Comparison of Lys ,Pro -Human Insulin Analog and ... - Diabetes Care
Comparison of Lys ,Pro -Human Insulin Analog and ... - Diabetes Care
Comparison of Lys ,Pro -Human Insulin Analog and ... - Diabetes Care

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
S H O R T R E P O R T<br />
<strong>Comparison</strong> <strong>of</strong> <strong>Lys</strong> B28 ,<strong>Pro</strong> B29 -<strong>Human</strong><br />
<strong>Insulin</strong> <strong>Analog</strong> <strong>and</strong> Regular <strong>Human</strong><br />
<strong>Insulin</strong> in the Correction <strong>of</strong> Incidental<br />
Hyperglycemia<br />
FRITS HOLLEMAN, MD<br />
JOOPJ.G. VAN DEN BRAND, MSC<br />
ROLAND A.R.A. HOVEN, MSC<br />
Jos M. VAN DER LINDEN, MA<br />
INGEBORG VAN DER TWEEL<br />
JOOST B.L. HOEKSTRA, MD, PHD<br />
D. WLLLEM ERKELENS, MD, PHD<br />
OBJECTIVE — To obtain clinically applicable data on the effects <strong>of</strong> regular human insulin<br />
<strong>and</strong> the <strong>Lys</strong> B28 ,<strong>Pro</strong> B29 -human insulin analogue (lispro) on the correction <strong>of</strong> incidental hyperglycemia.<br />
RESEARCH DESIGN AND METHODS— The insulins were compared in a nonclamped<br />
r<strong>and</strong>omized crossover study <strong>of</strong> 27 male IDDM patients. Hyperglycemia was induced<br />
by the withdrawal <strong>of</strong> the normal evening dose <strong>of</strong> insulin; the next morning patients fasted <strong>and</strong><br />
received a single dose <strong>of</strong> study insulin according to a dosing nomogram. Blood glucose concentration<br />
<strong>and</strong> GR (a measure <strong>of</strong> glucose corrected for differences in administered insulin dose:<br />
GR = glucose concentration X BMI X insulin dose"" 1 ) were followed for 4 h.<br />
RESULTS — The time courses <strong>of</strong> blood glucose concentration <strong>and</strong> GR were significantly different<br />
after regular insulin in comparison with lispro (multiple analysis <strong>of</strong> variance, P <<br />
0.001). At t = 120 min, glucose concentrations had decreased 1.4 mmol/1 more with lispro than<br />
with regular insulin (95% confidence interval [CI] 0.6-2.3, P = 0.002). Similarly, GR had<br />
decreased 4.4 mol • kg • IU" 1 • m~ 5 more with lispro than with regular insulin (95% CI<br />
2.6-6.2, P < 0.001). The overall difference in glucose values was 0.87 mmol/1 (lispro < regular<br />
insulin, P = 0.036), <strong>and</strong> the overall difference in GR values was 1.96 mol • kg • 1U" 1 • m~ 5<br />
(lispro < regular insulin, P = NS). Unexpectedly, the intrinsic variability <strong>of</strong> GR was higher for<br />
lispro than for regular insulin.<br />
CONCLUSIONS — The more rapid action <strong>of</strong> lispro is an advantage in the correction <strong>of</strong><br />
hyperglycemia, even though actual differences in glucose concentrations are smaller than<br />
suggested by previous clamped studies.<br />
The rapid <strong>and</strong> sufficient correction <strong>of</strong><br />
incidental hyperglycemia is hampered<br />
by the long duration <strong>of</strong> action<br />
<strong>of</strong> regular human insulin <strong>and</strong> the inability<br />
to predict the effect <strong>of</strong> a certain amount <strong>of</strong><br />
regular human insulin on blood glucose<br />
levels. The latter problem can largely be<br />
attributed to the high inter- <strong>and</strong> intra-individual<br />
variability in the absorption <strong>of</strong> reg-<br />
ular human insulin after subcutaneous<br />
injection (1-4).<br />
It would seem theoretically plausible<br />
that monomeric insulins, such as the<br />
<strong>Lys</strong> B28 ,<strong>Pro</strong> B29 -human insulin analog (lispro),<br />
show less variability in absorption than<br />
hexameric regular insulin (5). Such insulins<br />
could result in more clinically predictable<br />
behavior <strong>and</strong> possibly even a linear dose-<br />
From the Department <strong>of</strong> Internal Medicine (EH., J.J.G.B., R.A.R.A.H., J.B.L.H.), Diakonessenhuis, Utrecht;<br />
Eli Lilly <strong>and</strong> Company (J.M.L), Nieuwegein; Center for Biostatistics (IT.), Utrecht University, Utrecht; the<br />
Department <strong>of</strong> Internal Medicine (D.WE.), University Hospital, Utrecht, The Netherl<strong>and</strong>s.<br />
Address correspondence <strong>and</strong> reprint requests to Frits Holleman, MD, Department <strong>of</strong> Internal Medicine,<br />
Diakonessenhuis, Bosboomstraat 1, 3582 KE Utrecht, The Netherl<strong>and</strong>s.<br />
Received for publication 31 January 1996 <strong>and</strong> accepted in revised form 25 July 1996.<br />
(jR, relative measure <strong>of</strong> glucose; lispro, <strong>Lys</strong> B28 ,<strong>Pro</strong> B2c) -human insulin analog; MANOVA, multiple analysis<br />
<strong>of</strong> variance.<br />
effect relationship. The results <strong>of</strong> glucose<br />
clamp studies by Woodworth et al. (6) <strong>and</strong><br />
Antsiferov et al. (7) seem to support this<br />
hypothesis. However, the practical applicability<br />
<strong>of</strong> these results is difficult to ascertain<br />
(5,8,9).<br />
This study was designed to compare<br />
the decrease in glucose concentrations<br />
after the subcutaneous administration <strong>of</strong><br />
lispro <strong>and</strong> regular human insulin in a setting<br />
as close as possible to naturally occurring<br />
hyperglycemia. By using a well-controlled<br />
double-blind cross-over design, we<br />
tried to eliminate potential confounding<br />
factors.<br />
RESEARCH DESIGN AND<br />
METHODS — This study was approved<br />
by the Institutional Ethical Review Board.<br />
Informed consent was obtained from all<br />
participants. The trial was conducted<br />
according to the European Good Clinical<br />
Practice guidelines.<br />
A total <strong>of</strong> 27 healthy male IDDM<br />
patients aged 20-65 years with HbAlc<br />
Table 1—Dosing nomogram<br />
Glucose<br />
range<br />
(mmol/1)<br />
05-10<br />
10-15<br />
15-18<br />
18-21<br />
21-24<br />
24-27<br />
27-30<br />
<strong>Insulin</strong> dosage<br />
per kg/m 2<br />
0.1<br />
0.2<br />
0.3<br />
0.4<br />
0.5<br />
0.6<br />
0.7<br />
(NovoFine, Novo Nordisk, Bagsvaerd, Denmark).<br />
The pens were prefilled, blinded,<br />
<strong>and</strong> sealed by the hospital pharmacist.<br />
Venous blood samples were taken at t<br />
- 20, 40, 60, 90, 120, 150, 180, 210, <strong>and</strong><br />
240 min postinjection. Whole blood glucose<br />
was measured using an APEC glucose<br />
analyzer (Danvers, MA). HbAlc was measured<br />
using high-performance liquid chromatography<br />
(Biograd, Anaheim, CA).<br />
Since the insulin dosages were determined<br />
by the nomogram, we decided to<br />
obtain a relative measure which expresses<br />
the fall in glucose in such a way that it corrects<br />
for the differences in the BMI <strong>and</strong> the<br />
administered dose. This relative measure<br />
<strong>of</strong> glucose, GR (mol • kg • IU" 1 • m~ 5 ), was<br />
calculated by dividing the glucose values<br />
(in millimoles per liter) at all time points<br />
by the insulin dose actually administered<br />
(in international units) <strong>and</strong> multiplying<br />
this figure with the measured BMI (in kilograms<br />
per meters squared).<br />
Data were statistically analyzed using<br />
the SPSS computer program.<br />
Differences between the time course <strong>of</strong><br />
lispro <strong>and</strong> regular human insulin were evaluated<br />
using an analysis <strong>of</strong> variance with<br />
repeated measures. The within-patient variability<br />
was defined as the square root <strong>of</strong> the<br />
error variance after the correction for the<br />
decrease <strong>of</strong> the GR values in time.<br />
RESULTS— The participants had a<br />
median age <strong>of</strong> 34 years (range, 20-60<br />
years), a median duration <strong>of</strong> diabetes <strong>of</strong> 8<br />
years (range, 0-30 years), an average<br />
HbAlc <strong>of</strong> 7.7 ± 1.1%, <strong>and</strong> a BMI <strong>of</strong> 24.4 ±<br />
1.7 kg/m 2 . Thirteen patients were r<strong>and</strong>omized<br />
to the lispro-regular insulin<br />
sequence, <strong>and</strong> fourteen were r<strong>and</strong>omized<br />
to the regular-lispro insulin sequence.<br />
There were no significant differences in<br />
baseline characteristics. The average dose<br />
<strong>of</strong> insulin administered was 7.9 ± 3.5 IU<br />
2<br />
Absolute dose (IU) <strong>of</strong> insulin administered by BMI (kg/m )<br />
20 21 22 23 24 25 26 27<br />
2 2 2 2 2 2 3 3<br />
4 4 4 5 5 5 5 5<br />
6 6 7 7 7 7 8 8<br />
8 8 9 9 10 10 10 11<br />
10 10 11 11 12 12 13 14<br />
12 13 14 14 14 15 16 16<br />
14 15 15 16 17 17 18 19<br />
<strong>of</strong> regular human insulin <strong>and</strong> 7.9 ± 3.7 IU<br />
<strong>of</strong> lispro.<br />
The initial glucose values for regular<br />
human insulin ([Glue], = 0, reg) an d lispro<br />
([Gluc]( = 0 us) were 16.7 ± 4.7 mmol/1 <strong>and</strong><br />
16.4 ± 5.4 mmol/1, respectively. Four<br />
hours after injection, [Glue], = 240, a-g was<br />
8.7 ± 2.3 mmol/1, <strong>and</strong> [Gluc], = 24o, us was<br />
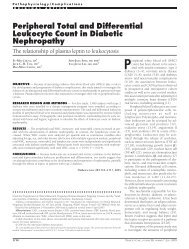
8.5 ± 2.5 mmol/1. The average values for<br />
glucose concentration are plotted against<br />
time in Fig. 1.<br />
The differences in glucose values<br />
between regular human insulin <strong>and</strong> lispro<br />
were dependent on time (multiple analysis<br />
<strong>of</strong> variance [MANOVA], P < 0.001).<br />
Overall, the average difference between<br />
[Gluc]reg <strong>and</strong> [GlucJiis from t = 0 min to t =<br />
240 min using MANOVA was 0.87<br />
mmol/1 (lispro < regular human insulin,<br />
95% CI 0.07-1.68, P = 0.036). The average<br />
fall in glucose concentration from t = 0<br />
min to t = 120 min was 4.8 mmol/1 for reg-<br />
24,0<br />
20,0<br />
16,0<br />
12,0<br />
I 4,0<br />
><br />
0,0<br />
0 20 40 60 80<br />
Figure 1—Glucose concentrations (means<br />
according to the nomogram at t = 0 min.<br />
<<br />
4<br />
<<br />
Holleman <strong>and</strong> Associates<br />
ular human insulin <strong>and</strong> 6.2 mmol/1 for<br />
lispro (95% CI 0.6-2.3, P - 0.002).<br />
At each time point after t = 60 min, a<br />
good correlation coefficient was found for<br />
the individual fall in glucose concentration<br />
plotted against the dose <strong>of</strong> insulin administered<br />
per kilograms per meters squared<br />
(all r > 0.89 <strong>and</strong> P < 0.001) for both regular<br />
human insulin <strong>and</strong> lispro.<br />
The relative measure <strong>of</strong> glucose, GR<br />
(mol • kg • IU" 1 • m ~0, at t -•• 0 min was<br />
55.2 ± 12.5 mol • kg • IU ! • m ' for regular<br />
human insulin <strong>and</strong> 54.7 ± 10.2 mol •<br />
kg • IU" 1 • m~ 5 for lispro. At t - 240 min,<br />
GR,K8 was 30.3 ±11.9 mol • kg • IU ' •<br />
m~ 5 <strong>and</strong> GRiiLS was 31.6 ± 15.1 mol • kg •<br />
IU" 1 • m" 5 . The average values <strong>of</strong> GR are<br />
represented in Fig. 2.<br />
Again, differences between regular<br />
human insulin <strong>and</strong> lispro were timedependent<br />
(P < 0.001). Overall, the average<br />
difference between GRrc,, <strong>and</strong> GRj,s<br />
from t = 0 min to t = 240 min using<br />
MANOVA was 1.96 mol • kg • IU ' • m *<br />
(lispro < regular human insulin, 95% CI<br />
-3.25-7.18, P = 0.45). The average fall in<br />
GR from t = 0 min to t = 120 min was 14.9<br />
mol • kg • IU" 1 • m" i for regular human<br />
insulin <strong>and</strong> 19.3 mol • kg • IU ' • m ' for<br />
lispro (95% CI 2.6-6.2, P < 0.001).<br />
The within-patient variability <strong>of</strong> all<br />
values <strong>of</strong> GR from t = 0 min to t = 240 min<br />
was 2.68 mol • kg • IU" 1 • m ' for regular<br />
human insulin <strong>and</strong> 3.58 mol • kg • IU ' •<br />
m~ 5 for lispro. The within-patient variability<br />
<strong>of</strong> the values <strong>of</strong> GR from t - 0 min to t -<br />
120 min was 2.25 mol • kg • IU ' • m '<br />
A<br />
4<br />
*- .<br />
100 120 140<br />
time (min.)<br />
•<br />
" .<br />
i<br />
<<br />
— •<br />
Li .pro<br />
Hi lmuli iR<br />
— —<br />
><br />
^—+ ,<br />
><br />
- A -<br />
160 180 200 220 240<br />
SD) after the administration <strong>of</strong> the study insulins<br />
DIABKTES CARE, VOLUME 19, NUMBER 12, DECEMBER 1996 1427<br />
•
<strong>Comparison</strong> <strong>of</strong> regular human insulin <strong>and</strong> lispro<br />
70,0<br />
60,0<br />
^50,0<br />
40,0<br />
30,0<br />
20,0<br />
10,0<br />
0,0<br />
<<br />
i<br />
<<br />
A<br />
i I<br />
•<br />
•<br />
i<br />
< i<br />
- —<br />
A<br />
•—-.<br />
— • -^ ^ • .<br />
' *<br />
< ><br />
—•<br />
Li spro<br />
—*<br />
Hi imuli lR<br />
0 20 40 60 80 100 120 140 160 180 200 220 240<br />
time (min.)<br />
Figure 2—Values o/GR (means ± SD) after the administration <strong>of</strong> the study insulins according to the<br />
nomogram att = O min.<br />
for regular human insulin <strong>and</strong> 2.68 mol •<br />
kg • IU" 1 • m" 5 for lispro.<br />
The fall in glucose concentration at a<br />
given time point that would be the result<br />
<strong>of</strong> the administration <strong>of</strong> 1 IU insulin per<br />
kg/m 2 at t = 0 min can be expressed as<br />
AGR. The differential <strong>of</strong> the fall in GR<br />
against time, AGR/A,, is a representation <strong>of</strong><br />
the in vivo time-action pr<strong>of</strong>ile <strong>of</strong> the<br />
administered insulins (Fig. 3).<br />
CONCLUSIONS— In this study, we<br />
used a relative measure <strong>of</strong> glucose, GR, that<br />
expresses the decrease in glucose concentration<br />
per 1 IU/BMI. This mathematical<br />
conversion might not be justified if, as<br />
13<br />
0,25<br />
§0,05<br />
0,00<br />
L<br />
JA<br />
\<br />
r-A V\<br />
1<br />
1<br />
published observations indicate (6,10),<br />
increased doses <strong>of</strong> regular insulin result in<br />
relatively decreasing effects on glucose disposal.<br />
However, we found linear correlations<br />
between the administered dose per<br />
kg/m 2 <strong>and</strong> the fall in glucose for regular<br />
human insulin <strong>and</strong> lispro, supporting the<br />
feasibility <strong>of</strong> our approach.<br />
The total decrease in glucose concentration<br />
<strong>and</strong> GR over 240 min was similar<br />
for both insulins, though there seems to be<br />
a residual effect <strong>of</strong> regular human insulin<br />
that lasts beyond 240 min (Figs. 2 <strong>and</strong> 3).<br />
The time courses <strong>of</strong> regular human insulin<br />
<strong>and</strong> lispro were significantly different. As<br />
illustrated in Figs. 2 <strong>and</strong> 3, the effect per<br />
\<br />
\<br />
Ns<br />
-*<br />
Li spro<br />
—*<br />
H jmuli riR<br />
0 20 40 60 80 100 120 140 160 180 200 220 240<br />
time (min.)<br />
Figure 3—The differential curve <strong>of</strong> AGR against time, AGR/A,, representing the time-action pr<strong>of</strong>iles<br />
<strong>of</strong> the studied insulins.<br />
•<br />
•<br />
IU/BMI in the first 120-min period was<br />
significantly higher for lispro than for regular<br />
human insulin. Also, the peak effect <strong>of</strong><br />
lispro, as reflected in AGR/A(, was about<br />
150% <strong>of</strong> the peak effect <strong>of</strong> regular human<br />
insulin. These results are compatible with<br />
previously published data on lispro<br />
(6,7,11-14).<br />
From a clinical point <strong>of</strong> view, the differences<br />
in the decrease <strong>of</strong> glucose<br />
between regular human insulin <strong>and</strong> lispro<br />
are modest: maximally ~1.4 mmol/1 at t =<br />
120 min. The overall difference during the<br />
whole time period was less (~0.9<br />
mmol/1), while the difference in GR (~2<br />
mol • kg • IU" 1 • m~ 5 ) was not even<br />
significant. Thus, it must be emphasized<br />
that large differences in insulin concentrations<br />
or glucose infusion rates found in<br />
previous clamp studies do not imply similarly<br />
large differences in glucose concentration.<br />
This may partly explain why the<br />
use <strong>of</strong> lispro, despite its more physiological<br />
insulin pr<strong>of</strong>ile, has not yet led to major<br />
improvements in HbAlc.<br />
We unexpectedly found a higher<br />
within-patient variability for lispro than<br />
for regular human insulin, even when we<br />
restricted our analysis to the first 120-min<br />
period.<br />
Given the time frame <strong>and</strong> the r<strong>and</strong>omization<br />
procedure used, these differences<br />
can hardly be attributed to the<br />
residual effects <strong>of</strong> the patients' own<br />
insulin. Maybe the uniformly monomeric<br />
state makes the diffusion <strong>of</strong> lispro more<br />
susceptible to subtle changes in local<br />
blood flow than the diffusion <strong>of</strong> regular<br />
insulin, which is buffered by the equilibrium<br />
mixture <strong>of</strong> monomeric <strong>and</strong> polymeric<br />
forms. However, given the conflicting<br />
results <strong>of</strong> Antsiferov (7), this point<br />
requires further investigation.<br />
In conclusion, as in most other studies,<br />
the lispro insulin analog showed a<br />
more rapid action pr<strong>of</strong>ile than regular<br />
human insulin. Lispro resulted in lower<br />
overall glucose values, but had a higher<br />
within-patient variability than regular<br />
human insulin. The absolute differences in<br />
effect on glucose for regular human<br />
insulin <strong>and</strong> lispro were not very large. Still,<br />
the early termination <strong>of</strong> insulin action is an<br />
advantage in the rapid <strong>and</strong> safe correction<br />
<strong>of</strong> incidental hyperglycemia.<br />
Acknowledgments— This study was financially<br />
supported by the Dutch branch <strong>of</strong> Eli Lilly<br />
& Company, Nieuwegein, The Netherl<strong>and</strong>s.<br />
1428 DIABETES CARE, VOLUME 19, NUMBER 12, DECEMBER 1996
References<br />
1. Binder C, Lauritzen T, Faber O, Pramming<br />
S: <strong>Insulin</strong> pharmacokinetics. <strong>Diabetes</strong> <strong>Care</strong><br />
7:188-199,1984<br />
2. Lauritzen T: Pharmacokinetic <strong>and</strong> clinical<br />
aspects <strong>of</strong> intensified subcutaneous insulin<br />
therapy. PhD thesis. Copenhagen, Denmark,<br />
University <strong>of</strong> Copenhagen, 1985<br />
3. Skyler JS: <strong>Insulin</strong> pharmacology. Med Clin<br />
North Am 72:1337-1354,1988<br />
4. De Meijer PHEM, Lutterman JA, van't Laar<br />
A: The absorption <strong>of</strong> subcutaneously<br />
injected insulin. Neth] Med 34:210-227,<br />
1989<br />
5. Furler SM, Kraegen EW: Quantitative<br />
aspects <strong>of</strong> subcutaneous insulin absorption.<br />
Diabetic Med 6:657-665, 1989<br />
6. Woodworth J, Howey D, Lutz S, Santa P,<br />
Brady P, Bowsher R: [LYS(B28),<br />
PRO(B29)] human insulin: dose ranging<br />
versus Humulin R. Diabetologia 36 (Suppl.<br />
1):A155,1993<br />
7. Antsiferov M, Woodworth JR, Mayorov A,<br />
Ristic S, Dedov I: Lower within patient<br />
variability in post-pr<strong>and</strong>ial glucose-excursion<br />
with lispro insulin analog compared<br />
with regular insulin. <strong>Diabetes</strong> 44 (Suppl.<br />
1):214A, 1995<br />
8. Boyle PJ: Glucose clamp investigations: the<br />
ups <strong>and</strong> downs. <strong>Diabetes</strong> <strong>Care</strong> 17:239-<br />
241, 1994<br />
9. DeFronzo RA, Tobin JD, Andres R: Glucose<br />
clamp technique: a method for quantifying<br />
insulin secretion <strong>and</strong> resistance. Am<br />
J Physiol 237(3):E214-E223, 1979<br />
10. Heinemann L, Richter B: Clinical pharmacology<br />
<strong>of</strong> human insulin. <strong>Diabetes</strong> <strong>Care</strong> 16<br />
(Suppl. 3):90-100, 1993<br />
11. Ter Braak EWMT, Bianchi R, Erkelens<br />
DW: More suitable action pr<strong>of</strong>ile for premeal<br />
treatment <strong>of</strong> <strong>Lys</strong>(B28)<strong>Pro</strong>(B29)<br />
Holleman <strong>and</strong> Associates<br />
insulin analogue than regular insulin. Diabetologia<br />
36 (Suppl. l):A30,1993<br />
12. Radziuk J, Davies J, Pye S, DiMarchi R,<br />
Shields J, Chance R: Subcutaneous<br />
absorption <strong>of</strong> fast-acting insulin analogs:<br />
kinetics <strong>and</strong> bio-effectiveness. Diabetologia<br />
35 (Suppl. 1):A3,1992<br />
13. Howey DC, Bowsher RR, Brunelle RL,<br />
Woodworth JR: [<strong>Lys</strong>(B28), <strong>Pro</strong>(B29)]human<br />
insulin: a rapidly absorbed analogue<br />
<strong>of</strong> human insulin. <strong>Diabetes</strong><br />
43:396-402,1994<br />
14. Torlone E, Fanelli C, Rambotti AM, Kassi<br />
G, Modarelli F, Di Vincenzo A, Epifano L,<br />
Ci<strong>of</strong>etta M, Pampanelli S, Brunetti P, Bolli<br />
GB: Pharmacokinetics, pharmacodynamics<br />
<strong>and</strong> glucose-counterregulation following<br />
subcutaneous injection <strong>of</strong> the<br />
monomeric insulin analogue [<strong>Lys</strong>(B28),<br />
<strong>Pro</strong>(B29)] in IDDM. Diabetologia 37:713-<br />
720,1994<br />
DIABETES CARE, VOLUME 19, NUMBER 12, DECEMBER 1996 1429