 h Infusion | 1.0 g, 1 h Infusion | 1.0 g, 4 h Infusion | |
| 0–2 h | 667 (535) | 974 (745) | 2674 (1888) | 1936 (996) |
| 2–4 h | 132 (57) | 296 (202) | 636 (339) | |
| 4–8 h | 31.7 (18.9) | 59.2 (34.5) | 119.4 (78.8) | 514 (266) |
| 8–12 h | 3.34 (2.62) | 4.05 (1.71) | 10.1 (8.27) | 34.9 (25.8) |
| 12–24 h | 0.304 (0.139) | 0.676 (0.517) | 1.27 (0.775) | 2.73 (2.63) |
| 0–24 h | ND | ND | ND | ND |
| Parameter | Estimate | Between-Subject Variability | ||
|---|---|---|---|---|
| Original Dataset (Typical Value) | Bootstrap Dataset (Median and 95% Interval Confidence) | Original Dataset (%) | Bootstrap Dataset (%) | |
| CL (L/h) | 14.2 | 14.2 (12.9, 15.5) | 15.1 | 14.4 |
| Vc (L) | 8.17 | 8.20 (7.42, 8.67) | 15.3 | 14.3 |
| Q (L/h) | 8.54 | 8.59 (7.30, 9.72) | 0 (FIX) | \ |
| Vp (L) | 6.95 | 6.95 (6.24, 7.58) | 7.37 | 6.70 |
| θBW on Vp | 0.713 | 0.700 (0.246, 0.987) | NA | NA |
| Proportional Error (%) | 12.1 | 12.0 (10.4, 13.7) | NA | NA |
| Additive Error (%) | 3.76 | 3.71 (2.59, 5.54) | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Liu, X.; Li, K.; Fan, Y.; Yu, J.; Wu, H.; Li, Y.; Wu, X.; Guo, B.; Li, X.; et al. Pharmacokinetics and Safety of Doripenem in Healthy Chinese Subjects and Monte Carlo Dosing Simulations. Antibiotics 2022, 11, 958. https://doi.org/10.3390/antibiotics11070958
Wang Y, Liu X, Li K, Fan Y, Yu J, Wu H, Li Y, Wu X, Guo B, Li X, et al. Pharmacokinetics and Safety of Doripenem in Healthy Chinese Subjects and Monte Carlo Dosing Simulations. Antibiotics. 2022; 11(7):958. https://doi.org/10.3390/antibiotics11070958
Chicago/Turabian StyleWang, Yu, Xiaofen Liu, Kun Li, Yaxin Fan, Jicheng Yu, Hailan Wu, Yi Li, Xiaojie Wu, Beining Guo, Xin Li, and et al. 2022. "Pharmacokinetics and Safety of Doripenem in Healthy Chinese Subjects and Monte Carlo Dosing Simulations" Antibiotics 11, no. 7: 958. https://doi.org/10.3390/antibiotics11070958