clerkship handbook - University of Hawaii â Department of Medicine
clerkship handbook - University of Hawaii â Department of Medicine
clerkship handbook - University of Hawaii â Department of Medicine

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
UNIVERSITY OF HAWAII<br />
JOHN A. BURNS SCHOOL OF MEDICINE<br />
DEPARTMENT OF MEDICINE<br />
THIRD-YEAR CLERKSHIP IN<br />
INTERNAL MEDICINE<br />
MEDICINE 531 (6B)<br />
MEDICINE 532 (6L)<br />
CLERKSHIP HANDBOOK<br />
Revised 02/25/13<br />
1
TABLE OF CONTENTS<br />
CONTACT INFORMATION ................................................................................................................................................... 3<br />
SUMMARY TABLE OF CLERKSHIP REQUIREMENTS ................................................................................................. 4<br />
TOP 10 WAYS TO EXCEL ON THE INTERNAL MEDICINE CLERKSHIP ................................................................. 5<br />
DESCRIPTION OF THE THIRD-YEAR CLERKSHIP IN INTERNAL MEDICINE ...................................................... 6<br />
INTRODUCTION ..................................................................................................................................................................... 6<br />
Goal <strong>of</strong> the Clerkship ........................................................................................................................................ 6<br />
Design <strong>of</strong> the Clerkship .................................................................................................................................... 6<br />
Work Hours, Designated Study Time, Days Off and Holidays ..................................................................... 6<br />
Absences ........................................................................................................................................................... 7<br />
CURRICULUM ....................................................................................................................................................... 8<br />
Learning Objectives .......................................................................................................................................... 9<br />
Learning Strategies .......................................................................................................................................... 9<br />
EVALUATION IN THE THIRD-YEAR CLERKSHIP IN INTERNAL MEDICINE ..................................................... 9<br />
General Guidelines ........................................................................................................................................... 9<br />
Retaking Exams .............................................................................................................................................. 10<br />
Honors.............................................................................................................................................................. 10<br />
SPECIFIC REQUIREMENTS AND GUIDELINES................................................................................................ 12<br />
Inpatient <strong>Medicine</strong> ........................................................................................................................................... 12<br />
Ambulatory <strong>Medicine</strong> ...................................................................................................................................... 16<br />
PBL Tutorial ..................................................................................................................................................... 18<br />
Role Descriptions for <strong>Medicine</strong> 531/532 ....................................................................................................... 19<br />
MISCELLANEOUS CLERKSHIP INFORMATION ......................................................................................................... 24<br />
GUIDELINES FOR APPROPRIATE APPEARANCE AND ATTIRE .................................................................... 25<br />
RECOMMENDED RESOURCES ......................................................................................................................... 26<br />
REQUIRED EQUIPMENT .................................................................................................................................... 27<br />
EXPOSURE TO BLOOD/BODY FLUIDS PROTOCOL ....................................................................................... 28<br />
HIV MEDICINE ..................................................................................................................................................... 29<br />
MEDICINE T-RES INSTRUCTIONS .................................................................................................................... 32<br />
STUDENT EVALUATION OF TEACHERS .......................................................................................................... 34<br />
EVALUATION FORMS ......................................................................................................................................................... 35<br />
OBSERVED HISTORY AND PHYSICAL ............................................................................................................. 36<br />
THE BASIC PHYSICAL EXAMINATION SEQUENCE (BPES) ........................................................................... 37<br />
OBSERVED PATIENT COUNSELING ................................................................................................................ 48<br />
CASE PRESENTATION ....................................................................................................................................... 49<br />
SMALL GROUP LEARNING EXPERIENCE ....................................................................................................... 50<br />
MID-CLEKSHIP FEEDBACK FORM ................................................................................................................... 51<br />
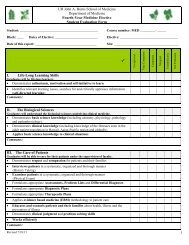
STUDENT EVALUATION FORM ......................................................................................................................... 52<br />
OTHER FORMS ...................................................................................................................................................................... 56<br />
INPATIENT MEDICINE AGREEMENT FORM ..................................................................................................... 57<br />
INPATIENT WORK HOURS LOG ........................................................................................................................ 59<br />
PHYSICIAN’S ORDERS ...................................................................................................................................... 60<br />
APPENDICES .......................................................................................................................................................................... 61<br />
TRAINING PROBLEMS LIST .............................................................................................................................. 62<br />
GENERAL CLINICAL CORE COMPETENCIES IN INTERNAL MEDICINE ..................................................... 192<br />
LIST OF ERROR-PRONE ABBREVIATIONS, SYMBOLS, AND DOSE DESIGNATIONS ............................... 234<br />
COMPREHENSIVE WRITE-UPS ....................................................................................................................... 238<br />
Definition <strong>of</strong> Comprehensive Write-up ....................................................................................................... 238<br />
Submission Requirements <strong>of</strong> Comprehensive Write-ups ........................................................................ 238<br />
Example <strong>of</strong> Inpatient History and Physical ................................................................................................ 239<br />
Example <strong>of</strong> Ambulatory Note ....................................................................................................................... 246<br />
CLINICAL SKILLS EXAMINATION (CSE) ........................................................................................................ 251<br />
NBME SUBJECT EXAM IN INTERNAL MEDICINE .......................................................................................... 256<br />
2
CONTACT INFORMATION<br />
Clerkship Director<br />
Clerkship Coordinator:<br />
Hospital Site Coordinators:<br />
Laurie M. Tam, M.D., F.A.C.P.<br />
Assistant Pr<strong>of</strong>essor <strong>of</strong> <strong>Medicine</strong><br />
1356 Lusitana Street, 7 th Fl.,<br />
Honolulu, HI 96813<br />
Telephone: (808) 586-7460 FAX: 586-7486<br />
e-mail: lmtam@hawaii.edu<br />
Ms. Julieta Rajlevsky<br />
1356 Lusitana Street, 7 th Fl.<br />
Honolulu, HI 96813<br />
Telephone: (808) 586-7478 FAX: 586-7486<br />
e-mail: jlrajlev@hawaii.edu<br />
Queens Medical Center:<br />
Miki Kiyokawa, M.D.<br />
Assistant Pr<strong>of</strong>essor <strong>of</strong> <strong>Medicine</strong><br />
QET9, 1301 Punchbowl Street,<br />
Honolulu, HI 96813<br />
Telephone: 586-2910 FAX: 586-7486<br />
e-mail: kmcsitecoordinator@yahoo.com<br />
Kuakini Medical Center:<br />
Miki Kiyokawa, M.D.<br />
Assistant Pr<strong>of</strong>essor <strong>of</strong> <strong>Medicine</strong><br />
Office <strong>of</strong> Medical Education<br />
347 N. Kuakini St., Honolulu, HI 96817<br />
Telephone: 547-9226 FAX: 547-9867<br />
e-mail: kmcsitecoordinator@yahoo.com<br />
Tripler Army Medical Center:<br />
Bethany Sonobe, MD<br />
Internal <strong>Medicine</strong><br />
Telephone: 433-2638 Pager: 363-1423<br />
e-mail: bethany.sonobe@amedd.army.mil<br />
3
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
SUMMARY TABLE OF CLERKSHIP REQUIREMENTS<br />
Inpatient Ambulatory<br />
1. Call<br />
a. Every time your team is on call 6B & 6L -<br />
6B & 6L<br />
-<br />
b. Overnight call once (preferably Friday night)<br />
at KMC<br />
2. Comprehensive Write-ups<br />
a. 1 Comprehensive Write-up per week<br />
6B & 6L<br />
(3 - 6 total)<br />
b. 2 Comprehensive Write-ups per week (10 total) 6B<br />
c. 2 Comprehensive Write-ups per month (10 total) - 6L<br />
3. Required Clerkship Activities<br />
a. UH <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> Grand Rounds<br />
(designated Tues, 12:30-1:30 pm)<br />
6B & 6L<br />
(All students<br />
except TAMC<br />
6B<br />
(All students<br />
except TAMC)<br />
b. PBL Tutorial 6B (1x/week)<br />
6L (1x/week)<br />
c. Bedside Clinical Skills (1-2x/week) 6B & 6L -<br />
d. Chief Medical Resident Rounds (1x/week) 6B & 6L -<br />
e. CVPE (usually Tues pm) 6L 6B<br />
f. EBM 1 and 2 (usually Wed pm) 6L 6B<br />
g. EKG Workshop (usually Tues pm) 6L 6B<br />
h. HIPSTER (Sim Session) 6B & 6L -<br />
6B (1x/week)<br />
6L (1x/month)<br />
i. HIV <strong>Medicine</strong> (Tues 1:30-5:00 pm) 6L 6B<br />
j. Neuro 1 and 2 (usually Tues pm) 6L 6B<br />
k. Site-specific conferences 6B & 6L 6B & 6L<br />
4. Learning Objectives<br />
a. Training Problems (33) 6B & 6L 6B & 6L<br />
b. General Clinical Core Competencies in IM (17) 6B & 6L 6B & 6L<br />
5. Evaluation<br />
a. Observed History and Physical (with BPES)<br />
6B & 6L -<br />
(by end <strong>of</strong> 2 nd wk <strong>of</strong> inpatient)<br />
b. Observed Patient Counseling (2) 6B & 6L<br />
c. Mid-Clerkship Feedback Form 6B & 6L 6B & 6L<br />
d. Student Evaluation Forms 6B & 6L 6B & 6L<br />
e. Clinical Skills Exam (Saturday, ____________ ) End <strong>of</strong> Clerkship<br />
f. NBME Exam (Friday, ____________________) End <strong>of</strong> Clerkship<br />
4
TOP 10 WAYS TO EXCEL ON THE INTERNAL MEDICINE CLERKSHIP<br />
1. Find out what your residents and preceptors expect <strong>of</strong> you. Meet and try to exceed their<br />
expectations. Follow through on every assigned task.<br />
2. Be actively involved in the care <strong>of</strong> your patients to the greatest extent possible. Go the<br />
extra mile for your patients. You will benefit as much as they will.<br />
3. Go the extra mile for your team. Additional learning will follow. The more you put in, the<br />
more you will gain.<br />
4. Read consistently and deeply about the problems your patients face. Raise what you<br />
learn in your discussions with your team and in your notes. Educate your team members<br />
about what you learn whenever possible.<br />
5. Learn to do excellent presentations as early as possible. This will make you more effective<br />
in patient care and gain the confidence <strong>of</strong> your supervisors to allow you more involvement<br />
in patient care.<br />
6. Ask good questions.<br />
7. Speak up—share your thoughts in teaching sessions, share your opinions about your<br />
patients’ care, constructively discuss how to improve the education you are receiving and<br />
the systems around you.<br />
8. Actively seek feedback and reflect on your experiences.<br />
9. Keep your goals focused on the right priorities, in the following order: patient care,<br />
learning, and personal satisfaction. You should always strive to meet all three goals.<br />
10. Always be enthusiastic. Be caring and conscientious and strive to deliver outstanding<br />
quality to your patients as you learn as much as you can from every experience.<br />
From: Primer to the Internal <strong>Medicine</strong> Clerkship, Second Edition, A Guide Produced by the<br />
Clerkship Directors in Internal <strong>Medicine</strong> (CDIM), c2008, 2nd edition<br />
Download free <strong>of</strong> charge from:<br />
http://www.im.org/Publications/PhysiciansInTraining/Pages/Primer.aspx<br />
5
DESCRIPTION OF THE THIRD-YEAR CLERKSHIP IN INTERNAL MEDICINE<br />
INTRODUCTION<br />
Goal <strong>of</strong> the Clerkship<br />
The goal <strong>of</strong> the Third-Year Clerkship in Internal <strong>Medicine</strong> is to provide the opportunity to develop<br />
experience and competence in Internal <strong>Medicine</strong>, which serves as the foundation for all<br />
specialties and their respective residencies. To practice competently, a physician must obtain and<br />
retain a large body <strong>of</strong> knowledge, master the skills <strong>of</strong> clinical practice, develop efficient problem<br />
solving techniques and demonstrate compassion, integrity, self-discipline and life-long learning<br />
skills. It is the student’s responsibility to utilize this <strong>clerkship</strong> experience to accomplish these<br />
goals. It is the <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong>’s responsibility to assure that every graduate <strong>of</strong> the John<br />
A. Burns School <strong>of</strong> <strong>Medicine</strong> has obtained graduation level competency in Internal <strong>Medicine</strong>.<br />
The core <strong>of</strong> this <strong>clerkship</strong> is “Patient-Based Learning,” which occurs as students evaluate patients<br />
through history taking and physical examinations, develop comprehensive assessments including<br />
appropriate differential diagnoses, formulate diagnostic, therapeutic and education plans and then<br />
provide care and follow-up appropriate to the inpatient or ambulatory setting.<br />
Design <strong>of</strong> the Clerkship<br />
Third-Year Clerkship in Internal <strong>Medicine</strong> (MED 531/532)<br />
MED 531 for 6B students is 11 weeks in length and consists <strong>of</strong> 5-1/2 or 6 weeks <strong>of</strong> Inpatient<br />
<strong>Medicine</strong> and 5-1/2 or 5 weeks <strong>of</strong> Ambulatory <strong>Medicine</strong>. MED 532 for 6L students consists <strong>of</strong> 6<br />
weeks <strong>of</strong> Inpatient <strong>Medicine</strong> (block) and 25 half days <strong>of</strong> ambulatory medicine (clinics - one half<br />
day weekly for 21-22 weeks plus 3-4 additional half days).<br />
Work Hours, Designated Study Time, Days Off and Holidays<br />
Work hours<br />
No student should work more than eighty (80) hours per week, averaged over the course <strong>of</strong> the<br />
<strong>clerkship</strong>.<br />
The <strong>clerkship</strong> recognizes that excessive work hours do not promote student well-being and may<br />
endanger students, their patients and others with whom they interact.<br />
For inpatient medicine, the earliest time that any student is permitted to arrive at the hospital is<br />
4:00 a.m. and the earliest time that any student is permitted to see any patient, that is, to actually<br />
talk to and examine, is 4:30 a.m. (excluding emergency situations such as Code Blues). (See<br />
Inpatient <strong>Medicine</strong>)<br />
The Hospital Site Coordinators and Chief Medical Residents are aware <strong>of</strong> these work hour<br />
guidelines.<br />
If a student is not able to complete his/her work within these work hour guidelines, the student is<br />
advised to see his/her Hospital Site Coordinator, Chief Medical Resident or Supervising Resident.<br />
6
If a student does not follow these guidelines, the Hospital Site Coordinator and Chief Medical<br />
Resident are required to advise the student and notify the <strong>clerkship</strong>.<br />
It is the <strong>clerkship</strong>'s goal that students will become more efficient with experience, that they will be<br />
able to arrive at the hospital and see patients at reasonable times and that they will be able to<br />
maintain reasonable work hours.<br />
"Designated study time"<br />
Students should have one (1) afternoon <strong>of</strong> "designated study time" per week, averaged over<br />
the course <strong>of</strong> the <strong>clerkship</strong>.<br />
"Designated study time" is defined as time Monday through Friday and morning through<br />
afternoon away from patient care responsibilities that is devoted to studying which includes<br />
reading, completing write-ups, preparing for required <strong>clerkship</strong> activities such as PBL Tutorials,<br />
Bedside Clinical Skills rounds, Chief Rounds and other inpatient or ambulatory activities.<br />
Students will have "designated study time" when their patient care responsibilities and any<br />
required activities are finished. (See Summary Table <strong>of</strong> Required <strong>Medicine</strong> Clerkship Activities)<br />
In both the inpatient and ambulatory settings, students are advised to notify their team and<br />
preceptor(s), respectively, when they are leaving to study.<br />
"Designated study time" should be used for educational activities, as described above, and not for<br />
leisure activities. Therefore, academic action may be initiated against students who abuse the<br />
"designated study time," as determined by the <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> Student Education<br />
Committee. Likewise, inpatient and ambulatory sites that do not follow the guidelines on<br />
"designated study time" should be brought to the attention <strong>of</strong> the <strong>clerkship</strong> director.<br />
The one day before the NBME Exam is designated a full day <strong>of</strong> “designated study time” for<br />
<strong>clerkship</strong> students.<br />
Days <strong>of</strong>f<br />
Students must have one (1) day <strong>of</strong>f per week, averaged over the course <strong>of</strong> the <strong>clerkship</strong>.<br />
On Inpatient <strong>Medicine</strong>, there is one (1) day <strong>of</strong>f each week, usually a Saturday or a Sunday. The<br />
day <strong>of</strong>f will be determined by the site’s Hospital Site Coordinator and Chief Medical Resident.<br />
On Ambulatory <strong>Medicine</strong>, there are usually two (2) days <strong>of</strong>f each week, usually Saturday and<br />
Sunday. The days <strong>of</strong>f will be determined by the Ambulatory Preceptor.<br />
Holidays<br />
Students will follow the holiday schedule that is observed at their training site.<br />
Absences<br />
Absences from Inpatient <strong>Medicine</strong><br />
On each day that you are absent, you must notify your Chief Medical Resident and your Hospital<br />
Site Coordinator.<br />
You may be required to make up any time missed. This decision will be made together by your<br />
Chief Medical Resident, Hospital Site Coordinator and Clerkship Director and is dependent on the<br />
reason for absence, length <strong>of</strong> absence, <strong>clerkship</strong> activities missed and your <strong>clerkship</strong><br />
7
performance to date.<br />
Absences from Ambulatory <strong>Medicine</strong><br />
On each half day that you are absent, you must notify your Ambulatory Preceptor and the Clerkship<br />
Director (Dr. Laurie Tam at lmtam@hawaii.edu).<br />
Each half day missed must be made up.<br />
6B students usually have 2-4 weekday afternoons and every Saturday <strong>of</strong>f each week. They<br />
should try to schedule their make up during these times, at the convenience <strong>of</strong> their Ambulatory<br />
Preceptor.<br />
6L ambulatory students usually have 3 half days and every Saturday <strong>of</strong>f each week. They should<br />
try to schedule their make up during these times, at the convenience <strong>of</strong> their Ambulatory<br />
Preceptor.<br />
Notes<br />
Attendance is mandatory for all <strong>Medicine</strong> Clerkship orientations and exams.<br />
If you are absent for more than three (3) days, totaled over the course <strong>of</strong> the <strong>clerkship</strong>, the<br />
<strong>clerkship</strong> is required to report this to the Office <strong>of</strong> Student Affairs.<br />
Required make up for time missed must be completed by the end <strong>of</strong> <strong>Medicine</strong> Clerkship in order<br />
to receive Credit for the <strong>clerkship</strong>. Ideally, required make up should be completed in the same<br />
half <strong>of</strong> the <strong>clerkship</strong> that time was missed.<br />
Questions regarding absences should be directed to the Clerkship Director (Dr. Laurie Tam at<br />
lmtam@hawaii.edu).<br />
CURRICULUM<br />
The <strong>Medicine</strong> Clerkship Curriculum is based on the Clerkship Directors in Internal <strong>Medicine</strong><br />
(CDIM)-Society <strong>of</strong> General Internal <strong>Medicine</strong> (SGIM) Core <strong>Medicine</strong> Clerkship Curriculum<br />
Guide Version 3.0, which was released in 2006 to all <strong>Medicine</strong> <strong>clerkship</strong> directors in the United<br />
States. The third edition outlines thirty-three (33) Training Problems and seventeen (17)<br />
General Clinical Core Competencies, which are aligned with the Accreditation Council for<br />
Graduate Medical Education (ACGME) general competencies. The Training Problems and<br />
General Clinical Core Competencies are printed in the <strong>clerkship</strong>’s Student Handbook and<br />
website.<br />
The <strong>Medicine</strong> Clerkship Curriculum, which has been reviewed by JABSOM’s <strong>Department</strong><br />
<strong>of</strong> <strong>Medicine</strong> Student Education Committee (SEC), is aligned with and fulfills JABSOM’s<br />
Graduation Objectives. The curriculum provides third-year medical students with the<br />
opportunity to develop and demonstrate competence and excellence in the medical<br />
knowledge, clinical skills and pr<strong>of</strong>essionalism expected in the evaluation and care <strong>of</strong> the<br />
adult patient.<br />
8
Learning Objectives<br />
a. Training Problems (See Appendix A)<br />
Appendix B)<br />
b. General Clinical Core Competencies in Internal <strong>Medicine</strong> (See<br />
Learning Strategies<br />
a. After seeing each patient, students should identify which Training<br />
Problems were manifested, read and study those Training Problems and assess whether<br />
they are able to meet the specific learning objectives for each (Appendix A).<br />
b. Students should read and study the General Clinical Core<br />
Competencies in Internal <strong>Medicine</strong> and assess whether they are able to meet the<br />
specific learning objectives for each (Appendix B).<br />
c. Students should refer to the Recommended Resources for their<br />
reading and studying. .<br />
EVALUATION IN THE THIRD-YEAR CLERKSHIP IN INTERNAL MEDICINE<br />
General Guidelines<br />
The <strong>clerkship</strong> uses a "competency-based" system to assess the three domains <strong>of</strong> Medical Knowledge,<br />
Skills and Pr<strong>of</strong>essionalism.<br />
For Medical Knowledge, competency is assessed throughout the <strong>clerkship</strong> by faculty and resident<br />
observations <strong>of</strong> students’ clinical performance. It is also assessed by performance on the NBME<br />
Subject Examination in Internal <strong>Medicine</strong> administered at the end <strong>of</strong> the <strong>clerkship</strong><br />
For Clinical Skills, competency is assessed throughout the <strong>clerkship</strong> by faculty and resident<br />
observations <strong>of</strong> students’ clinical performance. It is also assessed by performance on the Clinical<br />
Skills Exam (CSE) conducted by the Center for Clinical Skills near the end <strong>of</strong> the <strong>clerkship</strong>.<br />
For Pr<strong>of</strong>essionalism, competency is assessed throughout the <strong>clerkship</strong> by faculty and resident<br />
observations <strong>of</strong> students’ clinical performance.<br />
a. Hospital Site Coordinators and Ambulatory Preceptors give students mid-<strong>clerkship</strong> feedback on<br />
the students’ clinical performance, reviewing the students’ strengths and weaknesses and<br />
discussing specific strategies to improve. Therefore the <strong>clerkship</strong> expects students to<br />
demonstrate improvement in their clinical performance by the end <strong>of</strong> the <strong>clerkship</strong>.<br />
b. The UH <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> Student Education Committee reviews each student’s entire<br />
<strong>clerkship</strong> performance, including Clinical Performance (inpatient and ambulatory), CSE and<br />
NBME Exam to determine each student’s grade.<br />
c. The <strong>clerkship</strong> does not use numerical formulas for evaluation and grading.<br />
d. For questions about <strong>clerkship</strong> grades, refer to JABSOM’s Academic Appeals Policy.<br />
9
Credit<br />
a. To earn Credit for the Third-Year Clerkship in Internal <strong>Medicine</strong> (MED 531 for 6B students;<br />
MED 532 for 6L students), students must demonstrate Clerkship Level Competency in all three<br />
domains, as reflected by their Clinical Performance (inpatient and ambulatory), CSE and NBME<br />
Exam.<br />
For Clinical Performance (inpatient and ambulatory rotations), students need to receive ratings <strong>of</strong><br />
Competent or higher.<br />
On the CSE, students need to score 55 or higher.<br />
On the NBME Exam, students need to score 60 or higher.<br />
Students who do not demonstrate Clerkship Level Competency in all three domains by the end <strong>of</strong><br />
the <strong>clerkship</strong> may be required to repeat part or all <strong>of</strong> the <strong>clerkship</strong> and/or retake the CSE and/or<br />
NBME Exam.<br />
b. To earn Credit for Advanced <strong>Medicine</strong> (MED 541), which is a JABSOM graduation requirement,<br />
students must also demonstrate Graduation Level Competency on their CSE and NBME Exam<br />
by December 31 <strong>of</strong> the fourth year.<br />
On the CSE, students need to score 60 or higher.<br />
On the NBME Exam, students need to score 67 or higher.<br />
Students who do not demonstrate Graduation Level Competency on their CSE and/or NBME<br />
Exam by the end <strong>of</strong> the <strong>clerkship</strong> will be required to retake the respective exam. They may also<br />
be required to complete a designated fourth-year <strong>Medicine</strong> elective before retaking the exam.<br />
Retaking Exams<br />
CSE<br />
Students who score 55-59 on their CSE must retake the CSE and score 60 (Graduation Level<br />
Competency) or higher by December 31 <strong>of</strong> their fourth year. Students will have up to two (2)<br />
opportunities to achieve this.<br />
NBME Exam<br />
Students who score 60 - 66 on their NBME Exam must retake the NBME Exam and score 67<br />
(Graduation Level Competency) or higher by December 31 <strong>of</strong> their fourth year. Students will have up<br />
to two (2) opportunities to achieve this.<br />
Honors<br />
The <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> gives all students the opportunity to earn an "Honors" grade for exceptional<br />
performance in the Third-Year Clerkship in Internal <strong>Medicine</strong>.<br />
To earn Honors for the Third-Year Clerkship in Internal <strong>Medicine</strong> (MED 531 for 6B students; MED<br />
532 for 6L students), students must demonstrate mostly Exceptional performance in all three domains,<br />
as reflected by their Clinical Performance (inpatient and ambulatory), CSE and NBME Exam by the end<br />
<strong>of</strong> the <strong>clerkship</strong>.<br />
10
SUMMARY OF EVALUATION<br />
1. Medical Knowledge:<br />
o Clinical performance (Student Evaluation Form)<br />
(Interns, Residents, Chief Resident, Inpatient and Ambulatory Attendings)<br />
Credit for Credit for<br />
Clerkship Advanced <strong>Medicine</strong><br />
Competency (in 3 rd yr) (by 12/31 <strong>of</strong> 4 th yr) Consequence<br />
- - - Repeat the <strong>clerkship</strong>,<br />
partially or entirely<br />
Clerkship Level + +<br />
o NBME Subject Exam in Internal <strong>Medicine</strong> (Shelf Exam)<br />
Credit for Credit for<br />
NBME Clerkship Advanced <strong>Medicine</strong><br />
Score Competency (in 3 rd yr) (by 12/31 <strong>of</strong> 4 th yr) Consequence<br />
3. Pr<strong>of</strong>essionalism:<br />
o Clinical performance (reflected on Student Evaluation Form)<br />
(Interns, Residents, Chief Resident, Inpatient and Ambulatory Attending)<br />
Credit for Credit for<br />
Clerkship Advanced <strong>Medicine</strong><br />
Competency (in 3 rd yr) (by 12/31 <strong>of</strong> 4 th yr) Consequence<br />
- - - Repeat the <strong>clerkship</strong>,<br />
partially or entirely<br />
Clerkship Level + +<br />
SPECIFIC REQUIREMENTS AND GUIDELINES<br />
Inpatient <strong>Medicine</strong><br />
Schedule:<br />
1) For 6B students, Inpatient <strong>Medicine</strong> is 5-1/2 weeks (if in the first half <strong>of</strong> the academic year) or 6<br />
weeks (if in the second half <strong>of</strong> the academic year).<br />
2) For 6L students, Inpatient <strong>Medicine</strong> is 6 weeks.<br />
Site: The student will be assigned to Kuakini Medical Center (KMC), Queen’s Medical Center<br />
(QMC) or Tripler Army Medical Center (TAMC).<br />
Orientation: The student will be oriented to the site by its Hospital Site Coordinator(s) (HSC) and<br />
Chief Medical Resident (CMR).<br />
Team Assignment: The student will be assigned to a medical team where an Upper Level<br />
Resident will be directly responsible for the student’s supervision. The student will also work with<br />
the Intern(s) on the team.<br />
Call:<br />
1) Students must take call every day that their team is on call. Students may leave earlier if<br />
their patient care responsibilities are complete, with the Upper Level Resident’s approval.<br />
2) Students at KMC must take one (1) overnight call with their team, preferably a Friday night<br />
or a Saturday night.<br />
Work Hours (See Work Hours, Dedicated Study Time and Days Off):<br />
1) The earliest time that students are permitted to arrive at the hospital is 4:00 a.m. at KMC<br />
and 5:00 a.m. at QMC and TAMC.<br />
2) The earliest time that students are permitted to see patients, that is, to actually talk to and<br />
examine patients, is 4:30 a.m. at KMC and 5:30 a.m. at QMC and TAMC (excluding emergency<br />
situations such as Code Blues).<br />
3) The Hospital Site Coordinators, Chief Medical Residents and Upper Level Residents are<br />
aware <strong>of</strong> these work hour guidelines. If a student is not able to complete his/her work within<br />
these work hour guidelines, the student is advised to see his/her Hospital Site Coordinator, Chief<br />
12
Medical Resident or Upper Level Resident. If a student does not follow these work hour<br />
guidelines, the Hospital Site Coordinator, Chief Medical Resident or Upper Level Resident are<br />
required to advise the student and notify the <strong>clerkship</strong>.<br />
Patient Assignment:<br />
1) The Upper Level Resident will be responsible for assigning patients to the student.<br />
Patients should be selected for their ability to cooperate and communicate, as well as for their<br />
specific medical problems.<br />
2) The student has a list <strong>of</strong> Training Problems on which the Third-Year Clerkship in Internal<br />
<strong>Medicine</strong> curriculum and specific learning objectives are based. The student’s goal is to see at<br />
least one (1) inpatient patient with each <strong>of</strong> thirty-two (32) Training Problems. Note that the Training<br />
Problem does not have to be the patient’s Chief Complaint. In fact, a patient may present with many<br />
Training Problems. (See Training Problems section)<br />
Patient Census: The student should admit 1 – 2 patients per call. The student should actively<br />
follow an average <strong>of</strong> two (2) patients at all times (maximum 5 patients).<br />
Patient Care Responsibilities:<br />
1) The student should complete an Initial History and Physical on each and every patient<br />
assigned to the student, whether or not the student was present for the patient’s admission (i.e.<br />
transfer patients, etc). This Initial History and Physical includes interviewing and examining<br />
patients either independently or while being observed by a resident or attending. If the student<br />
observes a resident or attending obtain the History and Physical, this observation does not qualify as<br />
the student’s own History and Physical. The student would have to go back at another time and<br />
perform his/her own independent History and Physical “Group” work-ups are not allowed or<br />
accepted.<br />
2) The student should perform the physical exam which was taught as the Basic Physical<br />
Exam Sequence (BPES) in the pre-clinical years. Note that the funduscopic exam is included in the<br />
BPES. The student will also be expected to perform appropriate Branch Steps as needed. The<br />
Upper Level Resident is responsible for insuring proper supervision <strong>of</strong> the following parts <strong>of</strong> the<br />
physical exam which may be performed by the student if clinically indicated: female breast exam,<br />
female genital and/or pelvic exam, male genital and/or prostate exam, and female and male<br />
rectal exam. This means that the student must be supervised by a physician (interns, upper level<br />
residents, chief residents or attendings) who is certified or has expertise to competently perform the<br />
exam in question.<br />
4) The student is expected to Pre-Round and write daily Progress Notes on all his/her<br />
assigned patients before the Intern or Upper Level Resident(s) write their note(s). The Intern or<br />
Upper Level Resident should review the notes with the student, give constructive feedback and<br />
countersign the notes. Any missed history or physical exam finding should be noted, corrected and<br />
demonstrated as needed.<br />
5) The student should Round with the team. Since the student will be expected to have<br />
detailed knowledge <strong>of</strong> his/her assigned patients, the student is expected to take the lead in<br />
discussing his/her patients, including the student’s assessment <strong>of</strong> the patients’ problems and<br />
the student’s plans. In addition, the student will be expected to have a general knowledge <strong>of</strong> the<br />
other patients on the team so that he/she can be included in the team’s discussions <strong>of</strong> the care <strong>of</strong><br />
13
all <strong>of</strong> the team’s patients and can assist the team in the care <strong>of</strong> all <strong>of</strong> the team’s patients. The<br />
student will be expected to actively participate in teaching attending rounds with the team.<br />
6) The student is expected to assume as much patient care responsibility and functions<br />
as the team feels are appropriate for the individual student’s level <strong>of</strong> training and competence.<br />
The student is expected to participate in patient education and counseling, work with nursing<br />
staff, dieticians, respiratory therapists, physical and occupational therapists, social workers,<br />
hospital chaplains, etc. and to assist in discharge planning.<br />
7) The student may perform Procedures or assist in the performance <strong>of</strong> procedures that the<br />
team feels are appropriate for the student’s level <strong>of</strong> training and competence. The Upper Level<br />
Resident is responsible for insuring proper supervision <strong>of</strong> any procedure performed or assisted by<br />
the student. This means that the student must be supervised by a physician who is certified or has<br />
expertise to competently perform the procedure in question, which includes interns, upper level<br />
residents, chief residents or attendings. Note that there are no required procedures for third-year<br />
medical students to perform.<br />
8) The student should learn how to write Orders on his/her assigned patients. The student will<br />
observe the residents enter orders electronically. The student should practice writing orders in their<br />
Comprehensive Write-ups and daily Progress Notes (in the Plans section) and on the Physician's<br />
Orders forms (See Physician’s Orders). The Hospital Site Coordinator and residents should<br />
review the student’s orders with the student and correct them as needed.<br />
Comprehensive Write-ups:<br />
1) The student is required to submit 3 write-ups by halfway through the inpatient rotation<br />
(averaging 1 write-up each week - schedule to be determined by the Hospital Site Coordinator).<br />
The HSC will decide whether these 3 write-ups are satisfactory. If they are deemed satisfactory,<br />
then the student will not be required to submit any more write-ups. If, however, they are deemed<br />
unsatisfactory, then the student will be required to submit 1 – 3 additional write-ups, as<br />
determined by the Hospital Site Coordinator, up to a maximum <strong>of</strong> 6 write-ups. (See Appendix)<br />
2) The HSC should read and then review each comprehensive write-up with the student and<br />
give constructive feedback.<br />
3) At the end <strong>of</strong> Inpatient <strong>Medicine</strong>, the student will turn in a total <strong>of</strong> 3 - 6 comprehensive<br />
write-ups, (total number to be determined by the HSC), either the originals or copies <strong>of</strong> the originals<br />
with the HSC’s comments, to the <strong>clerkship</strong> <strong>of</strong>fice.<br />
Required Clerkship Activities specific to Inpatient <strong>Medicine</strong>:<br />
1) Bedside Clinical Skills<br />
week.<br />
a) All students on Inpatient <strong>Medicine</strong> will attend Bedside Clinical Skills 1 - 2 times each<br />
b) Each week, one student will prepare and formally present one <strong>of</strong> his/her patients.<br />
c) Patients should be chosen who are unknown to the other students in the group (ideally)<br />
and who have physical exam findings.<br />
d) The student who is presenting should have the case presentation memorized<br />
(written notes for referral only).<br />
14
e) After presenting the case, the student will take the group to see the patient. (The<br />
student should have already gotten the patient’s consent and determined that the patient would<br />
be available for bedside teaching.)<br />
f) The Bedside Clinical Skills attending will teach/review physical exam skills and<br />
review/clarify important physical exam findings.<br />
g) The Bedside Clinical Skills attending may meet individually with the student who<br />
presented to give constructive feedback on his/her case presentation. (See Case Presentation<br />
Evaluation Form)<br />
h) The Bedside Clinical Skills attending may use the Small Group Learning Experience<br />
Evaluation Form to evaluate the students in the group. (See Small Group Learning<br />
Experience Evaluation Form)<br />
2) Chief Medical Resident Rounds<br />
a) All students on Inpatient <strong>Medicine</strong> will attend weekly Chiefs Rounds with the Chief<br />
Medical Resident (CMR). These may include bedside or didactic teaching.<br />
b) Chief Rounds give the students the opportunity to specify which areas in Internal<br />
<strong>Medicine</strong> they would like the CMR to teach in a small group setting.<br />
c) The CMR, together with the Upper Level Resident, are responsible for insuring that<br />
students are instructed in, but not limited to, the following:<br />
o Case presentations<br />
o Interpretation <strong>of</strong> basic EKGs<br />
o Interpretation <strong>of</strong> common imaging, including chest and abdominal x-rays and<br />
CT, head CT and MRI<br />
o Physiology and management <strong>of</strong> fluids and electrolytes<br />
o Interpretation <strong>of</strong> arterial blood gases<br />
o Basic physiology and management <strong>of</strong> shock<br />
o Basic understanding and management <strong>of</strong> ventilators (at KMC)<br />
d) The CMR may use the Small Group Learning Experience valuation Form to evaluate<br />
the students in the group. (See Small Group Learning Experience Evaluation Form)<br />
3) HIPSTER (<strong>Hawaii</strong> InterPr<strong>of</strong>essional Simulation Training for Emergency<br />
Response)<br />
Evaluation and Feedback to Students:<br />
1) The student is expected to regularly (at least once a week) ask for feedback on his/her<br />
performance and progress from his/her residents and attendings. It is especially important that<br />
this occurs before the student rotates <strong>of</strong>f the team and before the residents and attendings rotate<br />
<strong>of</strong>f the team. This feedback should identify the student’s strengths and weaknesses so that the<br />
student will know what to work on improving.<br />
2) Midway through Inpatient <strong>Medicine</strong>, the Hospital Site Coordinator will complete a Mid-<br />
Clerkship Feedback Form and discuss it with the student. The HSC will indicate whether the<br />
student’s progress to date is satisfactory or unsatisfactory, identify the student’s strengths and<br />
weakness and suggest a remediation plan if necessary. (See Mid-Clerkship Feedback Form)<br />
15
3) Interns, Upper Level Residents and Attendings who work with the student for one (1) week<br />
or more are expected to evaluate the student. During the course <strong>of</strong> the student’s inpatient rotation,<br />
the Intern and Upper Level Resident are expected to give the student verbal feedback on his/her<br />
performance and progress. This feedback should be provided on a regular basis, ideally daily but at<br />
least weekly. Then during the last week <strong>of</strong> the Intern and Upper Level Resident’s block or during the<br />
last week <strong>of</strong> the student’s inpatient rotation, the Intern and the Upper Level Resident will complete<br />
independent evaluations <strong>of</strong> the student which will be turned in to the Chief Medical Resident or<br />
Hospital Site Coordinator. Finally, at the end <strong>of</strong> the student’s inpatient rotation, the HSC will<br />
summarize all evaluations and complete a summary Student Evaluation Form for the site, which is<br />
submitted to the <strong>clerkship</strong> <strong>of</strong>fice. (See Student Evaluation Form)<br />
4) The student will be formally observed performing a history and physical on a patient<br />
unknown to the student by the end <strong>of</strong> the student’s second week <strong>of</strong> Inpatient <strong>Medicine</strong>. It is the<br />
student’s responsibility to arrange for a time when both the student and the Chief Medical<br />
Resident are available. It is the CMR’s responsibility to find an appropriate patient. The CMR will<br />
observe the student perform a history and physical. The CMR may also ask the student to make<br />
a brief case presentation. The CMR will complete the Observed History and Physical and<br />
BPES (Basic Physical Exam Sequence) Evaluation Forms (which should be provided by the<br />
student to the CMR) and give the student immediate feedback. If the student’s performance is<br />
not satisfactory, the student must repeat the exercise until his/her performance is satisfactory to<br />
the CMR. Note that this history and physical may be used for one <strong>of</strong> the student’s<br />
comprehensive write-ups. (See Observed History and Physical and BPES Evaluation Forms –<br />
this is a required <strong>clerkship</strong> activity.)<br />
5) The student will have the opportunity to present his/her patients at various hospital rounds<br />
and conferences. The student should ask the Upper Level Resident or Chief Medical Resident in<br />
advance for assistance in preparing for such presentations at a level that is appropriate for the<br />
student’s training and for the particular rounds or conference. After the presentation, the student<br />
should ask the physician who is supervising the rounds or conference for feedback. (See Case<br />
Presentation Evaluation Form)<br />
Ambulatory <strong>Medicine</strong><br />
Schedule: For 6B students, Ambulatory <strong>Medicine</strong> consists <strong>of</strong> 5 half days per week for 5-1/2<br />
weeks (if in the first half <strong>of</strong> the academic year) or for 5 weeks (if in the second half <strong>of</strong> the<br />
academic year). For 6L students, Ambulatory <strong>Medicine</strong> consists <strong>of</strong> 25 half days (one half day<br />
weekly for 21-22 weeks plus 3-4 additional half days).<br />
Location: The Ambulatory <strong>Medicine</strong> sites include Queen Emma Clinics, TAMC Internal<br />
<strong>Medicine</strong> Clinic, VA Clinics, community health clinics, Kaiser HMO and private physician<br />
<strong>of</strong>fices. The sites for MED 531 for 6B students are all on Oahu, primarily in Honolulu,<br />
while the sites for MED 532 for 6L students are either outside <strong>of</strong> Honolulu on Oahu or on<br />
the Neighbor Islands. Although each site has unique features, the <strong>clerkship</strong>’s goal is to<br />
provide students with a uniform learning experience based on the same learning objectives<br />
while allowing students the opportunity to take advantage <strong>of</strong> the strengths <strong>of</strong> each site.<br />
Due to the distant location <strong>of</strong> their assigned sites and their schedules, 6L students<br />
do not attend any <strong>clerkship</strong> activities while on Ambulatory <strong>Medicine</strong> (UH <strong>Department</strong> <strong>of</strong><br />
<strong>Medicine</strong> Grand Rounds, EBM 1 and 2, EKG Workshop, HIV <strong>Medicine</strong>, Neuro 1 and 2).<br />
16
Patient Assignment: The Ambulatory Preceptor(s) will be responsible for assigning patients<br />
to the student. Patients should be selected for their ability to cooperate and communicate, as<br />
well as for their specific medical problems. The student has a list <strong>of</strong> Training Problems on<br />
which the Third-Year Clerkship in Internal <strong>Medicine</strong> curriculum and specific learning<br />
objectives are based. The student’s goal is to see at least one (1) ambulatory patient with<br />
each <strong>of</strong> thirty-three (33) Training Problems. Note that the Training Problem does not have to<br />
be the patient’s Chief Complaint. In fact, a patient may present with many Training Problems.<br />
(See Training Problems section)<br />
Patient Census: The student should work up at least two (2) patients each half day.<br />
Patient Care Responsibilities:<br />
1) The student may see new or returning patients for complete examinations or<br />
problem-focused visits. Ideally, the student will see some <strong>of</strong> the patients when they return<br />
for their follow-up visits.<br />
2) After reviewing the patient’s chart as necessary, the student will perform an<br />
appropriate history and physical examination. The student will present the case to the<br />
preceptor who should correct and demonstrate any missed history or physical exam<br />
findings and review the student’s assessment and plans.<br />
3) The student will write an appropriate write-up or progress note in a timely manner, as<br />
specified by the preceptor. The preceptor should review the write-up or note with the student and<br />
give constructive feedback.<br />
4) The student is expected to carry out whatever patient care responsibilities and functions<br />
the preceptor feels is appropriate for the student’s level <strong>of</strong> training and competence. The student<br />
should try to assume as much responsibility as is appropriate and possible. The student is<br />
expected to participate in patient education and counseling, work with <strong>of</strong>fice/clinic staff, and to<br />
assist in follow-up planning. If the student’s patient requires any consultations or procedures, the<br />
student is highly encouraged to be present if the patient agrees. If the student’s patient is<br />
hospitalized, the student is highly encouraged to follow the patient during the hospitalization.<br />
Comprehensive Write-ups:<br />
1) The 6B student is required to complete an average <strong>of</strong> two (2) comprehensive writeups<br />
each week. The 6L student is required to complete an average <strong>of</strong> two (2)<br />
comprehensive write-ups each month. These comprehensive write-ups may be different<br />
from those initially written – they are expected to be more detailed and thorough, requiring<br />
additional reading and thought. (See Appendix D and E)<br />
2) The Ambulatory Preceptor should read, correct and review each comprehensive writeup<br />
with the student and give constructive feedback.<br />
3) At the end <strong>of</strong> Ambulatory <strong>Medicine</strong>, the student will turn in a total <strong>of</strong> ten (10)<br />
comprehensive write-ups, either the originals or copies <strong>of</strong> the originals with the preceptor’s<br />
comments, to the <strong>clerkship</strong> <strong>of</strong>fice.<br />
Evaluation and Feedback to Students:<br />
1) The student is expected to regularly ask the Ambulatory Preceptor for feedback on<br />
his/her performance and progress, ideally on a weekly basis for 6B students and on a<br />
monthly basis for 6L students, and definitely before the student finishes Ambulatory<br />
<strong>Medicine</strong>. This feedback will give the student the opportunity to correct mistakes and<br />
17
omissions and to improve skills.<br />
2) Midway through Ambulatory <strong>Medicine</strong>, the student should provide the Ambulatory<br />
Preceptor with a Mid-Clerkship Feedback Form to complete and discuss with the<br />
student. The preceptor will indicate whether the student’s progress to date is satisfactory<br />
or unsatisfactory, identify the student’s strengths and weakness and suggest a remediation<br />
plan if necessary. (See Mid-Clerkship Feedback Form)<br />
3) At the end <strong>of</strong> Ambulatory <strong>Medicine</strong>, the Ambulatory Preceptor will complete a Student<br />
Evaluation Form provided by the Third-Year Clerkship in internal <strong>Medicine</strong>. The Student<br />
Evaluation Form should be completed during the last week <strong>of</strong> the student’s Ambulatory<br />
<strong>Medicine</strong>. The preceptor should review the Student Evaluation Form with the student and the<br />
student should then sign the form. The form is then submitted to the <strong>clerkship</strong> <strong>of</strong>fice. (See<br />
Student Evaluation Form)<br />
4) The student will be formally observed counseling a patient and/or family on two<br />
separate occasions. (See Observed Patient Counseling Evaluation Form – this is a<br />
required <strong>clerkship</strong> activity.)<br />
PBL Tutorial<br />
1) All students will attend PBL Tutorial:<br />
a. Inpatient students, whether 6B or 6L, will attend weekly PBL Tutorial led by<br />
their Hospital Site Coordinator who serves as the Inpatient PBL Tutor.<br />
b. Ambulatory 6B students will attend weekly PBL Tutorial led by an Ambulatory<br />
PBL Tutor.<br />
c. Ambulatory 6L students will attend monthly PBL Tutorial led by an<br />
Ambulatory PBL Tutor.<br />
2) One student will prepare and formally present one <strong>of</strong> his/her patients at each PBL<br />
Tutorial.<br />
3) Patients should ideally be chosen who are unknown to the other students in the<br />
tutorial group and who manifest one or more Training Problems (see Appendix A).<br />
4) The student who is presenting should have the case presentation memorized<br />
(written notes for referral only) and should bring and be familiar with all<br />
pertinent data (labs, pathology reports, EKG, imaging, etc.).<br />
6) The group will agree on appropriate Learning Issues that ideally address Training<br />
Problems and their specific Learning Objectives. (See Appendix A)<br />
7) At the following week’s PBL Tutorial, the Learning Issues from the previous week will<br />
be presented and discussed.<br />
8) The PBL Tutor should meet individually with the student who presented to give<br />
constructive feedback on the student’s case presentation. (See Case Presentation<br />
Evaluation Form)<br />
9) The PBL Tutor may use the Small Group Learning Experience Evaluation Form to<br />
evaluate the students in the group. (See Small Group Learning Experience<br />
Evaluation Form)<br />
18
Role Descriptions for <strong>Medicine</strong> 531/532<br />
The Bedside Clinical Skills Attending’s Role<br />
1. The BCS Attending’s role will be to serve as a role model, instructor and facilitator.<br />
The BCS Attending will make formal rounds. Meetings on the inpatient service will<br />
be scheduled regularly and this time should be held inviolable.<br />
2. The BCS Attending will be familiar with and reinforce the method <strong>of</strong> problem based,<br />
self-directed learning, as established in Units 1-5.<br />
3. BCS Attendings will emphasize bedside clinical teaching during their rounds, never<br />
failing to see the patients that are presented. The Attending will serve as resource<br />
faculty at the bedside, teaching techniques and demonstrating abnormalities. In<br />
addition to the general bedside teaching, they are tasked to specifically ensure<br />
competent student performance <strong>of</strong> pulmonary and cardiac bedside examination<br />
skills.<br />
4. The BCS Attending will be responsible for giving feedback to the student on his/her<br />
performance after each presentation. Any problems identified will be discussed and<br />
a plan to (FIX SPACING! remedy difficulties will be constructed. Progress on<br />
previously identified difficulties will also be discussed.<br />
5. BCS Attendings will be responsible for evaluation and will serve on the<br />
<strong>Department</strong>al Student Evaluation Committee.<br />
The Upper Level Resident’s Role<br />
1. Introduction:<br />
The upper level resident (Levels 2 or 3) is ultimately responsible for the third-year medical<br />
student’s experience with the inpatient medical team and should insure that the student has a<br />
good inpatient experience. At the beginning and throughout the student’s inpatient<br />
experience, the resident should clarify what is expected <strong>of</strong> students.<br />
2. Responsibilities:<br />
The Upper Level Resident will be responsible for assigning 2-3 patients per week<br />
for the student work up and continuing care. Patients should be selected for their<br />
ability to cooperate and communicate, as well as for their specific medical problems.<br />
The Upper Level Resident will be responsible also for reviewing the student’s write<br />
ups, for assistance with development <strong>of</strong> learning issues and for help in execution <strong>of</strong><br />
the learning agenda.<br />
The Upper Level Resident will "sign <strong>of</strong>f" on the student’s write up, confirming that<br />
he/she has reviewed the written note and given feedback.<br />
The Upper Level Resident will confirm that the student is pursuing self-directed<br />
learning by taking advantage <strong>of</strong> "Dedicated Learning Time."<br />
19
The Chief Medical Resident’s Role<br />
1. Introduction:<br />
The Chief Medical Resident (CMR) serves as a key faculty resource for the medical<br />
student on the inpatient service. As supervisor for the medical teams and their<br />
students, the CMR helps insure a good experience for the students.<br />
2. Responsibilities:<br />
a. The CMR will supervise and assist the Upper Level Resident in the<br />
inpatient instruction <strong>of</strong> medical students. They are responsible for insuring<br />
that students are instructed in, but not limited to, the following:<br />
o Case presentations<br />
o Interpretation <strong>of</strong> basic EKGs<br />
o Interpretation <strong>of</strong> common imaging, including chest and abdominal x-<br />
rays and CT, head CT and MRI<br />
o Physiology and management <strong>of</strong> fluids and electrolytes<br />
o Interpretation <strong>of</strong> arterial blood gases<br />
o Basic physiology and management <strong>of</strong> shock<br />
o Basic understanding and management <strong>of</strong> ventilators (at KMC)<br />
b. The CMR will observe and evaluate student’s Observed History and<br />
Physical during the student’s first two weeks <strong>of</strong> inpatient medicine, as<br />
previously described.<br />
c. The CMR will lead weekly Chief Rounds with the students as<br />
previously described<br />
d. The CMR will regularly discuss each student’s clinical performance<br />
with the Hospital Site Coordinator.<br />
The Site Coordinator’s Role<br />
1. Introduction:<br />
As a community-based <strong>clerkship</strong>, the Third-Year Clerkship in Internal <strong>Medicine</strong><br />
utilizes several clinical sites for medical student instruction. A major role <strong>of</strong> the<br />
Site Coordinator is to provide students at his/her site with the best possible<br />
educational experience and to insure that that learning experience is equivalent<br />
to the educational experience provided at the other sites utilized by the<br />
<strong>clerkship</strong>.<br />
The Site Coordinator is selected for his/her knowledge and experience at the site and<br />
the ability to work well with physicians, staff and administrators at the site, as well as<br />
the ability to work well with medical students. The Site Coordinator may be inpatient<br />
(Hospital Site Coordinator) or ambulatory (Ambulatory Site Coordinator).<br />
2. Responsibilities <strong>of</strong> Hospital Site Coordinators and Ambulatory Site<br />
Coordinators include, but are not limited to:<br />
a. Selecting qualified faculty to provide a good learning experience for the<br />
20
student(s) assigned to the site. The site coordinator will serve as a resource for<br />
the faculty and chief medical resident (CMR) at the site. This includes orienting<br />
new faculty and CMRs and assisting with faculty development and education<br />
regarding <strong>clerkship</strong> curriculum, expectations and goals.<br />
b. Identifying learning resources at the site that are available for student use (i.e.<br />
library, photocopying, computer, classrooms, etc.).<br />
c. Orientating new students, which include scheduling and leading orientations to<br />
the site and key personnel including faculty, CMR and administrative staff,<br />
making team/clinic assignments, reviewing <strong>clerkship</strong> requirements and student<br />
responsibilities. Orientations should occur on the student’s first day at the<br />
assigned site.<br />
d. Evaluating case presentations. (See Case Presentation Evaluation Form)<br />
e. Evaluating comprehensive write-ups. The Site Coordinator will read students’<br />
comprehensive write-ups and give constructive feedback at least on a weekly<br />
basis. (See Appendix D and E)<br />
f. Meeting with each student regularly to review the student’s performance and<br />
progress and to provide feedback. These meetings should also be used to<br />
review the number and type <strong>of</strong> patients that students are seeing and their level<br />
<strong>of</strong> patient care involvement. (See Training Problems List) Formal meetings<br />
with each student should be scheduled at least twice during the student’s<br />
rotation at the assigned site, once midway and once before the last day (ideally<br />
during the last week).<br />
g. Completing a Mid-Clerkship Feedback Form, midway through the student’s<br />
rotation at the assigned site, indicating whether the student’s progress to date is<br />
satisfactory or unsatisfactory, identifying the student’s strengths and weakness<br />
and suggesting a remediation plan if necessary. The Site Coordinator will<br />
review the completed form with the student to allow the student time to improve<br />
in the identified areas <strong>of</strong> weakness during the remainder <strong>of</strong> the rotation. If the<br />
student’s progress to date is unsatisfactory, the Site Coordinator must<br />
immediately notify the Clerkship Director who may further discuss the student’s<br />
performance and possible remediation with the <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> Student<br />
Education Committee. (See Mid-Clerkship Feedback Form)<br />
h. Coordinating the site evaluation <strong>of</strong> students. The Site Coordinator will<br />
review the student’s performance with each physician (including Interns, Upper<br />
Level Residents and Attendings) who worked with the student for one (1) week<br />
or more and also with any Attendings who worked with the student on a weekly<br />
basis. The Site Coordinator will collect and review evaluation forms such as the<br />
Observed History and Physical, Observed Patient Counseling, Case<br />
Presentations and Small Group Learning Experiences. The Site Coordinator<br />
will complete a summary Student Evaluation Form for the site at the end <strong>of</strong> the<br />
rotation (ideally, during the last week), summarizing all the evaluations including<br />
his/her own personal evaluation. The Site Coordinator will be careful to insure that<br />
a single evaluation, incident or conflict will not overshadow a student’s overall<br />
performance. The Site Coordinator will review the form with the student and<br />
then submit it to the <strong>clerkship</strong> <strong>of</strong>fice. In addition, the Site Coordinator will complete<br />
the confidential Honors/AOA Evaluation Form which is not shared with the student<br />
but is submitted to the <strong>clerkship</strong> <strong>of</strong>fice. If the student’s performance is marginal in<br />
21
any area(s), the Site Coordinator should immediately notify the Clerkship<br />
Director who may further discuss the student’s performance and possible<br />
remediation with the <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> Student Education Committee.<br />
(See Student Evaluation Form and Honors/AOA Evaluation Form)<br />
i. Serving as a member <strong>of</strong> the <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> Student Education<br />
Committee (SEC). The Site Coordinator attends the committee’s monthly<br />
meetings to act as a spokesperson for the students assigned to his/her site,<br />
reporting on students’ performance and progress and recommending<br />
commendation and remediation when appropriate. In addition, SEC members<br />
participate in the oversight, development and implementation <strong>of</strong> all <strong>of</strong> the<br />
<strong>Department</strong> <strong>of</strong> <strong>Medicine</strong>’s 3 rd and 4 th year clinical rotations.<br />
j. Monitoring students’ work hours, dedicated study time, days <strong>of</strong>f and<br />
absences. (See Work Hours, Dedicated Study Time and Days Off section.)<br />
k. Serving as mediator in the event students encounter problems at their<br />
assigned site. Problems may include <strong>clerkship</strong> requirements, <strong>clerkship</strong><br />
performance, absences, mistreatment, harassment and abuse. The Site<br />
Coordinator should refer significant problems to the Clerkship Director and/or the<br />
<strong>Department</strong> <strong>of</strong> <strong>Medicine</strong> Student Education Committee.<br />
3. Additional responsibilities <strong>of</strong> Hospital Site Coordinators include, but are not<br />
limited to:<br />
a. Assisting in Team Assignments - the Hospital Site Coordinator will assist<br />
the Chief Medical Resident with the assignment <strong>of</strong> students to medical<br />
teams.<br />
b. Leading PBL Tutorial. This should occur on average once a week<br />
throughout the <strong>clerkship</strong> and each session should last on average 2 – 3<br />
hours. (See PBL Tutorial description.)<br />
c. Insuring that Bedside Clinical Skills occur 1 – 2 times each week and<br />
Chief Medical Resident Rounds occur 1 time each week and monitoring<br />
students’ attendance at these as well as at other hospital conferences<br />
and rounds deemed to be <strong>of</strong> educational value by the Hospital Site<br />
Coordinator.<br />
The Ambulatory Attending’s Role<br />
1. Introduction:<br />
The ambulatory attending, or preceptor, is a critical element for student learning in<br />
Internal <strong>Medicine</strong> as it is practiced in the ambulatory milieu. Although sometimes<br />
lacking the drama <strong>of</strong> inpatient medicine, the outpatient setting <strong>of</strong>fers special skills sets<br />
in learning and teaching critical thinking, decision making, clinical skills and judgment,<br />
and patient-physician communication in Internal <strong>Medicine</strong><br />
2. Responsibilities:<br />
a) The ambulatory attending/preceptor will serve as a role model for excellence<br />
in ambulatory primary internal medical practice, to include thoughtful, evidence-<br />
22
ased health care that is patient focused, comprehensive, and which maximizes<br />
and restores health, and is preventative.<br />
b) The attending/preceptor will assign patients for student evaluation that will<br />
cover the depth and breadth <strong>of</strong> ambulatory learning issues, as found in the<br />
Learning Objectives listed under Patient’s Presenting Health issues (Appendix<br />
A).<br />
c) The attending/preceptor will monitor and teach data gathering as it applies to<br />
the clinical focus <strong>of</strong> ambulatory patient care; this includes appropriate<br />
consideration <strong>of</strong> the breadth <strong>of</strong> patient health issues, rather than a simple focus<br />
on chief complaint.<br />
d) The attending/preceptor will model and teach evidence-based problem<br />
solving as it applies to the ambulatory experience.<br />
e) The attending/preceptor will critique student write-ups for accuracy, style,<br />
problem solving and give constructive feedback, by applying the criteria <strong>of</strong> the<br />
“comprehensive write-up” and the write-up examples (see Appendix E).<br />
f) The attending/preceptor will give continuous feedback on student clinical and<br />
analytical skills, and stimulate his/her intellectual growth.<br />
g) The ambulatory preceptor will assure completion the “Observation <strong>of</strong> Patient<br />
Counseling form for a least 2 separate patient encounters.<br />
h) The attending/preceptor will evaluate student performance in areas <strong>of</strong><br />
medical knowledge, clinical skills, and pr<strong>of</strong>essionalism and work habits.<br />
23
MISCELLANEOUS CLERKSHIP INFORMATION<br />
24
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
GUIDELINES FOR APPROPRIATE APPEARANCE AND ATTIRE<br />
These guidelines are intended to contribute to your overall pr<strong>of</strong>essional development as students<br />
in training to become physicians. The Third Year Clerkship in Internal <strong>Medicine</strong> expects students<br />
to appear and dress in a pr<strong>of</strong>essional manner. Some things, such as your appearance and attire,<br />
which may have been acceptable in college, may no longer be appropriate in our <strong>clerkship</strong>. Your<br />
appearance and attire should show respect to faculty, staff, classmates, patients and the general<br />
public.<br />
It is recognized that different attire will be necessary for different settings, depending on factors<br />
such as student activities and responsibilities, training sites, patient and public contact. Student<br />
attire should always be appropriate and not interfere with the activities and responsibilities<br />
expected <strong>of</strong> students.<br />
General guidelines for all <strong>Medicine</strong> Clerkship students:<br />
Students should wear:<br />
JABSOM name tag with photo ID<br />
Short white medical coat<br />
Closed-toe footwear<br />
Students should maintain an optimum level <strong>of</strong> personal hygiene and grooming<br />
Strong odors and fragrances should be avoided<br />
Clothes, hair, fingernails and footwear should be clean and neat<br />
Clothing should not be suggestive, revealing or tight-fitting<br />
Clothing should not have <strong>of</strong>fensive images or language<br />
Sites-specific (inpatient and ambulatory) guidelines for <strong>Medicine</strong> Clerkship students:<br />
Students should adhere to the dress code/policy in place at their training site<br />
25
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
RECOMMENDED RESOURCES<br />
Highly recommended <strong>clerkship</strong> guidebook:<br />
Primer to the Internal <strong>Medicine</strong> Clerkship, Second Edition, A Guide Produced by the Clerkship<br />
Directors in Internal <strong>Medicine</strong> (CDIM), c2008, 2nd edition – download free <strong>of</strong> charge from<br />
http://www.im.org/Publications/PhysiciansInTraining/Pages/Primer.aspx<br />
Online resources:<br />
Internal <strong>Medicine</strong> Essentials for Clerkship Students - online materials such as photographs, tables,<br />
screening tools and other instruments – access free <strong>of</strong> charge at http://www.acponline.org/acp_press/essentials/<br />
UpToDate – access available at some training sites<br />
Textbooks:<br />
Internal <strong>Medicine</strong> Essentials for Students, American College <strong>of</strong> Physicians (ACP) and Clerkship Directors<br />
in Internal <strong>Medicine</strong> (CDIM), c2011 – discount <strong>of</strong>fered for ACP student members at<br />
http://www.im.org/Publications/PhysiciansInTraining/Pages/Essentials.aspx<br />
Kochar’s Clinical <strong>Medicine</strong> for Students, Lippincott Williams & Wilkins, c2008, 5 th edition<br />
Cecil Essentials <strong>of</strong> <strong>Medicine</strong>, Elsevier, c2011, 8th edition<br />
Reference textbooks:<br />
DeGowin’s Diagnostic Examination, McGraw-Hill, c2008, 9th edition<br />
Spiral bound books and pocket guides:<br />
Pocket <strong>Medicine</strong>, Lippincott Williams & Wilkins, c2010, 4 th edition<br />
Practical Guide to the Care <strong>of</strong> the Medical Patient, Elsevier, c2011, 8 th edition<br />
Washington Manual <strong>of</strong> Medical Therapeutics, Lippincott Williams & Wilkins, c2010, 33rd edition<br />
Washington Manual <strong>of</strong> Outpatient Internal <strong>Medicine</strong>, Lippincott Williams & Wilkins, c2010, 2nd edition<br />
The Sanford Guide to Antimicrobial Therapy, c2012, 42nd edition<br />
Highly recommended self-assessment program:<br />
MKSAP (Medical Knowledge Self-Assessment Program) for Students 5 (Book and Digital), American<br />
College <strong>of</strong> Physicians (ACP) and Clerkship Directors in Internal <strong>Medicine</strong> (CDIM), c2011 – discount <strong>of</strong>fered for ACP<br />
student members at http://www.im.org/Publications/PhysiciansInTraining/Pages/MKSAPforStudents.aspx<br />
26
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
REQUIRED EQUIPMENT<br />
1. White coat<br />
2. JABSOM nametag<br />
3. Stethoscope<br />
4. Ophthalmoscope and otoscope<br />
5. Penlight<br />
6. Reflex hammer<br />
7. Tuning fork 128 Hz for vibratory exam<br />
8. Tape measure<br />
9. Visual acuity card<br />
10. Small magnifier lens<br />
11. Disposable tongue blades<br />
12. Cotton-tipped swabs for sensory exam<br />
13. Watch with second and minute marks to record vital signs, etc.<br />
All <strong>of</strong> the above listed equipment, except for the JABSOM nametag and watch, are available for<br />
purchase at the Medical Bookstore.<br />
Students are expected to have ALL <strong>of</strong> the equipment and to bring them to their assigned training<br />
sites on the first day. The equipment should be easily and quickly accessible, i.e. worn, carried in<br />
a bag or in/on a white coat.<br />
All students on inpatient medicine are required to carry ALL <strong>of</strong> the listed equipment AT ALL<br />
TIMES while on the wards.<br />
Students on ambulatory medicine may find that their assigned sites may have some, but not all,<br />
<strong>of</strong> the listed equipment available for student use. If the listed equipment are NOT easily and<br />
quickly accessible at the site, it is the student’s responsibility to carry them AT ALL TIMES.<br />
The possible consequences <strong>of</strong> not having the required equipment are (1) being immediately sent<br />
to the medical bookstore to purchase them (requiring the student to make up the missed time)<br />
and (2) receiving unsatisfactory evaluations in the areas <strong>of</strong> (a) Clinical Skills - physical<br />
examinations and (b) Pr<strong>of</strong>essionalism dependability, pr<strong>of</strong>essional appearance and attire.<br />
27
EXPOSURE TO BLOOD/BODY FLUIDS PROTOCOL<br />
1. IMMEDIATELY following the exposure:<br />
a. Flush the exposed skin or mucous membrane with water or saline.<br />
If exposure to the eyes has occurred, use wash station or nearest sink to flush eyes with water for at<br />
least 5 minutes.<br />
b. Wash any needle stick, puncture, cut or abrasion with soap and water.<br />
2. Initiate the host agency protocol for hazardous exposure to blood/body fluids by following the instructions outlined in<br />
the table below.<br />
3. If the exposure is in a non-hospital setting (for example, ambulatory site not associated with a hospital, in a JABSOM<br />
lab, class, or other non-hospital-based exposure), you or your preceptor/supervisor can call Queens ED (547-4311)<br />
to review current protocol for immediate needs in such a circumstance, and begin the process, (AFTER #1). You<br />
may go to an Emergency <strong>Department</strong>, or during open hours, contact the <strong>University</strong> Health Services (Manoa<br />
Campus) 956-8965, and ask for immediate attention.<br />
FACILITY CONTACT or GO TO PHONE<br />
Castle Medical Center Report incident to supervisor. Obtain care from<br />
Employee Health Coordinator or hospital supervisor who<br />
will assist in filing incident report. Contact JABSOM<br />
OSA to report incident.<br />
263-5159 or<br />
hospital supervisor<br />
263-5329<br />
(5 pm-8 am)<br />
HOME Clinic<br />
Notify attending physician and complete incident report. 221-0685<br />
Kaiser Permanente Medical<br />
Center<br />
Kapiolani Medical Center<br />
Kuakini Medical Center<br />
Pali Momi Medical Center<br />
Call Dr. Jill Omori to report exposure.<br />
Report incident within 2 hours <strong>of</strong> exposure. Call<br />
operator in house “0” and ask for infection control<br />
personnel on duty.<br />
Report to Employee Health. Go to Emergency Dept, if<br />
EH closed, also call on-call Employee Health<br />
Coordinator, 983-6000).<br />
Occupational Health Services.<br />
When closed, go to ED, and also notify Nursing<br />
Supervisor (through Operator, dial “O”).<br />
Employee Health during regular work hours or<br />
Emergency <strong>Department</strong> when exposure occurs after<br />
hours. Notify supervisor. Report incident Work Injury<br />
Line.<br />
432-0000<br />
983-8525<br />
547-9531<br />
535-7200<br />
The Queen’s Medical Center Employee Health/PEP Team. 547-4004<br />
Straub Clinic and Hospital Employee Health during business hours, go directly to 522-3481<br />
ED after business hours.<br />
Tripler Army Medical Center Let care team know <strong>of</strong> exposure. Report to the ER.<br />
Report exposure to, or go to, Occupational Health the<br />
next business day.<br />
433-6235<br />
VA Clinic<br />
Contact EHU during business hours. Go to TAMC ER<br />
after hours.<br />
433-0091<br />
Wahiawa General Hospital<br />
Go to ER; also notify Nursing Supervisor (through<br />
operator) <strong>of</strong> exposure.<br />
621-4230<br />
You may also seek care and information from <strong>University</strong> Health Services (956-8965), your personal physician, or any emergency<br />
department, but seek immediate evaluation and counseling. All follow-up care after immediate evaluation services are the<br />
responsibility <strong>of</strong> the student<br />
4. Report exposure to;<br />
a. Your supervising faculty member and course/<strong>clerkship</strong> director<br />
b. Medical School Office <strong>of</strong> Student Affairs @ 692-1000;<br />
c. For URGENT after hours needs, call 692-0912, ask for Dr Smerz or Administrator on-call<br />
5. Students should be knowledgeable about their health insurance coverage, and should know what their plan will<br />
cover related to occupational exposures. Remind anyone billing for follow-up that it is NOT an Occupational<br />
Exposure, but medical follow-up, or the insurer may not want to pay for services.<br />
JABSOM’s Affiliation Agreement with Health Care Facilities (HCF) state:<br />
“Environmental exposure. In the event a medical student is exposed to an infectious, environmental, or occupational hazard at<br />
the HCF, the HCF shall be responsible for providing immediate evaluation and counseling as with employees <strong>of</strong> the HCF. Followup<br />
after the initial evaluation and counseling will not be the responsibility <strong>of</strong> the HCF, and will proceed according to <strong>University</strong><br />
student health policies.”<br />
28
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
HIV MEDICINE<br />
1:30 – 5:00 p.m.<br />
Clint Spencer Clinic<br />
Leahi Hospital<br />
All students in the Third-Year Clerkship in Internal <strong>Medicine</strong> are scheduled to attend one <strong>of</strong> the<br />
upcoming HIV <strong>Medicine</strong> sessions.<br />
This is a required <strong>clerkship</strong> activity.<br />
How to prepare for the HIV <strong>Medicine</strong> session:<br />
1. Read the 4 chapters on HIV at http://uhmed.org/images/HIV_Required_Reading.pdf<br />
2. Read about the Clint Spencer Clinic at http://www.hawaii.edu/hacrp/spencer.htm<br />
3. Read about HACRP (<strong>Hawaii</strong> AIDS Clinical Research Program) at<br />
http://www.hawaii.edu/hacrp/home2.htm<br />
4. If you are on inpatient medicine, please notify your team and chief resident <strong>of</strong> your<br />
scheduled absence to attend this required <strong>clerkship</strong> activity. Likewise, you should discuss<br />
with them whether or not you are expected to return to the hospital after this session.<br />
What to bring to the HIV <strong>Medicine</strong> session:<br />
White coat<br />
JABSOM nametag<br />
Temporary parking pass<br />
After attending the HIV <strong>Medicine</strong> session:<br />
Check <strong>of</strong>f HIV as an “S” (Special” patient encounter) on your Training Problems List<br />
Log patient(s)<br />
Evaluate teaching attending(s)<br />
29
Location and Parking:<br />
The Clint Spencer Clinic is located on the basement floor <strong>of</strong> the Young Building on the grounds <strong>of</strong><br />
Leahi Hospital at 3675 Kilauea Ave (on the block bordered by Kilauea Ave, Makapuu Ave,<br />
Maunalei Ave and Pokole St.) in Kaimuki.<br />
There is free parking in an open lot on Maunalei Ave. You may park in any unmarked stall. (Do<br />
not park in the stalls marked “Reserved for Clinical Research.”) Display your temporary parking<br />
pass on your dashboard.<br />
After parking, cross Maunalei Ave, walk on the main floor (actually the basement floor) <strong>of</strong> the<br />
main building (Young Building) and look for a sign that reads “HACRP” (<strong>Hawaii</strong> AIDS Clinical<br />
Research Program) and then the door that reads “Clint Spencer Clinic.” Check in with Joel<br />
Chapman at the reception desk.<br />
Please plan on arriving early at 1:15 p.m., especially if you are not familiar with Leahi Hospital<br />
and to allow time for parking.<br />
If you get lost, call the Clinic at 737-2751.<br />
30
TEMPORARY<br />
PARKING PASS<br />
FOR<br />
THE CLINT SPENCER<br />
CLINIC<br />
Date _______________<br />
1:30 – 5:00PM<br />
CALL 737-2751 for<br />
QUESTIONS<br />
31
MEDICINE T-RES INSTRUCTIONS<br />
General<br />
Logging all <strong>of</strong> your patients is required for JABSOM accreditation and for your <strong>clerkship</strong> grade.<br />
Failure to log properly and on a timely basis may lead to serious consequences for JABSOM<br />
and for you.<br />
You should log your patients regularly – ideally every workday so that you don’t forget and so<br />
that you don’t fall behind.<br />
You should sync your patient log regularly – at least once a week.<br />
T-Res Data Fields<br />
Complete all data fields (except 2 nd Diag which is not always needed).<br />
Date:<br />
In the Inpatient setting, the date is when you first saw the patient. This may or may not be the<br />
date <strong>of</strong> admission.<br />
In the Ambulatory setting, the date is when you see the patient. If you see a patient again for<br />
a follow-up visit, the patient should be logged again using the date <strong>of</strong> the follow-up visit.<br />
Site:<br />
In the Inpatient setting, select the hospital (KMC, QMC, TAMC)<br />
In the Ambulatory setting:<br />
o If you are working in a clinic, select the clinic (QEC, VA, Kaiser-Mapunapuna, Kaiser-<br />
Waipio, Kalihi Palama, Kokua Kalihi Valley, TAMC Clinic)<br />
or<br />
o<br />
If you are working in a physician’s <strong>of</strong>fice, select <strong>Medicine</strong> – Other Amb (Do not select<br />
Private Outpatient).<br />
Do not select Other<br />
Setting:<br />
For the Inpatient block: Select Inpatient or Special (Do not select Other)<br />
Inpatient is the patient for whom you performed a history and physical exam, and wrote daily<br />
progress notes. In other words, you provided “D” (Direct patient care) to this patient.<br />
You should log each patient only 1 time during the patient’s hospitalization. For example: If<br />
Mr. S was hospitalized for three days, although you wrote daily progress notes, you should log<br />
him only 1 time (upon his admission). If Mr. S. was discharged and then comes back to your<br />
team, you should log him again as a new patient encounter (upon his re-admission). If,<br />
however, Mr. S. went home AMA and then comes back with the same problem, you should<br />
not log him as a new patient encounter. If, however, Mr. S. went home AMA and then comes<br />
back with a different problem, you should log him as a new patient encounter.<br />
Special: Special is any patient that contributed to your education in the setting <strong>of</strong> conferences,<br />
rounds, procedures, etc. In other words, you did not provide “D” (Direct patient care) to this<br />
patient. Instead, this was an “S” (Special setting). If you wrote one or two progress notes to<br />
help out your team (but not on a daily basis), this is still an “S” (Special setting).<br />
For the Ambulatory block: Select Ambulatory or Special (Do not select Other)<br />
Ambulatory is the patient for whom you performed a history and physical exam, and wrote a<br />
note. In other words, you provided “D” (Direct patient care) to this patient.<br />
Each and every visit, including follow-up visits, should be considered a new patient encounter<br />
and logged.<br />
32
Special: Special is any patient that contributed to your education in the setting <strong>of</strong><br />
conferences, rounds, procedures, etc. In other words, you did not provide “D” (Direct patient<br />
care) to this patient. Instead, this was an “S” (Special setting).<br />
Supervisor:<br />
In the Inpatient setting, select last name MEDICINE + first name Inpt-KMC, Inpt-QMC-MTC,<br />
Inpt-QMC-UHS or Inpt-TAMC.<br />
In the Ambulatory setting, select the attending physician from the menu - except for the<br />
following situations:<br />
o If you are at QEC, select MEDICINE, QEC<br />
o If you are at TAMC IM Clinic, select MEDICINE, TAMC Clinic<br />
o If you are at VA Honolulu, select MEDICINE, VA<br />
o If you are at another VA, select your attending physician<br />
If the setting is Special, select MEDICINE, Special<br />
Do not select Other<br />
Birth Date:<br />
Enter the patient’s date <strong>of</strong> birth<br />
Sex:<br />
Select the patient’s gender<br />
Problems:<br />
Select up to 5 Training Problems that apply to the patient<br />
If none <strong>of</strong> the Training Problems apply to the patient, select None<br />
Prim Diag:<br />
Select the primary diagnoses that you addressed for this patient. You may enter up to 5<br />
diagnoses.<br />
If the diagnosis is not listed or if you have a more specific diagnosis than is listed, you can<br />
write in the diagnosis by choosing Other.<br />
2 nd Diag:<br />
Use this field if the patient has more than 5 diagnoses. You may enter up to 5 additional<br />
diagnoses, for a total <strong>of</strong> 10.<br />
Printed Reports<br />
Print an activity report according to the following schedule:<br />
o Mid-inpatient feedback meeting<br />
o Mid-ambulatory feedback meeting<br />
o End <strong>of</strong> the inpatient block<br />
o End <strong>of</strong> the ambulatory medicine block<br />
At the end <strong>of</strong> the inpatient block and at the end <strong>of</strong> the ambulatory block, your printed reports<br />
must reviewed, signed and dated by your Hospital Site Coordinator or Ambulatory Preceptor,<br />
respectively, and then turned in to the <strong>clerkship</strong>.<br />
Your Hospital Site Coordinator or Ambulatory Preceptor may request that you report additional<br />
handwritten information on your printed report (to help identify patients). However, the signed<br />
reports that you turn in to the <strong>clerkship</strong> should be copies without any additional handwritten<br />
information.<br />
Instructions for generating and printing your T-Res <strong>Medicine</strong> Activity Report:<br />
o Login to the T-Res web site: www.t-res.net<br />
o Select Lists under Reports in the left column<br />
o View report 038c – Activity Export Details for <strong>Hawaii</strong> Pediatrics<br />
o Activity Type: Internal <strong>Medicine</strong>, then View Report<br />
o Select Export as Acrobat (PDF) File<br />
o You can save a copy if you wish, otherwise select Open, then print the report<br />
33
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
<strong>Department</strong> <strong>of</strong> <strong>Medicine</strong><br />
STUDENT EVALUATION OF TEACHERS<br />
Please complete an evaluation on each <strong>of</strong> the following individuals with whom you interacted during your<br />
inpatient or ambulatory rotation:<br />
INPATIENT MEDICINE<br />
Clerkship Director - Dr. Tam<br />
Hospital Site Coordinator<br />
PBL Tutor<br />
Bedside Clinical Skills Teacher(s)<br />
Chief Medical Resident<br />
Upper Levels<br />
Interns<br />
CV PE - Dr. Fukuyama<br />
EBM - Dr. Kasuya<br />
EKG - Dr. Azuma<br />
HIV <strong>Medicine</strong> Teacher(s)<br />
HIPSTER - Dr. Ganitano<br />
Neurology - Dr. Yee<br />
AMBULATORY MEDICINE<br />
Clerkship Director - Dr. Tam<br />
Ambulatory Preceptor(s)<br />
PBL Tutor<br />
Upper Levels, if at VA<br />
Interns, if at VA<br />
CV PE - Dr. Fukuyama<br />
EBM - Dr. Kasuya<br />
EKG - Dr. Azuma<br />
HIV <strong>Medicine</strong> Teacher(s)<br />
HIPSTER - Dr. Ganitano<br />
Neurology - Dr. Yee<br />
In addition, you are also encouraged to complete evaluations on any other individuals to help the <strong>Department</strong> <strong>of</strong><br />
<strong>Medicine</strong> recognize our most outstanding teachers as well as identify those who may need further training to improve<br />
their teaching.<br />
These evaluations are anonymous. Your honest and thoughtful feedback is integral in helping the <strong>Department</strong> <strong>of</strong><br />
<strong>Medicine</strong> and its teachers improve students’ educational experiences. Your assistance is greatly appreciated. Thank<br />
you!<br />
INSTRUCTIONS<br />
1. Go to uhmed.org/db<br />
2. Login using the following: Account Name: student<br />
Password: jabsom*08<br />
3. Click on “StudentEval”<br />
4. Select “MS3”, the teacher and the academic year for which you are evaluating<br />
5. Select “Evaluation <strong>of</strong> Teacher”<br />
6. Enter your Block Number which will be emailed to you.<br />
7. Complete the evaluation form and then click submit.<br />
8. You will be given a confirmation number and the option to email it to yourself for record keeping (Do not email<br />
this number directly to Julieta, as she will not be able to identify the sender). Save this confirmation number as<br />
a pro<strong>of</strong> <strong>of</strong> your submission.<br />
9. To complete another evaluation, select “”Email & New Eval”.<br />
10. Email your confirmation number(s) to Julieta at jlrajlev@hawaii.edu<br />
34
EVALUATION FORMS<br />
35
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
OBSERVED HISTORY AND PHYSICAL<br />
Evaluation Form<br />
INSTRUCTIONS:<br />
o The Observed History and Physical should be scheduled by halfway through the inpatient block.<br />
o The Chief Medical Resident should select a patient who is unknown to the student.<br />
o The student must perform the Observed History and Physical by memory.<br />
o The student should try to finish the Observed History and Physical in 1 hour.<br />
o The student must turn in at least one (1) completed Observed History and Physical Evaluation Form to the<br />
Hospital Site Coordinator.<br />
Student_____________________________________________ Hospital (circle): KMC QMC TAMC<br />
Start Time ____:____<br />
Faculty (Chief Resident) _______________________________ Date_____________ End Time ____:____<br />
TOTAL Time ____:____<br />
A. PATIENT-PHYSICIAN RELATIONSHIP<br />
Observe whether and how the student:<br />
Maximum Score<br />
Student’s Score<br />
1. Introduces self to the patient and explains his/her role correctly 2 ( )<br />
2. Attends to the patient’s privacy and comfort 3 ( ) before beginning<br />
and throughout the history and physical<br />
3. Demonstrates effective listening skills 5 ( )<br />
(appropriate use <strong>of</strong> eye contact, posture, pauses/silence, etc.)<br />
4. Demonstrates effective verbal skills 5 ( )<br />
(appropriate use <strong>of</strong> open- and closed-ended questions,<br />
repetition, clarifying, restating, explanation, interpretation, etc.)<br />
5. Uses language that the patient understands 5 ( )<br />
B. INTERVIEW<br />
Observe whether and how the student:<br />
1. Obtains the patient’s complete history 5 ( )<br />
systematically and completely<br />
2. Balances allowing the patient to speak while 5 ( )<br />
directing questions to efficiently obtain a<br />
clear and accurate history in the time available<br />
3. Elicits the history <strong>of</strong> the present illness (HPI) 10 ( )<br />
systematically and completely<br />
4. Delineates major symptoms systematically and completely 5 ( )<br />
(location, radiation, quality, intensity, setting, onset, duration, frequency<br />
setting, aggravating and alleviating factors, associated manifestations,<br />
functional impairment, patient’s interpretation <strong>of</strong> symptoms, etc.)<br />
36
5. Obtains information for the other major sections <strong>of</strong> the history<br />
systematically and completely:<br />
Maximum Score<br />
THE BASIC PHYSICAL EXAMINATION SEQUENCE (BPES)<br />
Student’s<br />
A. GUIDELINES<br />
a. Past Medical History (PH) 5<br />
( )<br />
b. M<br />
During the physical examination, the following guidelines should be observed:<br />
e<br />
d<br />
ications (dose, route, frequency, last dose) 2 ( )<br />
c. Allergies (specific reactions and date) 2 ( )<br />
d. Family History (FH) 2 ( )<br />
e. Social History (SH) 2 ( )<br />
f. Substance Use (tobacco, alcohol and Illicit drugs) 2 ( )<br />
g. Review <strong>of</strong> Systems (ROS) 5 ( )<br />
C. PHYSICAL EXAMINATION<br />
Observe whether and how the student:<br />
1. Demonstrates proper hygienic practices 5 ( )<br />
2. Positions the patient and self properly 5 ( )<br />
for each part <strong>of</strong> the physical exam, being<br />
observant and respectful <strong>of</strong> the patient’s modesty and comfort<br />
3. Performs the patient’s complete physical exam 5 ( )<br />
systematically, completely and correctly<br />
4. Performs the basic physical examination sequence (BPES) 10 ( )<br />
systematically, completely and correctly<br />
5. Performs the appropriate branch steps 10 ( )<br />
systematically, completely and correctly<br />
Maximum<br />
Total Score<br />
Student’s<br />
Total Score<br />
100 ( )<br />
If the Student’s Total Score is < 85,<br />
the Observed History and Physical must be repeated with another patient.<br />
Comments:<br />
Chief Medical Resident’s name: _____________________________________<br />
Chief Medical Resident’s signature: __________________________________<br />
Student’s signature: ______________________________________________<br />
I received constructive and immediate feedback on my Observed History and Physical (circle): Yes No<br />
37
1. The patient always comes first - be considerate <strong>of</strong> his/her comfort and privacy.<br />
2. Students WILL wash their hands before each examination.<br />
3. While the patient must adequately disrobe, modesty should be respected at all times.<br />
4. The examiner should explain what he/she is doing during the examination.<br />
5. Never force a procedure on any adult patient.<br />
6. Reassure the patient during the examination.<br />
7. Be serious, yet maintain an appropriate sense <strong>of</strong> humor.<br />
8. Always be gentle -- a physical examination may be slightly uncomfortable if an<br />
abnormality is present. It should never be painful.<br />
9. Be systematic and thorough.<br />
Physical examination techniques and skills that are required for MD 1 are outlined in<br />
the MD 1 Handbook and are described in detail below , and in your physical diagnosis<br />
textbooks.<br />
B. STEPS OF THE BASIC PHYSICAL EXAMINATION SEQUENCE (BPES)<br />
These are the steps included in the student Basic Physical Examination Sequence<br />
(BPES). They should be performed by the student in every complete physical<br />
examination. The BPES should be completed in 30 minutes.<br />
Patient sitting: physician facing patient<br />
1. GENERAL APPEARANCE: Inspect for habitus, level <strong>of</strong> consciousness, movement,<br />
comfort, affect.<br />
2. VITAL SIGNS: Determine body temperature - read thermometer.<br />
Determine radial pulse - rate per minute and<br />
compare bilateral radial pulses simultaneously.<br />
Determine respiratory rate per minute (w hile<br />
comparing radial pulses).<br />
Determine blood pressure - place BP cuff 2.5 cm<br />
above antecubital fossa and at level <strong>of</strong> atria.<br />
Determine BP by unilateral palpation <strong>of</strong> radial pulse<br />
and then by auscultation <strong>of</strong> the brachial artery in the<br />
antecubital fossa.<br />
3. SKIN: Inspect for overall color, hair and gross lesions. (Inspect and palpate skin in<br />
detail under each regional exam below).<br />
4. HEENT: HEAD: Inspect face for symmetry, abnormality. Inspect and<br />
palpate scalp.<br />
38
EYES: Test Visual acuity. Check each eye separately (w ith<br />
corrective lenses) w ith Rosenbaum pocket chart or new sprint.<br />
Cover opposite eye. Inspect external ocular structures - inspect<br />
lids, conjunctivae, sclerae, cornea. Test Ocular muscle function<br />
and alignment (III, IV, VI). Note light reflex in neutral position. Ask<br />
patient to direct eyes laterally, superiorly and inferiorly " up and<br />
out," " dow n and out." Test pupillary response in accommodation<br />
(convergence) and to light (direct and consensual). Inspect<br />
corneas, lenses, ocular fundi (retina <strong>of</strong> each eye) w ith<br />
ophthalmoscope. Stabilize head w ith opposite hand. Ask patient<br />
to fix gaze on a specific point on the w all. Change hands and<br />
sides appropriately for examination <strong>of</strong> the other eye.<br />
EARS: Test Hearing. Use w ristw atch or w hispered voice. Inspect<br />
and palpate auricles and mastoids. Inspect canals and tympanic<br />
membranes on each side.<br />
NOSE: Palpate for tenderness and ask patient to " sniff" to test<br />
for patency <strong>of</strong> each nasal passage. Inspect each passage w ith<br />
light, using nasal speculum.<br />
MOUTH: Palpate masseters as you ask patient to " bite dow n"<br />
(V) bilaterally. Inspect for symmetry as patient " show s teeth"<br />
(VII) & " protrudes tongue" (XII). Inspect lips, teeth, gingivae,<br />
oral mucosa, tongue, under tongue, and posterior pharynx w ith<br />
tongue blade and light. Note uvula motion w hen patient says<br />
" ah" .<br />
Patient sitting: physician in front <strong>of</strong>/behind patient.<br />
(Tutor to demonstrate both techniques.)<br />
5. NECK: Inspect neck for neck veins (see below - #7). Inspect and palpate for lymph<br />
nodes -postauricular, anterior and posterior cervical, submandibular and supraclavicular<br />
bilaterally, simultaneously with both examining hands. Palpate for parotid glands bilaterally.<br />
Inspect and palpate for thyroid - each lobe separately, with patient swallowing, and<br />
palpate for trachea, from front or rear <strong>of</strong> patient.<br />
39
6. THORAX:<br />
POSTERIOR THORAX: Inspect thorax and palpate entire spine. Percuss at costovertebral angles -w ith<br />
fore-w arning Percuss for diaphragmatic excursion, from mid-thorax dow n to dullness before and after<br />
deep inspiration on each side. Percuss bilateral chest w all at equivalent areas looking for<br />
hyperresonance or dullness. Auscultate posterior and lateral lung fields -w ith diaphragm <strong>of</strong><br />
stethoscope, w hile patient is deep-breathing w ith mouth open. Compare side to side in equivalent<br />
areas.<br />
Patient sitting: physician facing patient.<br />
ANTERIOR THORAX: Inspect. Auscultate anterior lung fields beginning w ith supraclavicular areas<br />
bilaterally w ith deep breathing.<br />
Patient supine: physician at right.<br />
AXILLAE: Palpate w ith passive abduction-adduction (R hand for L axilla and<br />
vice versa).<br />
BREASTS: Inspect and palpate in all quadrants and nipples bilaterally.<br />
7. CARDIOVASCULAR:<br />
NECK: Inspect veins. Palpate carotid pulses on each side one at a time.<br />
Auscultate carotids bilaterally.<br />
HEART: Inspect precordium. Palpate apical impulse (PMI) and entire precordium w ith R hand.<br />
Auscultate w ith diaphragm <strong>of</strong> stethoscope all cardiac areas (aortic, pulmonic, LSB and apex) w ith<br />
concurrent left finger palpation <strong>of</strong> right carotid pulse for time <strong>of</strong> the heart sounds. Auscultate at<br />
pulmonic area for split S2 during inspiration. Auscultate at apex w ith bell <strong>of</strong> stethoscope (supine,<br />
and in left lateral decubitus position, for presence <strong>of</strong> S3, S4 and murmur).<br />
8. ABDOMEN:<br />
ABDOMEN: Begin by inquiring about pain. Alert patient. Ask patient to flex hips<br />
and knees to relax abdominal wall muscles.<br />
40
Inspect. Auscultate - epigastrium, left paraumbilical area over aorta for bruit and<br />
bowel sounds. Palpate - superficially and deeply in all four quadrants. Palpate deeply<br />
for aorta and for liver and spleen with deep inspiration. Palpate for spleen: turn<br />
patient to R lateral decubitus if spleen not previously felt with patient supine.<br />
INGUINAL AREAS:<br />
Inspect. Palpate for lymph nodes and/or masses<br />
and femoral arterial pulses.<br />
9. EXTREMITIES:<br />
LOWER EXTREMITIES:<br />
Inspect and palpate feet, legs, and thighs for<br />
edema. Palpate dorsalis pedis and posterior tibial<br />
pulses bilaterally and simultaneously.<br />
Patient sitting: physician facing patient.<br />
UPPER EXTREMITIES: Inspect skin, fingernails, and for tremor. Test strength- <strong>of</strong> grip bilaterally by<br />
asking patient to squeeze 2 <strong>of</strong> your fingers. Ask patient to "shrug shoulders" (XI).<br />
DEEP TENDON REFLEXES:<br />
plantar reflexes bilaterally.<br />
Test biceps, triceps, patellar, achilles reflexes and<br />
Patient standing: physician facing patient and then behind patient.<br />
POSTURE:<br />
Inspect for symmetry <strong>of</strong> shoulders, hips, and<br />
curvature <strong>of</strong> the spine.<br />
LOWER EXTREMITIES: Inspect for varicose veins, other deformities.<br />
GAIT: Inspect gait as patient walks barefoot.<br />
The follow ing is usually omitted for the video examination:<br />
MALE GENITALIA: Inspect penis (ask patient to retract foreskin) and scrotum.<br />
Palpate scrotal contents and inguinal canals.<br />
ANORECTUM: Men – have patient bend over examining table or lie in<br />
left lateral decubitus position w ith right hip and knee flexed.<br />
Women - patient in dorsosacral position w ith<br />
knees flexed and abducted (if for pelvic exam), or<br />
lying in left lateral decubitus position w ith right hip<br />
and knee flexed.<br />
Inspect anus, buttocks, and perineum.<br />
41
Palpate anal canal, rectal ampulla (and prostate in<br />
men), after gently inserting gloved and lubricated<br />
index finger.<br />
PELVIC EXAM: Instruction by obstetrician-gynecologist.<br />
C. BRANCH STEPS: (EXTENDED PHYSICAL EXAMINATION)<br />
If an abnormality is detected, it must be fully described and additional examination<br />
(branch steps) performed to clarify and delineate that finding.<br />
Example: If decreased auditory acuity is noted, the Weber and Rinne tests must be<br />
done.<br />
Such branch steps, how ever, are not part <strong>of</strong> the BPES.<br />
Branch steps are taught in separate laboratory sessions. They are useful in further<br />
elucidating abnormalities uncovered in the history and BPES and are generally not<br />
screening maneuvers (Refer to page 24).<br />
42
COMMON ERRORS OF THE BASIC PHYSICAL EXAM SEQUENCE<br />
EYES:<br />
When testing visual acuity for each eye corrected preferred, use some form <strong>of</strong><br />
measurement so that your evaluator knows that the same distance is being used for both<br />
eyes. For most pocket eye-chart cards, the card should be held 14 inches away from the<br />
eye being tested.<br />
When testing pupillary responses in accommodation and to light (direct and<br />
consensual), review the difference between accommodation and convergence. For<br />
accommodation, ask the patient to look at a distant object or the wall (for example) for<br />
distance, then have the patient look at your finger held at 2-4 inches from the bridge <strong>of</strong> his/her<br />
nose. Convergence should be tested along with ocular motor function testing.<br />
When inspecting cornea, lens and retina <strong>of</strong> each eye with ophthalmoscope, remember to<br />
turn <strong>of</strong>f the room lights. Use your right eye and hold the ophthalmoscope in your right hand when<br />
examining the patient’s right eye. Conversely, use your left eye and hold the ophthalmoscope in<br />
your left hand when examining the patient’s left eye.<br />
EARS: When testing for auditory acuity bilaterally, patient should have their eyes closed. Test<br />
one ear at a time. Begin by snapping your fingers 3 feet (arms length) away from the ear being<br />
tested. Ask the patient to indicate if he/she hears the snapping <strong>of</strong> your fingers. If the patient<br />
doesn’t hear, move closer to ear in six-inch increments and retest.<br />
NECK: Inspect and palpate thyroid, each lobe separately, and trachea with swallowing from<br />
front or back. If you choose to examine the patient from the front, identify the thyroid<br />
isthmus and then each lobe <strong>of</strong> the thyroid gland together and separately, asking the patient<br />
to swallow as you examine each side.<br />
THORAX:<br />
Review technique to percuss the lungs, percussing the posterior chest wall in<br />
symmetrical areas.<br />
Review proper technique to percuss diaphragmatic excursion on each side.<br />
Need to estimate the descent <strong>of</strong> the diaphragm when patient inspires.<br />
Review proper technique to palpate axillae with passive abduction-adduction. Your left<br />
hand should be used to examine the patient’s right axillae, using your right hand to support the<br />
patient’s right arm. Your right hand should be used to examine the patient’s left axillae, using<br />
your left hand to support the patient’s left arm.<br />
ABDOMEN:<br />
Review proper use <strong>of</strong> hands. Your left hand should be used to support the patient’s left<br />
flank and your right should be used to feel for the spleen.<br />
EXTREMITIES:<br />
Review proper technique to test for deep tendon reflexes, biceps, triceps, knee, ankle,<br />
and plantar reflexes bilaterally. Student should check patient’s bicep reflexes on each arm then<br />
tricep reflexes on each arm in order to compare bilaterally versus checking the bicep and tricep<br />
reflexes on one arm then moving to the other arm and checking the bicep and tricep reflexes.<br />
When inspecting the spine, please have patient bend over forward in order to check the<br />
curvature <strong>of</strong> their spine.<br />
43
EVALUATION OF PERFORMANCE OF<br />
BASIC PHYSICAL EXAMINATION SEQUENCE<br />
Student: Date: _________ Evaluator: ___________________<br />
Steps Done Not<br />
Done<br />
Seq.<br />
Incor<br />
.<br />
Tech<br />
.<br />
Incor<br />
.<br />
Comments<br />
1. General Appearance: (sitting)<br />
Inspect overall<br />
2. Vital Signs (sitting)<br />
A. Temperature with thermometer<br />
B. Pulse - Measure rate per minute<br />
Compare bilaterally<br />
C. Respiratory - rate per minute<br />
D. Blood pressure - Palpation (unilateral)<br />
(unilateral)<br />
- Auscultation<br />
3. Skin (sitting)<br />
Inspect overall<br />
4. HEENT<br />
A. Head - Inspect face<br />
Inspect/palpate scalp<br />
B. Eyes (sitting)<br />
Test visual acuity for each eye,<br />
corrected preferred<br />
Inspect lids, conjunctivae, sclerae,<br />
corneas<br />
Test extraocular muscle movements<br />
and convergence<br />
Test pupillary responses to light (direct<br />
and consensual) and to accomodation<br />
Inspect cornea, lens and retina <strong>of</strong> each<br />
eye with ophthalmoscope<br />
C. Ears (sitting)<br />
Test for auditory acuity bilaterally<br />
Inspect and palpate auricles and<br />
mastoids<br />
Inspect canals and tympanic<br />
membranes<br />
44
Steps Done Not<br />
Done<br />
Seq.<br />
Incor<br />
.<br />
Tech<br />
.<br />
Incor<br />
.<br />
Comments<br />
D. Nose (sitting)<br />
Palpate nose and sinuses for<br />
tenderness<br />
Test patency <strong>of</strong> each nasal passage by<br />
asking patient to "sniff"<br />
Inspect each nasal passage with<br />
speculum<br />
E. Mouth (sitting)<br />
Test CN V - "bite down" palpate<br />
masseter<br />
Examine CN VII - "show teeth"<br />
Test CN XII - "protrude tongue"<br />
Inspect lips, teeth, gingivae, tongue,<br />
posterior pharynx: "say ah"<br />
5. Neck (sitting)<br />
Inspect for neck veins (see below also)<br />
Inspect/palpate for postauricular, cervical,<br />
sub-mandibular and supraclavicular nodes<br />
Palpate for parotid gland on each side<br />
Inspect and palpate thyroid (each lobe<br />
separately), (and trachea) with swallowing<br />
6. Thorax (sitting)<br />
A. Posterior Thorax (sitting)<br />
Inspect posterior thorax with<br />
respiration<br />
Inspect and palpate entire spine<br />
Percuss costovertebral angles for<br />
tenderness<br />
Percuss posterior thorax bilaterally and<br />
symmetrically<br />
Percuss diaphragmatic excursion<br />
bilaterally<br />
Auscultate posterior lung fields<br />
bilaterally with deep inspiration<br />
Auscultate lateral lung fields bilaterally<br />
B. Anterior Thorax (sitting)<br />
Inspect anterior thorax with respiration<br />
45
Steps Done Not<br />
Done<br />
Seq.<br />
Incor<br />
.<br />
Tech<br />
.<br />
Incor<br />
.<br />
Comments<br />
Auscultate anterior lung fields<br />
bilaterally (starting with supraclavicular area)<br />
with deep inspiration<br />
C. Axillae (supine) Palpate axillae with<br />
passive abduction- adduction<br />
D. Breasts (supine)<br />
Inspect & palpate breasts including<br />
nipples<br />
7. Cardiovascular (supine)<br />
A. Neck Veins/arteries: Inspect, palpate,<br />
auscultate carotid arteries bilaterally one at a<br />
time<br />
B. Heart (supine) Inspect precordium<br />
Palpate PMI (apical impulse) &<br />
precordium<br />
Auscultate with diaphragm at aortic and<br />
pulmonic areas, LSB and apex<br />
Auscultate for splitting <strong>of</strong> S 2 in pulmonic<br />
area<br />
left<br />
Auscultate with bell at apex (supine &<br />
lateral decubitus)<br />
8. Abdomen (supine; hips and knees flexed)<br />
Alert patient to abdominal exam<br />
Inspect abdomen<br />
for<br />
Auscultate epigastrium and over aorta<br />
bruit, and bowel sounds<br />
Palpate superficially/deeply in 4<br />
quadrants<br />
Palpate for liver<br />
Palpate for aorta<br />
Palpate for spleen - supine position<br />
- R lateral decubitus<br />
Inspect and palpate for inguinal nodes<br />
and femoral pulses in inguinal areas<br />
bilaterally<br />
9. Extremities<br />
A. Lower Extremities (supine)<br />
Inspect and palpate legs and feet for edema<br />
46
Steps Done Not<br />
Done<br />
Seq.<br />
Incor<br />
.<br />
Tech<br />
.<br />
Incor<br />
.<br />
Comments<br />
Palpate dorsalis pedis & posterior tibial<br />
pulses bilaterally<br />
B. Upper Extremities (sitting)<br />
Inspect skin and nails. Observe for<br />
tremor<br />
Examine grip<br />
Examine CN XI ("shrug shoulders")<br />
Test for deep tendon reflexes, biceps,<br />
triceps, knee, ankle, and plantar<br />
reflexes bilaterally<br />
C. Posture (standing) - Inspect spine<br />
D. Lower Extremities (standing)<br />
Inspect for varicosities<br />
E. Gait - Inspect walking<br />
Did student respect patient's privacy?<br />
No<br />
Did student arouse patient's anxiety?<br />
No<br />
Yes<br />
Yes<br />
Did student display appropriate affect?<br />
No<br />
Yes<br />
Did student use appropriate verbal/nonverbal behavior? Yes<br />
No<br />
47
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
OBSERVED PATIENT COUNSELING<br />
Evaluation Form<br />
Complete 2 during ambulatory medicine and turn in to your Ambulatory Preceptor.<br />
Student: __________________________ Site: ________________ Date: __________<br />
Setting: _____ Inpatient<br />
Counseling was directed at: _____ Patient<br />
_____ Ambulatory (check one or both) _____ Patient’s family<br />
Counseling:<br />
___ Explain diagnoses<br />
___ Explain tests, procedures or surgery<br />
___ Review results <strong>of</strong> tests, procedures or surgery<br />
___ Review medications (indications, dosing, side effects, etc.)<br />
___ Review diets, exercise or other lifestyle changes<br />
___ Discuss smoking cessation<br />
___ Discuss alcohol use<br />
___ Discuss compliance (medications, follow-up, etc.)<br />
___ Review discharge instructions<br />
___ Other (specify) ___________________________<br />
Good<br />
Needs Improvement<br />
Student used clear and understandable language.<br />
Student adapted to patient’s/family’s readiness to learn.<br />
Student adapted to patient’s/family’s comprehension level<br />
All pertinent information was presented accurately.<br />
Student demonstrated empathy and compassion.<br />
Patient’s/family’s comprehension was assessed.<br />
Evaluator Comments:<br />
Evaluator’s name _________________________<br />
Evaluator’s signature _______________________<br />
Student’s signature _______________________<br />
I received constructive feedback on my Observed Patient Counseling (circle): Yes No<br />
48
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
CASE PRESENTATION<br />
Evaluation Form<br />
Before presenting, the student should give this form to the attending or resident leading rounds. Afterwards, the<br />
student should turn the form in to the Hospital Site Coordinator.<br />
Student: _______________________________________<br />
Date: _______________<br />
Rounds:<br />
___ Attending Rounds<br />
___ Bedside Clinical Skills<br />
___ ICU Rounds<br />
___ Morning Report<br />
___ PBL Tutorial<br />
___ Other Rounds/Conference __________________<br />
Major problems/diagnoses <strong>of</strong> case presented:<br />
1. ___________________________<br />
2. ___________________________<br />
3. ___________________________<br />
Presentation was clear<br />
Presentation was organized<br />
Presentation was memorized<br />
All pertinent history was presented<br />
accurately<br />
All pertinent physical findings were<br />
presented accurately<br />
All pertinent labs were presented<br />
accurately<br />
All pertinent problems were correctly<br />
identified<br />
Assessment was appropriate for level <strong>of</strong><br />
training<br />
Plan (diagnostic, therapeutic, education)<br />
was appropriate for level <strong>of</strong> training<br />
Comments:<br />
Exceptional<br />
Very<br />
Competent Competent Marginal Unsatisfactory<br />
Evaluator:<br />
Print _____________________________<br />
Signature _________________________<br />
49
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
SMALL GROUP LEARNING EXPERIENCE<br />
Evaluation Form<br />
Student: ____________________ Date: _________ Activity: ____ PBL Tutorial<br />
____ Bedside Clinical Skills<br />
____ Chief Rounds<br />
____ Other: ___________<br />
Check appropriate box on this Rating Scale:<br />
Activity<br />
Participates actively<br />
Shares knowledge<br />
Respects opinions and learning<br />
needs <strong>of</strong> others<br />
Asks thoughtful questions<br />
Facilitates group process<br />
Demonstrates appropriate fund<br />
<strong>of</strong> knowledge for MS3<br />
Demonstrates appropriate<br />
clinical skills for MS 3<br />
Is properly prepared for this<br />
activity<br />
Evaluator Comments:<br />
Exceptional<br />
Very<br />
Competent<br />
Competent Marginal Unsatisfactory<br />
Evaluator’s name: ___________________ Evaluator’s signature: _____________________<br />
Student’s signature _________________<br />
50
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
MID-CLEKSHIP FEEDBACK FORM<br />
Student’s name: ___________________________________________________<br />
Considering the three domains <strong>of</strong> Medical Knowledge, Clinical Skills and Pr<strong>of</strong>essionalism,<br />
This student’s STRENGTHS are:<br />
This student NEEDS TO WORK AND IMPROVE ON:<br />
Overall, this student’s progress to date is:<br />
___ Satisfactory<br />
___ Unsatisfactory<br />
Evaluator’s name: ___________________________<br />
Student's signature: __________________________<br />
Signature: _____________________________<br />
Date reviewed with student: _______________<br />
Please make a photocopy <strong>of</strong> this form after it is completed, reviewed and signed by both the Evaluator and the<br />
Student.<br />
Instructions for the Student:<br />
Keep a photocopy <strong>of</strong> this form after your Hospital Site Coordinator or Ambulatory Preceptor completes and reviews it with<br />
you.<br />
You should actively work on and improve the areas identified above.<br />
You will be instructed on how to turn in the completed form at the end <strong>of</strong> your inpatient block and at the end <strong>of</strong> your<br />
ambulatory block.<br />
Instructions for the Evaluator:<br />
Please keep a copy and include the information in your final Student Evaluation Form.<br />
Specifically, if you identified any areas to work on and improve, please comment on whether the student successfully<br />
responded to your feedback and improved by the end <strong>of</strong> the block.<br />
51
Exceptional<br />
Very Competent<br />
Competent<br />
Marginal<br />
Unsatisfactory<br />
Not Evaluated<br />
UH John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
STUDENT EVALUATION FORM<br />
Student: _____________________________________<br />
Ambulatory Site: _______________________<br />
Block: _____ Dates <strong>of</strong> rotation: _____________________ Date <strong>of</strong> this report: ___________________<br />
IMPORTANT:<br />
o Comments are MANDATORY for any Exceptional, Marginal or Unsatisfactory ratings.<br />
<br />
I. Life-Long Learning Skills<br />
Graduates will be life-long learners.<br />
Demonstrates enthusiasm, motivation and self-initiative to learn<br />
Identifies relevant learning issues, searches for and critically appraises information<br />
(self-directed learning)<br />
Comments:<br />
II.<br />
The Biological Sciences<br />
Graduates will understand the biological sciences underlying clinical medicine.<br />
Demonstrates basic science knowledge (including anatomy, physiology,<br />
pathology and pathophysiology)<br />
Demonstrates clinical knowledge (including knowledge <strong>of</strong> the illnesses seen in the<br />
adult patient/population in <strong>Hawaii</strong>, Asia-Pacific region and globally)<br />
Applies basic science knowledge to clinical situations<br />
Comments:<br />
52
Exceptional<br />
Very Competent<br />
Competent<br />
Marginal<br />
Unsatisfactory<br />
Not Evaluated<br />
<br />
<br />
III. The Care <strong>of</strong> Patients<br />
Graduates will be able to care for their patients under the supervision <strong>of</strong> faculty.<br />
Demonstrates respect and compassion for patients and their families<br />
Serves as an effective patient advocate<br />
Interviews patients in a systematic, organized and thorough manner<br />
(History Taking)<br />
Examines patients in a systematic, organized and thorough manner<br />
(Physical Exam)<br />
Formulates appropriate Assessments, Problem Lists and Differential Diagnoses<br />
Formulates appropriate Diagnostic Plans<br />
Formulates appropriate Therapeutic Plans<br />
Educates and counsels patients (and their families) about their health and<br />
medical problems<br />
Demonstrates clinical judgment and problem solving skills<br />
Works efficiently<br />
Comments:<br />
IV. Oral and Written Communication Skills<br />
Graduates will be able to communicate effectively with patients, families and other<br />
healthcare providers.<br />
Uses effective verbal and non-verbal communication skills (including listening<br />
and using language appropriate for each patient, family and clinical setting)<br />
Presents cases in a systematic, organized and thorough manner that is accurate<br />
and appropriate for the clinical setting<br />
Writes notes (write-ups and progress notes, etc.) in a systematic, organized and<br />
thorough manner that is accurate, legible and appropriate for the clinical setting<br />
Comments:<br />
53
Exceptional<br />
Very Competent<br />
Competent<br />
Marginal<br />
Unsatisfactory<br />
Not Evaluated<br />
<br />
V. Pr<strong>of</strong>essionalism<br />
Graduates will be pr<strong>of</strong>essional and ethical, demonstrate an enthusiasm for medicine, and value<br />
honor, integrity, altruism, respect, accountability, excellence, scholarship, and leadership<br />
while delivering compassionate care to their patients.<br />
Demonstrates pr<strong>of</strong>essional appearance and attire<br />
Attends all required <strong>clerkship</strong> and training site-specific activities; is punctual<br />
Listens attentively and participates actively<br />
Completes all <strong>clerkship</strong> and patient care responsibilities on time<br />
Demonstrates pr<strong>of</strong>essional behavior<br />
Demonstrates pr<strong>of</strong>essional relationships (with attendings, residents, students,<br />
nurses, other health care workers, patients and their families)<br />
Seeks, accepts and responds positively and effectively to feedback<br />
Works as an effective team member<br />
Comments:<br />
COMMENTS:<br />
Ambulatory Preceptor’s name: ___________________________________________<br />
Ambulatory Preceptor’s signature: ____________________________ Date: _________________<br />
Student’s signature: ______________________________________<br />
Date: _________________<br />
Please return this form to:<br />
Julieta Rajlevsky<br />
UH <strong>Department</strong> <strong>of</strong> <strong>Medicine</strong><br />
1356 Lusitana St., 7 th Floor, Honolulu, HI 96813<br />
Fax: (808) 586-7486 Phone: (808) 586-7478<br />
54
UNIVERSITY OF HAWAII JOHN A. BURNS SCHOOL OF MEDICINE<br />
THIRD-YEAR CLERKSHIP IN INTERNAL MEDICINE<br />
STUDENT EVALUATION FORM<br />
Ratings Definitions<br />
EXCEPTIONAL:<br />
The student consistently demonstrates medical knowledge, clinical skills or pr<strong>of</strong>essionalism at a level<br />
higher than expected for a third year student. In other words, the student consistently “goes the extra mile”<br />
and performs “above and beyond” in the item rated.<br />
Comments are mandatory for this rating.<br />
VERY COMPETENT:<br />
The student on occasion demonstrates medical knowledge, clinical skills or pr<strong>of</strong>essionalism at a level<br />
higher than expected for a third year student. In other words, the student on occasion, but not consistently,<br />
“goes the extra mile” and performs “above and beyond” in the item rated. The student should continue to<br />
strive for Exceptional ratings.<br />
COMPETENT:<br />
The student demonstrates medical knowledge, clinical skills or pr<strong>of</strong>essionalism at the level expected for a<br />
third year student. Note that the <strong>clerkship</strong> expects that most students will receive Competent ratings for the<br />
majority <strong>of</strong> items. Some students in the past have incorrectly interpreted Competent ratings as punitive.<br />
On the contrary, this rating merely indicates that the student performed at the expected level for that<br />
particular item. The student should continue to strive for Very Competent and Exceptional ratings.<br />
MARGINAL:<br />
The student demonstrates medical knowledge, clinical skills or pr<strong>of</strong>essionalism slightly below the level<br />
expected for a third year student. An item rated Marginal is an area <strong>of</strong> weakness that has been identified.<br />
The student will be expected to work on this area <strong>of</strong> weakness and demonstrate improvement to the level<br />
expected for a third year student. A Marginal rating probably precludes an Honors grade.<br />
Comments are mandatory for this rating.<br />
UNSATISFACTORY:<br />
The student demonstrates medical knowledge, clinical skills or pr<strong>of</strong>essionalism below the level expected<br />
for a third year student. An item rated Unsatisfactory is an area <strong>of</strong> weakness that has been identified.<br />
Formal remediation may be required. An Unsatisfactory rating precludes an Honors grade.<br />
Comments are mandatory for this rating.<br />
55
OTHER FORMS<br />
56
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
MS3-RESIDENT<br />
INPATIENT MEDICINE AGREEMENT FORM<br />
(Revised 8/11/12)<br />
Name <strong>of</strong> MS3 _______________________________________________<br />
1. The upper level (UL) resident (Level 2 or 3) is responsible for the third-year medical<br />
student’s inpatient medicine experience. At the beginning and throughout the student’s<br />
inpatient experience, the UL should clarify what is expected <strong>of</strong> the student.<br />
2. The earliest time that the student is permitted to arrive at the hospital is:<br />
o 4:00 a.m. at Kuakini<br />
o 5:00 a.m. at Queen’s<br />
o 5:00 a.m. at Tripler<br />
The earliest time that the student is permitted to see patients is:<br />
o 4:30 a.m. at Kuakini<br />
o 5:30 a.m. at Queen’s<br />
o 5:30 a.m. at Tripler<br />
3. The student must take every call with his/her team throughout the inpatient rotation.<br />
Call at Kuakini:<br />
The student must take every call (q4) with his/her team throughout the inpatient rotation.<br />
Overnight Call - 1 required, preferably a Fri night<br />
If the student is unable to take overnight call on a Fri night, he/she must talk to the<br />
CMR and the Hospital Site Coordinator about taking overnight call on a Sat instead.<br />
Call – q4 days until 10 p.m. at the latest<br />
(May leave earlier depending on admissions and UL approval.)<br />
Non-Call Days – The student will assist his/her team until after the team signs out.<br />
Call at Queen’s:<br />
The student must take every call (q4) with his/her team throughout the inpatient rotation.<br />
Overnight Call - none<br />
Long Call – q4 days until 10 p.m. at the latest<br />
(May leave earlier depending on admissions and UL approval.)<br />
Non-Call Days –The student will assist his/her team with admitting patients and may<br />
leave after team is done with work, with UL approval.<br />
Call at Tripler:<br />
The student must take every call (q4) with his/her team throughout the inpatient rotation.<br />
Overnight Call - none<br />
Long Call: 0600 – 1900 q4 days<br />
Short Call: 0600 – 1600 all other days - The student will assist his/her team until sign<br />
out.<br />
4. The UL is responsible for assigning patients to the student (see Training Problems List).<br />
The student will admit 1 - 2 patients per call.<br />
The student should actively follow an average <strong>of</strong> 2 patients at all times (maximum 5).<br />
57
5. The student must interview and examine patients on his/her own. The student may<br />
observe the Intern and/or UL obtain the history and physical, but this observation does not<br />
qualify as the student’s history and physical.<br />
6. The student must pre-round and write daily Progress Notes on all his/her assigned<br />
patients before the Intern and/or UL write their notes. The UL should review the<br />
Progress Notes with the student, give constructive feedback and countersign the note.<br />
7. The UL is responsible for insuring proper supervision <strong>of</strong> the following parts <strong>of</strong> the<br />
physical exam performed by the student: female breast exams, pelvic exams, rectal<br />
exams and prostate exams. The supervision must be provided by a physician (such as<br />
Interns, ULs, Chief Residents or Attendings).<br />
8. The UL is responsible for insuring proper supervision <strong>of</strong> any procedure performed<br />
by the student. The supervision must be provided by a physician (such as Interns, ULs,<br />
Chief Residents or Attendings) who is certified or has expertise to competently perform<br />
the procedure in question. Note that there are no required procedures for students.<br />
9. The UL should assist the student in preparing case presentations at hospital rounds<br />
or conferences at a level that is appropriate for the student’s training. Whenever a<br />
student’s patient will be presented, the student is expected to be the one presenting the<br />
patient (unless it is an ICU patient at Kuakini – then it is up to the CMR and HSC).<br />
10. The student must have one (1) day <strong>of</strong>f per week, either a Saturday or a Sunday.<br />
At Kuakini, the day <strong>of</strong>f should be on Sunday - unless the student has call on Sunday, in<br />
which case the student will take Saturday <strong>of</strong>f.<br />
11. The student must inform the UL <strong>of</strong> the student’s activities and whereabouts at all<br />
times. Specifically, the student must notify the UL whenever leaving the hospital,<br />
including leaving to attend required 3 rd year or <strong>clerkship</strong> activities or to study, and should<br />
discuss if or when he/she needs to return.<br />
12. When the UL is absent or <strong>of</strong>f, the Intern should assume the UL’s role and<br />
responsibilities, including all those listed above, in supervising the student.<br />
13. The Intern and UL should discuss medical student issues and problems with the<br />
Chief Resident and/or Hospital Site Coordinator as soon as possible.<br />
1 st Upper Level Resident:<br />
Name _______________________ Signature ______________________ Date _________<br />
(Required by end <strong>of</strong> MS3’s 1 st week)<br />
2nd Upper Level Resident:<br />
Name _______________________ Signature ______________________ Date_________<br />
(Required by end <strong>of</strong> UL’s 1 st week)<br />
58
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
INPATIENT WORK HOURS LOG<br />
Student _____________________________________<br />
Inpatient site (circle) KMC QMC TAMC<br />
Week ___ beginning ____/_____/2012<br />
On Call?<br />
Other Activities?<br />
# New Patients<br />
(admissions, transfers)<br />
# Old Patients<br />
TOTAL # PATIENTS<br />
For KMC,<br />
# ICU Patients<br />
Time In<br />
Time Out<br />
TOTAL # HOURS<br />
MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY<br />
TOTAL # HOURS FOR THE WEEK: _______<br />
o<br />
o<br />
o<br />
o<br />
o<br />
o<br />
o<br />
o<br />
o<br />
o<br />
o<br />
o<br />
Please log your hours daily – otherwise it’s difficult to remember.<br />
You should log only the hours that you are "working" which includes patient care and required 3 rd year, hospital and <strong>clerkship</strong> activities such as Colloquia, rounds, conferences,<br />
PBL Tutorials, Bedside Clinical Skills, Chief Rounds, CV PE, EBM, EKG, HIV <strong>Medicine</strong>, METS Sim Session, Neuro, etc.<br />
It's ok to include meals in the middle <strong>of</strong> your “work day” (as long as it's not a 1 hr lunch!) – it’s too much trouble to clock out for lunch and then clock in afterwards.<br />
You should not include meals at the hospital before/after your “work day” or reading at the hospital before/after your “work day.”<br />
You should not include writing your Comprehensive Write-ups and LIs – even if done at the hospital - since that is "home" work.<br />
You should work no more than 80 hours per week, averaged over the course <strong>of</strong> the entire <strong>clerkship</strong>.<br />
You should have 1 day <strong>of</strong>f per week, usually a Sat or Sun.<br />
You should follow the holiday schedule observed by your site, since this varies by site.<br />
On Call? If relevant, please specify Short, Long, or Overnight.<br />
Other Activities? Please specify <strong>of</strong>f-campus activities. Ex: Colloquia, HIV <strong>Medicine</strong>, METS Sim Session, etc.<br />
# Patients is the # <strong>of</strong> patients (counted at the end <strong>of</strong> each day) that you are actively following - that is, pre-rounding on, writing notes on and presenting.<br />
Ask your UL to sign the following Monday _____________________________________________Then turn completed Log in to your CMR/Hospital Site Coordinator.<br />
59
PHYSICIAN’S ORDERS<br />
DATE: / / TIME:<br />
IMPORTANT<br />
INSTRUCTIONS<br />
► 1. All orders must be written in metric system<br />
2. Write with ball point pen only<br />
SIGNATURE<br />
DATE: / / TIME:<br />
SIGNATURE<br />
DATE: / / TIME:<br />
SIGNATURE<br />
60
APPENDICES<br />
61
U.H. John A. Burns School <strong>of</strong> <strong>Medicine</strong><br />
Third-Year Clerkship in Internal <strong>Medicine</strong><br />
TRAINING PROBLEMS LIST<br />
You are required to see at least one patient with each <strong>of</strong> the 33 Training Problems during the course <strong>of</strong> this <strong>clerkship</strong>.<br />
This is the minimum requirement. Your goal, however, should be to see at least one inpatient patient and one<br />
ambulatory patient with each <strong>of</strong> the Training Problems. The Training Problem does not have to be the patient’s Chief<br />
Complaint. In fact, a patient may present with many Training Problems.<br />
Of course, the more patients you see with these Training Problems, the more you will learn.<br />
Keep track <strong>of</strong> your patient encounters in the chart below.<br />
Indicate which encounters involved Direct Patient Care (D) and which encounters did not involve direct patient care,<br />
referred to as “Special” (S), as in your PDA Patient Log.<br />
It is your responsibility to insure that you have seen patients with each <strong>of</strong> the 33 Training Problems by the end <strong>of</strong> the<br />
<strong>clerkship</strong>. You are advised to see your Upper Level Resident, Chief Medical Resident and/or Hospital Site Coordinator<br />
(when you are on inpatient medicine) or Ambulatory Preceptor (when you are on ambulatory medicine) as soon as<br />
possible to assist you in finding appropriate patients.<br />
Please refer to the Student Handbook for the Specific Learning Objectives for each Training Problem.<br />
Your study <strong>of</strong> Internal <strong>Medicine</strong> in this <strong>clerkship</strong> should be guided by these Training Problems and their Specific Learning<br />
Objectives.<br />
Inpatient<br />
Ambulatory<br />
-- -- D S 1. Healthy Patient:<br />
Health promotion, disease prevention and screening<br />
(i.e. annual or routine physical exam)<br />
Patients with a symptom, sign or<br />
lab abnormality (14):<br />
D S D S 2. Abdominal pain<br />
D S D S 3. Altered mental status<br />
D S D S 4. Anemia<br />
D S D S 5. Back pain<br />
D S D S 6. Chest pain<br />
D S D S 7. Cough<br />
D S D S 8. Dyspnea<br />
D S D S 9. Dysuria<br />
D S D S 10. Fever<br />
D S D S 11. Fluid, electrolyte & acid-base disorders<br />
D S D S 12. GI bleeding<br />
D S D S 13. Knee pain<br />
D S D S 14. Rash<br />
D S D S 15. Upper respiratory complaints<br />
62
TRAINING PROBLEMS LIST (continued)<br />
Inpatient<br />
Ambulatory<br />
Patients with a known condition<br />
(18):<br />
D S D S 16. Acute MI<br />
D S D S 17. Acute renal failure & Chronic kidney<br />
disease<br />
D S D S 18. Common cancers<br />
D S D S 19. COPD & Obstructive airways disease<br />
D S D S 20. Diabetes mellitus<br />
D S D S 21. Dyslipidemias<br />
D S D S 22. Heart failure<br />
D S D S 23. HIV infection<br />
D S D S 24. Hypertension<br />
D S D S 25. Liver disease<br />
D S D S 26. Major depression<br />
D S D S 27. Nosocomial infections<br />
D S D S 28. Obesity<br />
D S D S 29. Pneumonia<br />
D S D S 30. Rheumatologic problems<br />
D S D S 31. Smoking cessation<br />
D S D S 32. Substance abuse<br />
D S D S 33. Venous thromboembolism<br />
Complete the Inpatient half <strong>of</strong> this 2 page chart by your last day <strong>of</strong> inpatient medicine, including your Hospital Site<br />
Coordinator’s signature, and then turn in to Julieta Rajlevsky in the Dept <strong>of</strong> <strong>Medicine</strong> at UHT 7 th fl.<br />
Complete the Ambulatory half <strong>of</strong> this 2 page chart by your last day <strong>of</strong> ambulatory medicine, including your<br />
Ambulatory Preceptor’s signature, and then turn in to Julieta Rajlevsky in the Dept <strong>of</strong> <strong>Medicine</strong> at UHT 7 th fl.<br />
Student_____________________________<br />
Name<br />
____________________________ Date____________<br />
Signature<br />
Hospital Site Coordinator____________________ _____________________________ Date____________<br />
Name<br />
Signature<br />
Ambulatory Preceptor______________________<br />
Name<br />
_____________________________ Date ____________<br />
Signature<br />
63
TRAINING PROBLEM #1: THE HEALTHY PATIENT: HEALTH<br />
PROMOTION, DISEASE PREVENTION, AND SCREENING<br />
RATIONALE:<br />
The growing appreciation for the contributions <strong>of</strong> screening, prevention, and health promotion to<br />
health outcomes necessitates that basic clinical education incorporate advances made in this<br />
area. Especially important are those interventions that relate to prevention <strong>of</strong> cardiovascular<br />
disease, the early detection and treatment <strong>of</strong> potentially curable cancers, and to optimizing care<br />
for chronic diseases.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to obtain a patient history that includes a family history and an assessment <strong>of</strong> risk<br />
factors.<br />
Knowledge <strong>of</strong> the warning signs <strong>of</strong> common cancers.<br />
Knowledge <strong>of</strong> basic criteria and principles <strong>of</strong> health screening.<br />
Knowledge <strong>of</strong> clinical epidemiologic concepts as they pertain to estimation <strong>of</strong> health risk and<br />
quantitative rationale for screening.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The epidemiology and definitions <strong>of</strong> hypertension, its contribution to cardiovascular risk, the<br />
impact <strong>of</strong> treatment on risk, and current. Recommendations for screening. (MK)<br />
2. The epidemiology <strong>of</strong> hyperlipidemia, its contribution to cardiovascular risk, the reliability <strong>of</strong><br />
testing modalities, the impact <strong>of</strong> treatment on cardiovascular risk, and current<br />
recommendations for screening. (MK)<br />
3. The epidemiology <strong>of</strong> common cancers, including:<br />
Breast cancer, including the efficacy <strong>of</strong> available screening modalities, impact <strong>of</strong> early<br />
treatment on survival, and current recommendations for screening. (MK)<br />
Common skin cancers, including the warning signs <strong>of</strong> melanoma and basal and squamous<br />
cell carcinoma. (MK)<br />
Cervical cancer, including the utility <strong>of</strong> the Pap smear, impact <strong>of</strong> early treatment on<br />
outcome, and current recommendations for screening.(MK)<br />
Colorectal cancer, including the utility <strong>of</strong> available screening methodologies, the impact <strong>of</strong><br />
early treatment on outcome, and current screening recommendations. (MK)<br />
Prostate cancer, including the utility <strong>of</strong> available screening modalities, impact <strong>of</strong> early<br />
treatment on outcome, and current screening recommendations. (MK)<br />
4. The risks, benefits, methods, and recommendations for immunizing adults against hepatitis B,<br />
influenza, pneumococcal infection, tetanus/diphtheria, and mumps/measles/rubella. (MK)<br />
5. Safe sexual practices and risks, benefits, and efficacy <strong>of</strong> common methods <strong>of</strong> contraception.<br />
(MK)<br />
6. Efficacy <strong>of</strong> seat belt use and proper belt application. (MK)<br />
7. Efficacy <strong>of</strong> exercise and weight loss in prevention <strong>of</strong> cardiovascular disease and recommended<br />
exercise programs. (MK)<br />
8. The clinical presentations <strong>of</strong> substance abuse and basic approaches to prevention and<br />
treatment. (MK)<br />
64
9. The impact <strong>of</strong> smoking on cardiovascular and cancer risk and basic approaches to smoking<br />
cessation. (MK)<br />
10. Daily caloric, fat, carbohydrate, protein, mineral, and vitamin requirements; adequacy <strong>of</strong> diets<br />
in providing such requirements; evidence <strong>of</strong> need for supplements (e.g. calcium, antioxidants).<br />
(MK)<br />
11. The functional status assessment in the geriatric patient and its impact on assuring the best<br />
possible functional state. (MK)<br />
12. Common environmental and occupational hazards. (MK)<br />
13. Controversies and differences that exist in the recommendations for preventive measures and<br />
screening. (MK)<br />
B. SKILLS: Students should demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history, including:<br />
Dietary intake <strong>of</strong> fats and cholesterol. (PC, CS)<br />
Exercise and activity levels. (PC, CS)<br />
Substance use and its effects, including tobacco, alcohol, and elicit drugs. (PC, CS)<br />
Psychosocial stresses and environmental risks. (PC, CS)<br />
Specific cancer risks (e.g. family history, exposures, warning symptoms, preventive efforts).<br />
(PC, CS)<br />
Any high-risk sexual practices. (PC, CS)<br />
Immunization status appropriate for adults, including:<br />
o Diphtheria/tetanus for all adults. (PC, CS)<br />
o Influenza vaccine and pneumococcal vaccine for the elderly and those with underlying<br />
chronic disease. (PC, CS)<br />
o Rubella for sero-negative women <strong>of</strong> child-bearing age. (PC, CS)<br />
o Hepatitis B vaccine for medical personnel and other at-risk populations. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam with features<br />
depending on age/sex/race and medical history <strong>of</strong> an individual, including:<br />
Screening skin examination for signs <strong>of</strong> malignancy. (PC)<br />
Screening breast examination for a dominant nodule and secondary signs <strong>of</strong> malignancy.<br />
(PC)<br />
Participation in obtaining a Pap smear. (PC)<br />
Screening rectal examination that includes palpation <strong>of</strong> the prostate gland, identification <strong>of</strong><br />
any nodules, and performance <strong>of</strong> a stool test for occult blood. (PC)<br />
Performance <strong>of</strong> a functional status examination in the geriatric patient (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
using specific history, physical exam, and laboratory findings identified during the screening<br />
examination (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend and interpret laboratory<br />
tests for screening purposes, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and other tests may include, when<br />
appropriate:<br />
Complete blood count. (PC, MK)<br />
Fasting lipid panel. (PC, MK)<br />
Fasting blood glucose. (PC, MK)<br />
Urinalysis. (PC, MK)<br />
65
Stool test for occult blood. (PC, MK)<br />
Prostate specific antigen. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) results<br />
<strong>of</strong>:<br />
Mammography. (PC, MK)<br />
Colonoscopy. (PC, MK)<br />
Pap smear. (PC, MK)<br />
Bone densitometry. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate results <strong>of</strong> the evaluation and counsel for disease prevention. (PC, CS)<br />
Elicit questions from the patient and his or her family about the plan. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Perform a urinalysis (dipstick and microscopic). (PC)<br />
Stool occult blood testing. (PC)<br />
Calculate a BMI. (PC)<br />
Perform a functional status examination for elderly patients. (PC)<br />
Administer intramuscular injection <strong>of</strong> a vaccine. (PC)<br />
Participate in obtaining a Pap smear. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for healthy patients, including:<br />
Designing an appropriate work-up for any abnormalities noted on the screening exam. (PC,<br />
MK)<br />
Teaching breast self-examinations. (PC, CS)<br />
Counseling for:<br />
o Safe sexual practices. (PC, CS)<br />
o Seatbelt use. (PC, CS)<br />
o Healthy diet. (PC, CS)<br />
o Weight loss. (PC, CS)<br />
o Practical exercise program appropriate to the patient's age, and current physical<br />
condition. (PC, CS)<br />
o Stress management. (PC, CS)<br />
o Alcohol abstinence. (PC, CS)<br />
o Smoking cessation. (PC, CS)<br />
o Cancer screening. (PC, CS)<br />
o Limiting risks <strong>of</strong> occupational and environmental hazards. (PC, CS)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to healthy patients. (PC, PLI)<br />
Using a cost-effective approach based for screening. (PC, SBP)<br />
Incorporating patient preferences. (PC, P)<br />
Engaging the patient as an active participant in his/her health care. (PC,P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Recognize the importance <strong>of</strong> regularly screening all patients followed and <strong>of</strong> teaching all<br />
patients about preventive measures. (PC, P)<br />
2. Appreciate the necessity <strong>of</strong> keeping detailed records <strong>of</strong> screening and health maintenance<br />
measures. (PC, P)<br />
3. Understand that physicians and health care delivery organizations are frequently judged by<br />
their ability to deliver the highest quality screening and preventive measures. (PLI, P, SBP)<br />
66
4. Recognize the importance <strong>of</strong> addressing community sources <strong>of</strong> health risk. (PC, P)<br />
5. Respond appropriately to patients who are nonadherent preventive measures. (CS, P)<br />
6. Respect the patient’s right to refuse preventive measures and screening. (P)<br />
7. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> screening tests. (PLI, P)<br />
8. Demonstrate ongoing commitment to self-directed learning regarding prevention and<br />
screening. (PLI, P)<br />
9. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in preventative medicine. (P, SBP)<br />
D. RESOURCES:<br />
484.<br />
USPSTF Recommendation: Screening for Breast Cancer<br />
www.ahcpr.gov/clinic/3rduspstf/breastcancer/brcanrr.htm<br />
USPSTF Recommendation: Screening for Cervical Cancer<br />
www.ahrq.gov/clinic/3rduspstf/cervcan/cervcanrr.htm<br />
USPSTF Recommendations Statement: Counseling to prevent tobacco use and tobaccocaused<br />
disease<br />
www.ahrq.gov/clinic/3rduspstf/tobacccoun/tobcounrs.htm<br />
Screening for Prostate Cancer. American College <strong>of</strong> Physicians. Ann Int Med 1997; 126: 480-<br />
Summary <strong>of</strong> Recommendations for Adult Immunization. Immunization Action Coalition Bulletin.<br />
Adapted from the recommendations <strong>of</strong> the Advisory Committee on Immunization Practices<br />
(ACIP), August 2005<br />
www.immunize.org/acip<br />
67
TRAINING PROBLEM #2: ABDOMINAL PAIN<br />
RATIONALE:<br />
Abdominal pain is a common symptom that can be attributed to a wide variety <strong>of</strong> acute and<br />
chronic disease processes, many <strong>of</strong> which may represent serious medical problems. Mastery <strong>of</strong><br />
the approach to patients with abdominal pain is important to third year medical students.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> gastrointestinal and gynecologic anatomy, physiology, and pathophysiology.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Three principal types <strong>of</strong> abdominal pain:<br />
Visceral pain: (MK)<br />
o Poorly localized but site roughly corresponds to dermatome that innervates the affected<br />
organ.<br />
o Characteristics may vary (dull, cramping, burning).<br />
o Frequently accompanied by secondary autonomic effects (nausea, vomiting, pallor,<br />
diaphoresis, restlessness).<br />
o Patient moves around in an attempt to alleviate discomfort.<br />
Somatoparietal or peritoneal pain: (MK)<br />
o More localized and more intense than visceral pain.<br />
o Arises from peritoneal irritation.<br />
o Aggravated by movement (patient attempts to lie still).<br />
Referred pain: (MK)<br />
o Usually well localized but felt in areas remote to affected organ.<br />
o May be felt in skin or in deeper tissues.<br />
o Results from convergence <strong>of</strong> visceral afferent neurons with somatic neurons from<br />
different anatomic regions.<br />
2. Relative likelihood <strong>of</strong> the common causes <strong>of</strong> abdominal pain based on the pain pattern and the<br />
quadrant in which the pain is located. (MK)<br />
3. Diagnostic discrimination between common causes <strong>of</strong> abdominal pain based on history,<br />
physical exam, laboratory testing, and imaging procedures. (MK)<br />
4. Symptoms and signs indicative <strong>of</strong> an acute/surgical abdomen. (MK)<br />
5. The influence <strong>of</strong> age, gender, menopausal status, and immunocompetency on the prevalence<br />
<strong>of</strong> different disease processes that may result in abdominal pain. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
appropriately complete medical history that differentiates among etiologies <strong>of</strong> disease,<br />
including:<br />
• Chronology. (PC, CS)<br />
68
• Location. (PC, CS)<br />
• Radiation. (PC, CS)<br />
• Character. (PC, CS)<br />
• Intensity. (PC, CS)<br />
• Duration. (PC, CS)<br />
• Aggravating or alleviating factors. (PC, CS)<br />
• Associated symptoms. (PC, CS)<br />
• Pertinent information about previous abdominal or pelvic surgeries, chronic medical<br />
conditions, sexual activity, medications, and family history. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a focused physical exam in<br />
patients who present with abdominal pain in order to:<br />
Establish a preliminary diagnosis <strong>of</strong> the cause. (PC)<br />
Assess the severity <strong>of</strong> the patient’s presenting symptoms and signs(PC)<br />
Determine the urgency <strong>of</strong> implementing diagnostic and treatment<br />
plans. (PC)<br />
The initial physical examination <strong>of</strong> the patient should include:<br />
A general assessment <strong>of</strong> the patient’s appearance, position, and degree <strong>of</strong> discomfort.<br />
(PC)<br />
Measurement <strong>of</strong> vital signs, including temperature, pulse, blood pressure, and, when<br />
indicated, orthostatic blood pressure and pulse. (PC)<br />
Correct order and technique for examining the abdomen. (PC)<br />
Inspection <strong>of</strong> the abdomen for surgical scars, distension, asymmetry or cutaneous<br />
abnormalities (dilated veins, ecchymoses, etc.). (PC)<br />
Auscultation <strong>of</strong> the abdomen for abnormal bowel sounds, bruits. (PC)<br />
Percussion <strong>of</strong> the abdomen for detection <strong>of</strong> hepatomegaly, splenomegaly, abdominal<br />
masses, or the presence <strong>of</strong> ascites. (PC)<br />
Palpation <strong>of</strong> the abdomen for areas <strong>of</strong> tenderness, signs <strong>of</strong> peritoneal inflammation,<br />
hepatomegaly, splenomegaly, abnormal masses, pulsations, or hernias. (PC)<br />
Performance <strong>of</strong> rectal and pelvic exams (under supervision). (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
diagnosis <strong>of</strong> the most important and likely causes <strong>of</strong> a patient’s abdominal pain and<br />
recognize specific history, physical exam, and laboratory findings that distinguish<br />
between the following diagnoses or conditions:<br />
Appendicitis. (PC, MK)<br />
Cholecystitis (biliary colic). (PC, MK)<br />
Pancreatitis. (PC, MK)<br />
Diverticulitis. (PC, MK)<br />
Peptic ulcer disease including perforation. (PC, MK)<br />
Gastroenteritis. (PC, MK)<br />
Hepatitis. (PC, MK)<br />
Irritable bowel syndrome. (PC, MK)<br />
Small bowel obstruction. (PC, MK)<br />
Acute mesenteric ischemia. (MK, PC)<br />
Inflammatory bowel disease. (PC, MK)<br />
Ruptured abdominal aortic aneurysm. (PC, MK)<br />
Ureteral stones (renal colic). (PC, MK)<br />
Pelvic inflammatory disease. (PC, MK)<br />
69
Ruptured ectopic pregnancy. (PC, MK)<br />
Abdominal wall pain. (PC, MK)<br />
Referred pain. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to interpret specific diagnostic tests<br />
and procedures that are commonly ordered to evaluate patients who present with<br />
abdominal pain. Test interpretation should take into account:<br />
Important differential diagnostic considerations including potential diagnostic<br />
emergencies. (PC, MK)<br />
Pre-test and post-test likelihood <strong>of</strong> disease (probabilistic reasoning). (PC, MK)<br />
Performance characteristics <strong>of</strong> individual tests (sensitivity, specificity, positive and<br />
negative predictive value, likelihood ratios). (PC, MK)<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
• CBC with differential. (PC, MK)<br />
• UA. (PC, MK)<br />
• Pregnancy test. (PC, MK)<br />
• Stool for occult blood. (PC, MK)<br />
• Hepatic function panel. (PC, MK)<br />
• Amylase and lipase. (PC, MK)<br />
• Abdominal obstructive series. (PC, MK)<br />
Students should be able to define the indications for, and interpret (with<br />
consultation) the results <strong>of</strong>:<br />
Abdominal ultrasound. (PC, MK)<br />
Abdominal CT scan. (PC, MK)<br />
Paracentesis fluid studies. (PC, MK)<br />
Upper gastrointestinal endoscopy. (PC, MK)<br />
Sigmoidoscopy/colonoscopy. (PC, MK)<br />
Barium contrast studies. (PC, MK)<br />
Radionuclide scan <strong>of</strong> the hepatobiliary system. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient<br />
and his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC,<br />
CS)<br />
Communicate in lay terms the indications, risk/benefits, and expected outcomes<br />
essential to obtaining informed consent for diagnostic and therapeutic procedures<br />
commonly used to evaluate and treat patients who present with abdominal pain. (PC,<br />
CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Insert a nasogastric tube. (PC)<br />
Perform stool occult blood testing. (PC)<br />
Assist in performing a paracentesis after explaining the procedure to the patient. (PC,<br />
CS)<br />
7. Management skills: Students should be able to develop an appropriate<br />
evaluation and treatment plan for patients that includes:<br />
Recognizing the role <strong>of</strong> narcotic analgesics and empiric antibiotics in treating selected<br />
patients who present with acute abdominal pain. (PC, MK)<br />
Determining when to consult a gastroenterologist or a surgeon. (PC, SBP)<br />
Involving a surgeon as soon as possible when a patient is identified as having an acute<br />
abdomen. (PC, SBP)<br />
70
Selecting various tests and procedures commonly used to diagnose patients who<br />
present with symptoms <strong>of</strong> abdominal pain. ( PC, MK)<br />
Recommending basic initial management plans for the various causes <strong>of</strong> abdominal<br />
pain listed in the differential diagnosis. (PC, MK)<br />
Considering the potential value <strong>of</strong> addressing psychosocial issues in the management<br />
<strong>of</strong> chronic abdominal pain. (PC, MK)<br />
Accessing and utilizing appropriate information systems and resources to help<br />
delineate issues related to abdominal pain. (PC, PLI)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for abdominal<br />
pain. (PLI, P)<br />
2. Recognize the importance <strong>of</strong> patient needs and preferences when selecting among<br />
diagnostic and therapeutic options for abdominal pain. (P)<br />
3. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essions in the treatment <strong>of</strong> abdominal pain. (P, SBP)<br />
D. REFERENCES:<br />
Silen W. Cope’s Early Diagnosis <strong>of</strong> the Acute Abdomen. 20 th ed. New York: Oxford<br />
<strong>University</strong> Press; 2000.<br />
Wagner JM, McKinney WP, Carpenter JL. The rational clinical exam. Does this patient<br />
have appendicitis? JAMA. 1996;276:1589-94.<br />
Lederle F, Simel D. The rational clinical exam. Does this patient have an abdominal<br />
aortic aneurysm? JAMA. 1999;281:77-82.<br />
Trowbridge RL, Rutkowski NK, Shojania KG. The rational clinical exam. Does this<br />
patient have acute cholecystitis? JAMA. 2003;289: 80-86.<br />
71
TRAINING PROBLEM #3: ALTERED MENTAL STATUS<br />
RATIONALE:<br />
The diagnosis and management <strong>of</strong> altered mental status requires a working knowledge <strong>of</strong> all areas <strong>of</strong><br />
internal medicine, so varied are the etiologies and corresponding treatment strategies. Internists must<br />
master an approach to the problem as they are <strong>of</strong>ten the first physicians to see such patients.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Basic course work in physiology, pathophysiology, and neuroanatomy.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The differentiation <strong>of</strong> delirium, dementia, and depression. (MK)<br />
2. The pathophysiology, symptoms, and signs <strong>of</strong> the most common and most serious causes <strong>of</strong><br />
altered mental status, including:<br />
Metabolic causes (e.g. hyper/hyponatremia, hyper/hypoglycemia, hypercalcemia,<br />
hyper/hypothyroidism, hypoxia/hypercapnea, B12 deficiency, hepatic encephalopathy,<br />
uremic encephalopathy, drug/alcohol intoxication/withdrawal, and Wernicke’s<br />
encephalopathy). (MK)<br />
Structural lesions (e.g. primary or metastatic tumor, intracranial hemorrhage, subdural<br />
hematoma). (MK)<br />
Vascular (e.g. cerebrovascular accident, transient ischemic attack, cerebral vasculitis).<br />
(MK)<br />
Infectious etiologies (e.g. encephalitis, meningitis, urosepsis, endocarditis, pneumonia,<br />
cellulites). (MK)<br />
Seizures/ post-ictal state. (MK)<br />
Hypertensive encephalopathy. (MK)<br />
Low perfusion states (e.g. arrhythmias, MI, shock, acute blood loss, severe dehydration).<br />
(MK)<br />
Miscellaneous causes (e.g. fecal impaction, postoperative state, sleep deprivation, urinary<br />
retention). (MK)<br />
3. The importance <strong>of</strong> thoroughly reviewing prescription medications over-thecounter drugs, and<br />
supplements and inquiring about substance abuse. (MK)<br />
4. The risk factors for developing altered mental status, including:<br />
Dementia. (MK)<br />
Advanced age. (MK)<br />
Substance abuse. (MK)<br />
Comorbid physical problems such as sleep deprivation, immobility, dehydration, pain, and<br />
sensory impairment. (MK)<br />
ICU admission. (MK)<br />
5. The diagnostic evaluation <strong>of</strong> altered mental status. (MK)<br />
6. Indications, contraindications, and complications <strong>of</strong> lumbar puncture. (MK)<br />
72
7. Principles <strong>of</strong> management <strong>of</strong> the common causes <strong>of</strong> altered mental status. (MK)<br />
8. Nonpharmacologic measures to reduce agitation and aggression, including:<br />
Avoiding the use <strong>of</strong> physical restraints whenever possible. (MK)<br />
Using reorientation techniques. (MK)<br />
Assuring the patient has their devices to correct sensory deficits. (MK)<br />
Promoting normal sleep and day/night awareness. (MK)<br />
Preventing dehydration and electrolyte disturbances. (MK)<br />
Avoiding medications which may worsen delirium whenever possible<br />
(e.g. anticholinergics, benzodiazepines, etc.). (MK)<br />
9. The risks <strong>of</strong> using physical restraints. (MK)<br />
10. The risk and benefits <strong>of</strong> using low-dose high potency antipsychotics for delirium associated<br />
agitation and aggression. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1 History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> altered mental status including<br />
eliciting appropriate information from patients and their families regarding the onset, progression,<br />
associated symptoms, and level <strong>of</strong> physical and mental disability. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Complete neurologic examination. (PC)<br />
Mental status examination. (PC)<br />
Fundoscopic examination. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology for<br />
altered mental status. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
CBC with differential. (PC, MK)<br />
Electrolytes, BUN/Cr, GLC, hepatic function panel, Ca. (PC, MK)<br />
ABG. (PC, MK)<br />
Toxicology screen. (PC, MK)<br />
VDRL. (PC, MK)<br />
Vitamin B12 and thiamine measurements. (PC, MK)<br />
Thyroid function tests. (PC, MK)<br />
Urinalysis and urine culture. (PC, MK)<br />
Blood cultures. (PC, MK)<br />
Cerebrospinal fluid analysis (color, opening pressure, chemistries, cell<br />
counts, staining, cultures, cytology, cryptococcal antigen, VDRL). (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation)<br />
the results <strong>of</strong>:<br />
Cranial CT. (PC, MK)<br />
Cranial MRI. (PC, MK)<br />
Electroencephalogram. (PC, MK)<br />
73
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
When the patient is unable to communicate, obtain a history from a collateral source such<br />
as a family member or other health care proxy. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Obtain an ABG. (PC)<br />
Assist in performing a lumbar puncture after explaining the procedure to the patient. (PC,<br />
CS)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Recognizing that altered mental status in a older inpatient is a medical<br />
emergency and requires that the patient be evaluated immediately. (PC, MK)<br />
Writing appropriate fluid and replacement orders for patients with common electrolyte and<br />
metabolic disturbances. (PC, MK)<br />
Writing appropriate antibiotic orders for the treatment <strong>of</strong> common infectious etiologies. (PC,<br />
MK)<br />
Ordering appropriate nonpharmacologic and pharmacologic interventions for patients with<br />
acute altered mental status with accompanying agitation and aggression. (PC, MK)<br />
Determining when to obtain consultation from a neurologist or neurosurgeon. (PC, SBP)<br />
Utilizing hospital and community resources for patients with permanent or disabling<br />
conditions to help assist their transfer back to the community or rehabilitation facility. (PC,<br />
SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to altered mental status. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Appreciate the family’s concern and at times despair arising from a loved one’s<br />
development <strong>of</strong> altered mental status. (CS, P)<br />
2. Appreciate the patient’s distress and emotional response to that may accompany<br />
circumstances <strong>of</strong> altered mental status. (CS,P)<br />
3. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for altered mental<br />
status. (PLI, P)<br />
4. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic<br />
and therapeutic options for altered mental status. (P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding altered mental<br />
status. (PLI, P)<br />
6. Appreciate the impact altered mental status has on a patient’s quality <strong>of</strong> life, wellbeing,<br />
ability to work, and the family. (P)<br />
7. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong><br />
other healthcare pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> altered mental status. (P,<br />
SBP)<br />
D. REFERENCES:<br />
74
Ropper AH. (2005). Acute confusional states and coma. In Kasper DL, Braunwald EB,<br />
Fauci AS, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>.<br />
16 th ed. New York, NY: McGraw-Hill; 2005:1624-31.<br />
Gleason OC. Delirium. Am Fam Physician. 2003;67:1027-34.<br />
Brown TM, Boyle MF. Delirium. BMJ. 2002;325:644-7.<br />
Meagher DJ. Delirium: optimizing management. BMJ. 2001;322:144-9.<br />
75
TRAINING PROBLEM #4: ANEMIA<br />
RATIONALE:<br />
Anemia is a common finding, <strong>of</strong>ten identified incidentally in asymptomatic patients. It can be a<br />
manifestation <strong>of</strong> a serious underlying disease. Distinguishing among the many disorders that cause<br />
anemia, not all <strong>of</strong> which require treatment, is an important training problem for third year medical<br />
students.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should<br />
include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> pathogenesis and pathophysiology <strong>of</strong> anemia.<br />
Knowledge <strong>of</strong> the basic biochemistry and pathophysiology <strong>of</strong> the blood and bone marrow.<br />
Knowledge <strong>of</strong> the pharmacology <strong>of</strong> medications that can cause anemia as well as those used<br />
to treat it.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Classification <strong>of</strong> anemia based on red cell size:<br />
Microcytic:<br />
o Iron deficiency. (MK)<br />
o Thalassemic disorders. (MK)<br />
o Sideroblastic anemia. (MK)<br />
Normocytic:<br />
o Acute blood loss. (MK)<br />
o Hemolysis. (MK)<br />
o Anemia <strong>of</strong> chronic disease (e.g. infection, inflammation, malignancy). (MK)<br />
o Chronic renal insufficiency/erythropoietin deficiency. (MK)<br />
o Bone marrow suppression (e.g. bone marrow invasion, aplastic anemia).<br />
o Hypothyroidism. (MK)<br />
o Testosterone deficiency. (MK)<br />
o Early presentation <strong>of</strong> microcytic or macrocytic anemia (e.g. early iron deficiency<br />
anemia). (MK)<br />
o Combined presentation <strong>of</strong> microcytic and macrocytic anemias. (MK)<br />
Macrocytic:<br />
o Ethanol abuse. (MK)<br />
o B12 deficiency. (MK)<br />
o Folate deficiency. (MK)<br />
o Drug-induced. (MK)<br />
o Reticulcytosis. (MK)<br />
o Liver disease. (MK)<br />
o Myelodysplastic syndromes. (MK)<br />
o Hypothyroidism. (MK)<br />
10. Morphological characteristics, pathophysiology, and relative prevalence <strong>of</strong> each <strong>of</strong> the causes<br />
<strong>of</strong> anemia. (MK)<br />
76
11. The meaning and utility <strong>of</strong> various components <strong>of</strong> the hemogram (e.g. hemoglobin, hematocrit,<br />
mean corpuscular volume, and random distribution width). (MK)<br />
12. The classification <strong>of</strong> anemia into hypoproliferative and hyperproliferative categories and the<br />
utility <strong>of</strong> the reticulocyte count/index. (MK)<br />
13. The potential usefulness <strong>of</strong> the white blood cell count and red blood cell count when attempting<br />
to determine the cause <strong>of</strong> anemia. (MK)<br />
14. The diagnostic utility <strong>of</strong> the various tests for iron deficiency (e.g. serum iron, total iron binding<br />
capacity, transferrin saturation, ferritin). (MK)<br />
15. The genetic basis <strong>of</strong> some forms <strong>of</strong> anemia. (MK)<br />
16. Indications, contraindications, and complications <strong>of</strong> blood transfusion. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history, that differentiates among etiologies <strong>of</strong> disease, including:<br />
Constitutional and systemic symptoms (e.g. fatigue, weight loss). (PC, CS)<br />
History <strong>of</strong> gastrointestinal bleeding or risk factors for it. (PC, CS)<br />
Abdominal pain. (PC, CS)<br />
Prior history <strong>of</strong> anemia or other blood diseases. (PC, CS)<br />
Medications. (PC, CS)<br />
Diet. (PC, CS)<br />
Alcohol use. (PC, CS)<br />
Menstrual history. (PC, CS)<br />
Family history <strong>of</strong> anemia or other blood diseases. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Pallor (e.g. palms, conjunctiva, nail beds). (PC)<br />
Mouth (e.g. glossitis, cheilosis). (PC)<br />
Hyperdynamic precordium, systolic flow murmur. (PC)<br />
Lymph nodes. (PC)<br />
spleen. (PC)<br />
Obtain stool for occult blood testing. (PC)<br />
Nervous system. (PC)<br />
3. Differential diagnosis: Students should be able to generate a list <strong>of</strong> the most important and<br />
most common causes <strong>of</strong> anemia, recognizing specific history, physical exam, and laboratory<br />
findings that suggest a specific etiology. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
Hemoglobin and hematocrit. (PC, MK)<br />
Red cell indices (e.g. mean corpuscular volume and random distribution width). (PC, MK)<br />
White blood cell and platelet count. (PC, MK)<br />
Reticulocyte count. (PC, MK)<br />
Iron studies (serum iron, TIBC, ferritin, transferrin). (PC, MK)<br />
Serum B12 and folate. (PC, MK)<br />
Haptoglobin. (PC, MK)<br />
77
Lactic dehydrogenase. (LDH) (PC, MK)<br />
Hemoglobin electrophoresis. (PC, MK)<br />
Blood smear. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) results<br />
<strong>of</strong>:<br />
Bone marrow biopsy. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient about the management plan. (PC, CS)<br />
Counsel with regard to (a) possible causes, (b) appropriate further evaluation to establish<br />
the diagnosis <strong>of</strong> an underlying disease, and (c) the impact on the family (genetic<br />
counseling). (PC, CS)<br />
6. Basic procedural skills: Students should be able to perform and interpret:<br />
Stool occult blood testing. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Evaluating for underlying disease processes, given that anemia is not a disease per se, but<br />
rather a common finding that requires further delineation in order to identify the underlying<br />
cause. (PC, MK)<br />
Prescribing indicated replacement therapy, including iron, vitamin B12, and folic acid. (PC,<br />
MK)<br />
Determining when to obtain consultation from a hematologist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to anemia. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1 Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for anemia. (PLI, P)<br />
2 Respond appropriately to patients who are non-adherent to treatment for anemia. (CS, P)<br />
3 Demonstrate ongoing commitment to self-directed learning regarding anemia. (PLI, P)<br />
Appreciate the impact anemia has on a patient’s quality <strong>of</strong> life, well-being, ability to work, and<br />
the family. (P)<br />
4 Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essions in the treatment <strong>of</strong> anemia. (P, SBP)<br />
D. REFERENCES:<br />
Sheth TN. Choudhry NK. Bowes M. Detsky AS. The relation <strong>of</strong> conjunctival pallor to the<br />
presence <strong>of</strong> anemia. J Gen Intern Med. 1997;12:102-6.<br />
Guyatt, G H. Oxman, A D. Ali, M. Willan, A. McIlroy, W. Patterson, C. Laboratory<br />
diagnosis <strong>of</strong> iron-deficiency anemia: an overview. J Gen Intern Med. 1992;7:145-53.<br />
Kis AM. Carnes M. Detecting iron deficiency in anemic patients with concomitant<br />
medical problems. J Gen Intern Med. 1998; 13:455-61.<br />
Bain BJ. Diagnosis from the blood smear. N Engl Journal Med. 2005;353:498-507.<br />
Weiss G. Goodnough LT. Anemia <strong>of</strong> chronic disease. N Engl J Med. 2005;352:1011-23.<br />
78
H<strong>of</strong>fbrand V. Provan D. ABC <strong>of</strong> clinical haematology: macrocytic anaemias. BMJ.<br />
1997;314:430-3.<br />
79
TRAINING PROBLEM #5: BACK PAIN<br />
RATIONALE:<br />
Back pain is one <strong>of</strong> the most commonly encountered problems in the outpatient, primary care internal<br />
medicine setting. It has an important differential diagnosis, and the initial decision-making must be<br />
made on the basis <strong>of</strong> clinical findings. As such, it is an excellent training condition for teaching<br />
decision-making based on careful collection and interpretation <strong>of</strong> basic clinical data. There is<br />
emerging data on test utility, especially as regards expensive spinal imaging, which facilitates<br />
teaching rational, cost-effective test ordering. Moreover, its requirement for skillful management,<br />
patient education, and support facilitate the teaching <strong>of</strong> these competencies.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy and physiology <strong>of</strong> bony, s<strong>of</strong>t tissue, vascular, and <strong>of</strong> the spine.<br />
Pathogenesis and pathophysiology <strong>of</strong> muscular strain, osteoarthritis, spinal stenosis,<br />
osteoporosis, disc degeneration, and spinal metastases.<br />
Pharmacology <strong>of</strong> non-narcotic and narcotic analgesics, nonsteroidal anti-inflammatory drugs,<br />
muscle “relaxants.”<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The symptoms, signs, and typical clinical course <strong>of</strong> the various causes <strong>of</strong> back pain including:<br />
Ligamentous/muscle strain (nonspecific musculoskeletal back pain). (MK)<br />
Degenerative arthritis (spondylosis). (MK)<br />
Disc herniation. (MK)<br />
Spinal stenosis. (MK)<br />
Vertebral compression fracture. (MK)<br />
Traumatic fracture. (MK)<br />
Sacroileitis. (MK)<br />
Spinal metastases. (MK)<br />
Spinal epidural abscess. (MK)<br />
Cauda equina syndrome. (MK)<br />
2. The role <strong>of</strong> diagnostic studies in the evaluation <strong>of</strong> the back pain there indications,<br />
limitations, cost:<br />
Plain radiography. (MK)<br />
CT. (MK)<br />
MRI. (MK)<br />
Myelogram. (MK)<br />
Electrodiagnosis (i.e. electromyography and nerve conduction studies). (MK)<br />
Bone densitometry. (MK)<br />
3. Response to therapy <strong>of</strong> the various etiologies, with understanding <strong>of</strong> the roles <strong>of</strong>:<br />
80
Bed rest. (MK)<br />
Exercise. (MK)<br />
Analgesia. (MK)<br />
NSAIDs. (MK)<br />
Heat/ice. (MK)<br />
Ultrasound. (MK)<br />
Spinal manipulation. (MK)<br />
Surgical interventions. (MK)<br />
4. Risk factor for and means <strong>of</strong> limiting disability and chronicity. (MK)<br />
5. Fear avoidance behaviors. (MK)<br />
6. Pain related behaviors with regard to chronic narcotic use. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, that differentiates among etiologies <strong>of</strong> disease,<br />
including:<br />
Cancer history. (PC, CS)<br />
Weight loss. (PC, CS)<br />
Fever. (PC, CS)<br />
Recent infection. (PC, CS)<br />
Intravenous drug use. (PC, CS)<br />
Steroid use. (PC, CS)<br />
Trauma. (PC, CS)<br />
Rapidly progressive focal numbness and/or weakness. (PC, CS)<br />
Bowel/bladder dysfunction. (PC, CS)<br />
Saddle anesthesia. (PC, CS)<br />
Symptoms <strong>of</strong> systemic rheumatologic conditions. (PC, CS)<br />
Anatomic abnormalities (e.g. kyphosis, scoliosis). (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Examination <strong>of</strong> the spine. (PC)<br />
Neurologic examination <strong>of</strong> the lower extremities. (PC)<br />
Straight leg raising test. (PC)<br />
Testing for saddle anesthesia. (PC)<br />
Assessment <strong>of</strong> rectal tone. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology for back<br />
pain (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
ESR. (PC, MK)<br />
CBC. (PC, MK)<br />
Serum Alk Phos. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
81
esults <strong>of</strong>:<br />
Plain spinal radiography. (PC, MK)<br />
Spinal CT. (PC, MK)<br />
Spinal MRI. (PC, MK)<br />
Radionuclide bone scan. (PC, MK)<br />
Bone densitometry. (PC, MK)<br />
Electrodiagnostic tests. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Explain the importance <strong>of</strong> active participation in the treatment plan. (PC, CS)<br />
Elicit questions from the patient and their family about the management plan.<br />
(PC, CS)<br />
6. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Patient education about the typical course <strong>of</strong> back pain. (PC, MK)<br />
Methods to prevent the development <strong>of</strong> chronic back pain. (PC, MK)<br />
Proper use <strong>of</strong> analgesics, NSAIDs, muscle relaxants, and local heat/ice. (PC, MK)<br />
Teaching back hygiene measures, exercises, and proper lifting and standing ergonomics.<br />
(PC, MK)<br />
Counseling patients about lifestyle modifications including weight loss. (PC, MK)<br />
The potential role <strong>of</strong> chiropractic, acupuncture, and massage (PC, MK)<br />
Determining when to obtain consultation from an appropriate back pain specialist. (PC,<br />
SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to back pain. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1 Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for back pain. (PLI, P)<br />
2 Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for back pain. (P)<br />
3 Appreciate the importance <strong>of</strong> active patient involvement in the treatment <strong>of</strong> back pain. (P)<br />
4 respond appropriately to patients who are nonadherent to treatment for back pain. (CS, P)<br />
5 respond appropriately to patients with chronic back pain (P)<br />
6 Demonstrate ongoing commitment to self-directed learning regarding back pain. (PLI, P)<br />
7 Appreciate the impact back pain has on a patient’s quality <strong>of</strong> life, well-being, ability to work,<br />
and the family. (P)<br />
8 Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essionals in the treatment <strong>of</strong> back pain. (P, SBP)<br />
D. REFERENCES:<br />
Carragee EJ. Persistent low back pain. N Engl J Med. 2005;352:1891-8.<br />
Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344:363-70.<br />
Atlas SJ, Deyo RA. Evaluating and managing acute low back pain in the primary care<br />
82
setting. J Gen Intern Med. 2001;16:120-31.<br />
Deyo RA. Diagnostic evaluation <strong>of</strong> LBP: reaching a specific diagnosis is <strong>of</strong>ten<br />
impossible. Arch Intern Med. 2002;162:1444-7; discussion 1447-8.<br />
83
TRAINING PROBLEM #6: CHEST PAIN<br />
RATIONALE:<br />
Chest pain is a common and important presenting symptom for a variety <strong>of</strong> disorders, some <strong>of</strong> which<br />
may be life-threatening emergencies. The ability to distinguish chest pain caused by an acute<br />
coronary syndrome (unstable angina or acute myocardial infarction) from other cardiac,<br />
gastrointestinal, pulmonary, musculoskeletal or psychogenic etiologies is an important training<br />
problem for third-year medical students.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate appropriately with patients <strong>of</strong> diverse backgrounds, including the elderly<br />
patient.<br />
Knowledge <strong>of</strong> the anatomy <strong>of</strong> the heart, chest and abdomen.<br />
Understanding <strong>of</strong> the epidemiology <strong>of</strong> heart disease.<br />
Knowledge <strong>of</strong> the pathogenesis and pathophysiology <strong>of</strong> cardiovascular disease.<br />
Knowledge <strong>of</strong> the pharmacology <strong>of</strong> cardiovascular drugs.<br />
Ability to perform a cardiovascular risk assessment and understand issues related to primary<br />
and secondary prevention <strong>of</strong> cardiovascular disease.<br />
Ability to understand the impact <strong>of</strong> illness on individuals and their families.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe and discuss:<br />
1 Symptoms and signs <strong>of</strong> chest pain that may be due to an acute coronary syndrome such as<br />
unstable angina or acute myocardial infarction. (MK)<br />
2 Symptoms and signs <strong>of</strong> chest pain that are characteristic <strong>of</strong> angina pectoris. (MK)<br />
3 Symptoms and signs <strong>of</strong> chest pain due to other cardiac causes such as:<br />
Atypical or variant angina (coronary vasospasm, Prinzmetal angina). (MK)<br />
Cocaine-induced chest pain. (MK)<br />
Pericarditis. (MK)<br />
Aortic dissection. (MK)<br />
Valvular heart disease (aortic stenosis, mitral valve prolapse). (MK)<br />
Non-ischemic cardiomyopathy. (MK)<br />
Syndrome X. (MK)<br />
4. Symptoms and signs <strong>of</strong> chest pain due to gastrointestinal disorders such as:<br />
Esophageal disease (GERD, esophagitis, esophageal dysmotility). (MK)<br />
Biliary disease (cholecystitis, cholangitis). (MK)<br />
Peptic ulcer disease. (MK)<br />
Pancreatitis. (MK)<br />
5. Symptoms and signs <strong>of</strong> chest pain due to pulmonary disorders such as:<br />
Pneumonia. (MK)<br />
Spontaneous pneumothorax. (MK)<br />
Pleurisy. (MK)<br />
Pulmonary embolism. (MK)<br />
84
Pulmonary hypertension/cor pulmonale. (MK)<br />
6. Symptoms and signs <strong>of</strong> chest pain due to musculoskeletal causes such as:<br />
Costochondritis. (MK)<br />
Rib fracture. (MK)<br />
My<strong>of</strong>ascial pain syndromes. (MK)<br />
Muscular strain. (MK)<br />
Herpes zoster. (MK)<br />
7. Symptoms and signs <strong>of</strong> chest pain due to psychogenic causes such as:<br />
Panic disorders. (MK)<br />
Hyperventilation. (MK)<br />
Somat<strong>of</strong>orm disorders. (MK)<br />
8. Factors that may be responsible for provoking or exacerbating symptoms <strong>of</strong> ischemic chest<br />
pain by:<br />
Increasing myocardial oxygen demand.<br />
o Tachycardia or tachyarrhythmia. (MK)<br />
o Hypertension. (MK)<br />
o Increased wall stress (aortic stenosis, cardiomyopathy). (MK)<br />
o Hyperthyroidism. (MK)<br />
Decreasing myocardial oxygen supply.<br />
o Anemia. (MK)<br />
o Hypoxemia. (MK)<br />
9. Risk factors for the development <strong>of</strong> coronary heart disease:<br />
Age and gender. (MK)<br />
Family history <strong>of</strong> sudden death or premature CAD. (MK)<br />
Personal history <strong>of</strong> peripheral vascular or cerebrovascular disease. (MK)<br />
Smoking. (MK)<br />
Lipid abnormalities (includes dietary history <strong>of</strong> saturated fat and cholesterol). (MK)<br />
Diabetes mellitus. (MK)<br />
Hypertension. (MK)<br />
Obesity. (MK)<br />
Sedentary lifestyle. (MK)<br />
Cocaine use. (MK)<br />
Estrogen use. (MK)<br />
Chronic inflammation. (MK)<br />
10. Physiologic basis and/or scientific evidence supporting each type <strong>of</strong> treatment, intervention or<br />
procedure commonly used in the management <strong>of</strong> patients who present with chest pain. (MK)<br />
11. Role <strong>of</strong> a critical pathway or practice guideline in delivering high quality, cost-effective care for<br />
patients presenting with symptoms <strong>of</strong> chest pain in the outpatient clinic, emergency room or<br />
hospital. (MK, PC, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
appropriately complete medical history that differentiates among the common etiologies <strong>of</strong><br />
chest pain.<br />
85
The initial medical history should allow students to categorize the patients’ symptoms as<br />
angina pectoris, atypical angina or non-cardiac chest pain. (PC, CS)<br />
Specifically, the medical history <strong>of</strong> a patient with chest pain should contain information<br />
about those clinical characteristics that are typical <strong>of</strong> angina pectoris:<br />
o Substernal location. (PC, CS)<br />
o Precipitated by exertion. (PC, CS)<br />
o Relieved by rest or nitroglycerin. (PC, CS)<br />
o Onset, duration, severity, radiation, presence or absence <strong>of</strong> associated symptoms (such<br />
as dyspnea, diaphoresis or lightheadedness). (PC, CS)<br />
The history <strong>of</strong> a patient with chest pain should also contain information about:<br />
o Risk factors for coronary heart disease. (PC, CS)<br />
o Previous history <strong>of</strong> ischemic heart disease or valvular heart disease (rheumatic fever,<br />
cardiac murmurs). (PC, CS)<br />
o Previous history <strong>of</strong> peripheral vascular disease or cerebrovascular disease. (PC, CS)<br />
Students should be able to use the medical history to assess the<br />
functional status <strong>of</strong> patients who present with ischemic chest pain. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a focused physical exam that<br />
includes the following elements:<br />
Accurate measurement <strong>of</strong> arterial blood pressure and recognition <strong>of</strong> the typical blood<br />
pressure findings that occur in patients with aortic stenosis, aortic insufficiency, and pulsus<br />
paradoxus. (PC)<br />
Assessment <strong>of</strong> major arterial pulses for abnormalities, including bruits. (PC)<br />
Assessment <strong>of</strong> the neck veins for jugular venous distention and, when necessary,<br />
evaluation for abdominal jugular reflux. (PC)<br />
Assessment <strong>of</strong> the conjunctiva and optic fundus. (PC)<br />
Assessment <strong>of</strong> the extremities to ascertain skin condition, including color, temperature and<br />
the presence <strong>of</strong> edema, xanthomas, cyanosis and clubbing. (PC)<br />
Assessment <strong>of</strong> the lungs for crackles, rhonchi, rubs and decreased breath sounds. (PC)<br />
Inspection and palpation <strong>of</strong> the anterior chest to identify right and left sided heaves, lifts,<br />
and thrills. (PC)<br />
Auscultation <strong>of</strong> the heart to determine rhythm, intensity <strong>of</strong> heart sounds, splitting <strong>of</strong> S2 and<br />
the presence <strong>of</strong> rubs, gallops (S3, S4, summation) or extra heart sounds (e.g. clicks). (PC)<br />
Auscultation <strong>of</strong> the heart to detect the presence <strong>of</strong> heart murmurs. When a heart murmur is<br />
present, students should be able to:<br />
o Identify timing (systolic vs. diastolic, holosystolic vs. ejection). (PC)<br />
o Describe pitch, location and pattern <strong>of</strong> radiation. (PC)<br />
o Gauge significance (innocent vs. pathologic, sclerosis vs. stenosis). (PC)<br />
Assessment <strong>of</strong> the abdomen to determine the presence <strong>of</strong> epigastric or right<br />
upper quadrant tenderness, hepatomegaly, abnormal pulsations or bruits. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
and recognize specific history, physical exam, and laboratory findings that suggest a diagnosis<br />
<strong>of</strong> myocardial ischemia rather than a non-ischemic cause <strong>of</strong> chest pain (GI, pulmonary,<br />
musculoskeletal, psychogenic or undetermined). (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Test interpretation should take into account:<br />
Important differential diagnostic considerations including the “must not miss” diagnoses.<br />
(PC, MK)<br />
86
Pre-test and post-test likelihood <strong>of</strong> disease (probabilistic reasoning). (PC, MK)<br />
Performance characteristics <strong>of</strong> individual tests (sensitivity, specificity,<br />
positive and negative predictive value, likelihood ratios). (PC, MK)<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Cardiac biomarkers indicative <strong>of</strong> myocardial necrosis. (PC, MK)<br />
12-lead ECG. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
ABG. (PC, MK)<br />
Students should be able to define the indications for, and interpret (with consultation) the<br />
results <strong>of</strong> the following diagnostic tests and procedures:<br />
Echocardiogram (transthoracic and transesophageal). (PC, MK)<br />
Exercise stress test. (PC, MK)<br />
Stress thallium (myocardial perfusion scan). (PC, MK)<br />
Dobutamine stress echocardiography. (PC, MK)<br />
Coronary angiography. (PC, MK)<br />
Electron beam CT scan (for coronary calcification). (PC, MK)<br />
Ventilation/perfusion lung (V/Q) scan. (PC, MK)<br />
Pulmonary embolism protocol CT scan. (PC, MK)<br />
Pulmonary angiography. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, prognosis and treatment plan to patients and their families.<br />
(PC, CS)<br />
As appropriate for age and gender, educate patients about risk factors for cardiovascular<br />
disease. (PC, CS)<br />
Counsel patients or facilitate the provision <strong>of</strong> counseling related to:<br />
o<br />
Smoking cessation. (PC, CS)<br />
o<br />
Reduction <strong>of</strong> dietary saturated fats and cholesterol. (PC, CS)<br />
o<br />
Restriction <strong>of</strong> dietary sodium intake. (PC, CS)<br />
o<br />
Weight reduction. (PC, CS)<br />
o<br />
Increased physical activity. (PC, CS)<br />
6. Basic procedural skills: Students should be able to:<br />
• Perform a 12-lead ECG. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Identification <strong>of</strong> the indications, contraindications, mechanisms <strong>of</strong> action, adverse reactions,<br />
significant interactions, and relative costs <strong>of</strong> the following medications:<br />
o Anti-platelet agents (aspirin, clopidogrel). (PC, MK)<br />
o Nitroglycerin and long-acting nitrates. (PC, MK)<br />
o Beta-blockers. (PC, MK)<br />
o Angiotensin-converting enzyme inhibitors. (PC, MK)<br />
o Calcium channel blockers. (PC, MK)<br />
o Antithrombotic therapy (heparin, warfarin). (PC, MK)<br />
o Glycoprotein IIb/IIIa inhibitors. (PC, MK)<br />
o Lipid-lowering agents. (PC, MK)<br />
Identification <strong>of</strong> the indications, contraindications, complications, long-term outcomes and<br />
relative costs associated with the following treatment modalities for ischemic heart disease:<br />
o Thrombolytic therapy. (PC, MK)<br />
o Percutaneous coronary intervention (with or without stenting). (PC, MK)<br />
o Coronary artery bypass graft surgery (CABG). (PC, MK)<br />
87
Determining when to consult a cardiologist or other subspecialist in the management <strong>of</strong><br />
patients with chest pain. (PC, SBP)<br />
Description <strong>of</strong> how the diagnosis and treatment <strong>of</strong> chest pain in special populations may<br />
differ (e.g. very elderly, associated co-morbidities). (PC, MK)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to chest pain. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Understand the emotional impact <strong>of</strong> a diagnosis <strong>of</strong> coronary artery disease and its potential<br />
effect on lifestyle (work performance, sexual functioning, etc). (PC, P)<br />
2. Respond appropriately to patient who are nonadherent to lifestyle modifications.<br />
(CS, P)<br />
3. Recognize the importance <strong>of</strong> early detection and modification <strong>of</strong> risk factors that may<br />
contribute to the development <strong>of</strong> atherosclerosis. (PC, P)<br />
4. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for chest pain. (PLI,<br />
P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding chest pain. (PLI, P)<br />
6. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> chest pain. (P, SBP)<br />
D. REFERENCES:<br />
ACC/AHA 2002 guideline update for the management <strong>of</strong> patients with chronic stable<br />
angina--summary article: a report <strong>of</strong> the American College <strong>of</strong> Cardiology/American<br />
Heart Association Task Force on practice guidelines (Committee on the Management<br />
<strong>of</strong> Patients With Chronic Stable Angina). J Am Coll Cardiol. 2003;41:159-68.<br />
http://www.acc.org/clinical/guidelines/stable/stable_clean.pdf<br />
Panju AA, Hemmeigarn BR, Guyatt GH, Simel DL. Is this patient having a myocardial<br />
infarction? JAMA. 1998;280:1256-63.<br />
Klompas M. Does this patient have an acute thoracic aortic dissection? JAMA.<br />
2002;287:2262-72.<br />
TRAINING PROBLEM #7: COUGH<br />
RATIONALE:<br />
Cough is one <strong>of</strong> the most common symptoms with which a patient will present in the outpatient<br />
setting. There are several common etiologies for cough <strong>of</strong> which a third year medical student<br />
should be aware, as well as more clinically concerning etiologies. A proper understanding <strong>of</strong> the<br />
pathophysiology, diagnosis, and treatment <strong>of</strong> cough is an important learning objective.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
88
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> respiratory anatomy, physiology and pathophysiology.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe and discuss:<br />
1. The criteria used to classify a cough (e.g. acute vs. chronic, productive vs. non-productive).<br />
(MK)<br />
2. Symptoms, signs, pathophysiology, differential diagnosis, and typical clinical course <strong>of</strong> the<br />
most common causes cough:<br />
Acute cough:<br />
o<br />
Viral tracheitis. (MK)<br />
o<br />
o<br />
Acute bronchitis. (MK)<br />
Pneumonia. (MK)<br />
Chronic cough:<br />
o Gastroesophageal reflux. (MK)<br />
o Post-nasal drip. (MK)<br />
o Asthma/reactive airways disease. (MK)<br />
o Angiotensin converting enzyme inhibitors. (MK)<br />
o Post-infectious. (MK)<br />
o Infectious (pertussis, tuberculosis). (MK)<br />
o Chronic bronchitis. (MK)<br />
o Bronchiectasis. (MK)<br />
o Pleural effusion. (MK)<br />
o Lung cancer. (MK)<br />
o Congestive heart failure. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among the etiologies <strong>of</strong> disease, including:<br />
Onset. (PC, CS)<br />
Duration. (PC, CS)<br />
Exacerbating/relieving factors. (PC, CS)<br />
Associated symptoms (fever, chills, weight loss). (PC, CS)<br />
Presence or absence <strong>of</strong> hemoptysis. (PC, CS)<br />
Tobacco history. (PC, CS)<br />
Relevant past medical history. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Accurately determining respiratory rate and level <strong>of</strong> respiratory distress. (PC)<br />
Recognizing the pharyngeal signs <strong>of</strong> post nasal drip. (PC)<br />
Identifying rales, rhonchi, and wheezes. (PC)<br />
Recognizing signs <strong>of</strong> pulmonary consolidation. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritorized differential<br />
diagnosis recognizing history, physical exam, and laboratory findings that suggest a specific<br />
etiology <strong>of</strong> cough. (PC, MK)<br />
4. Laboratory interpretations: Students should be able to recommend when to order diagnostic<br />
89
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
Chest radiograph. (PC, MK)<br />
Pleural fluid cell count and chemistries. (PC, MK)<br />
PFTs. (PC, MK)<br />
Sputum Gram stain and sputum acid-fast stain. (PC, MK)<br />
Sputum culture and sensitivities. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) results<br />
<strong>of</strong>:<br />
Barium swallow. (PC, MK)<br />
Upper endoscopy. (PC, MK)<br />
Sputum cytology. (PC, MK)<br />
Chest CT scan. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Counsel and educate patients about environmental contributors to their disease,<br />
pneumococcal and influenza immunizations, and smoking cessation. (PC, CS)<br />
Communicate the diagnosis, prognosis, and treatment plan, and subsequent follow-up to<br />
the patient and his or her family. (PC, CS)<br />
Elicit input and questions from the patient and his or her family about the management<br />
plan. (PC, CS)<br />
6. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Describing the indications, contraindications, mechanisms <strong>of</strong> action, adverse reactions,<br />
significant interactions, and relative costs <strong>of</strong> the various treatments, interventions, or<br />
procedures commonly used to diagnose and treat patients who present with symptoms <strong>of</strong><br />
cough. (PC, MK, SBP)<br />
Determining when to obtain consultation from a pulmonologist, allergist, otolaryngologist, or<br />
gastroenterologist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to patients with chronic cough. (PC, PLI)<br />
Incorporating patient needs and preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for cough. (PLI, P)<br />
2. Respond appropriately to patients who are non-adherent to treatment for cough and smoking<br />
cessation. (CS, P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding diagnosis and<br />
management <strong>of</strong> cough. (PLI, P)<br />
4. Appreciate the impact that an acute or chronic cough has on a patient’s quality <strong>of</strong> life, wellbeing,<br />
ability to work, and the family. (P)<br />
5. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> cough. (P, SBP)<br />
D. REFERENCES:<br />
90
Currie GP, Gray RD, McKay J. Chronic cough. BMJ. 2003;326:261.<br />
Irwin RS, Madison JM. The persistently troublesome cough. Am J Respir Crit Care Med.<br />
2002;165:1469-74.<br />
Jones HC, Chang SI. Clinical Inquires. What is the best approach to the evaluation and<br />
treatment <strong>of</strong> chronic cough? J Fam Pract. 2001;50:748-9.<br />
Irwin RS, Madison MJ. Primary care: the diagnosis and treatment <strong>of</strong> cough. N Engl J Med.<br />
2000;343:1715-21.<br />
Irwin RS, Boulet LP, Cloutier MM, et al. Managing cough as a defense mechanism and as a<br />
symptom. Consensus panel report <strong>of</strong> the American College <strong>of</strong> Chest Physicians. Chest.<br />
1998;114:133S-181S.<br />
91
TRAINING PROBLEM #8: DYSPNEA<br />
RATIONALE:<br />
Shortness <strong>of</strong> breath or dyspnea is one <strong>of</strong> the most common patient complaints encountered in<br />
internal medicine. It has a very large number <strong>of</strong> etiologic possibilities— some benign but many<br />
potentially life-threatening. Because <strong>of</strong> the latter, a systematic approach to dyspnea is crucial.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy, physiology, and pathophysiology <strong>of</strong> the pulmonary, cardiac, neurologic, and<br />
musculoskeletal systems.<br />
Physiology <strong>of</strong> acid-base homeostasis.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Major organ systems/pathologic states causing dyspnea and their<br />
pathophysiology, including:<br />
Cardiac. (MK)<br />
Pulmonary. (MK)<br />
Anemia/hypovolemia. (MK)<br />
Acid-base disorders and other metabolic derangements (MK)<br />
Neuromuscular weakness. (MK)<br />
Central neurologic derangements. (MK)<br />
2. The symptoms, signs, and laboratory values associated with respiratory failure and ventilatory<br />
failure. (MK)<br />
3. The alveolar-arterial oxygen gradient and the pathophysiologic states that can alter it. (MK)<br />
4. The potential risks <strong>of</strong> relying too heavily on pulse oximetry as the sole indicator <strong>of</strong> arterial<br />
oxygen content. (MK)<br />
5. The common causes <strong>of</strong> acute dyspnea, their pathophysiology, symptoms, and signs, including:<br />
Pulmonary edema. (MK)<br />
Pulmonary embolism. (MK)<br />
Pneumonia. (MK)<br />
Acute exacerbation <strong>of</strong> COPD. (MK)<br />
Asthma. (MK)<br />
Cardiac ischemia. (MK)<br />
Pneumothorax. (MK)<br />
Anxiety. (MK)<br />
6. The common causes <strong>of</strong> chronic dyspnea their pathophysiology, symptoms, and signs,<br />
including:<br />
Congestive heart failure. (MK)<br />
COPD. (MK)<br />
Pulmonary parenchymal disease. (MK)<br />
Pulmonary vascular disease. (MK)<br />
92
Anemia. (MK)<br />
Neuromuscular weakness. (MK)<br />
7. Basic treatment options for the common causes <strong>of</strong> acute and chronic dyspnea. (MK)<br />
8. The utility <strong>of</strong> supplemental oxygen therapy and the potential dangers <strong>of</strong> overly aggressive<br />
oxygen supplementation in some pathophysiologic states. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, that differentiates among etiologies <strong>of</strong> disease,<br />
including:<br />
Quantity, quality, severity, duration, ameliorating/exacerbating factors <strong>of</strong> the dyspnea. (PC,<br />
CS)<br />
Associated symptoms such as fevers, chills, sweats, orthopnea, paroxysmal nocturnal<br />
dyspnea, wheezing, edema, chest pain, cough, sputum production, hemoptysis,<br />
palpitations, nausea, anxiety, dizziness, orthostasis, weakness. (PC, CS)<br />
History <strong>of</strong> pulmonary, cardiac, neuromuscular/neurologic, renal, hepatic, and coagulopathic<br />
disorders. (PC, CS)<br />
Risk factors for deep vein thrombosis/pulmonary embolism. (PC, CS)<br />
Ingestion <strong>of</strong> drugs and toxic substances, administration <strong>of</strong> IV fluids. (PC, CS<br />
Smoking and environmental exposures. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Accurately determining respiratory rate and level <strong>of</strong> respiratory distress. (PC)<br />
Assessing the use <strong>of</strong> accessory muscles for breathing. (PC)<br />
Accurately measuring pulsus paradox. (PC)<br />
Identifying bronchial breath sounds, rales, rhonchi, wheezes, and subcutaneous<br />
emphysema. (PC)<br />
Identifying signs <strong>of</strong> pulmonary consolidation and hyperresonance. (PC)<br />
Identifying signs <strong>of</strong> pleural effusion. (PC)<br />
Identifying signs <strong>of</strong> elevated central venous pressure. (PC)<br />
Identifying signs <strong>of</strong> hypovolemia. (PC)<br />
Identifying S3 gallop, edema, and pallor. (PC)<br />
Identifying signs <strong>of</strong> deep vein thrombosis. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology <strong>of</strong><br />
dyspnea (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
CBC. (PC, MK)<br />
Electrolytes, BUN/Cr, GLC. (PC, MK)<br />
Pulse oximitry. (PC, MK)<br />
ABG. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
12-lead ECG. (PC, MK)<br />
Pulmonary function tests. (PC, MK)<br />
93
Students should be able to define the indications for and interpret (with consultation) the<br />
results <strong>of</strong>:<br />
Ventilation perfusion scintigraphy. (PC, MK)<br />
Chest CT. (PC, MK)<br />
Venous Doppler studies. (PC, MK)<br />
Cardiac stress test. (PC, MK)<br />
Echocardiography. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Counsel and educate patients about environmental contributors to their disease. (PC, CS)<br />
Counsel patients nonjudgmentally about smoking cessation. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Obtain an ABG. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and treatment<br />
plan for patients that includes:<br />
A rapid triage approach to the acutely dyspneic patient. (PC, MK)<br />
An appropriate assessment <strong>of</strong> the patient’s oxygenation status. (PC, MK)<br />
Appropriate oxygen supplementation as indicated. (PC, MK)<br />
Management plans for pulmonary edema/congestive heart failure, pneumonia, COPD,<br />
asthma, pulmonary embolism, cardiac ischemia, hypovolemia, anemia, and pneumothorax.<br />
(PC, MK)<br />
Determining when to obtain consultation from an appropriate specialist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to dyspnea. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for dyspnea. (PLI, P)<br />
2. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for dyspnea. (P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding dyspnea. (PLI, P)<br />
4. Appreciate the impact dyspnea has/have on a patient’s quality <strong>of</strong> life, wellbeing, ability to work,<br />
and the family. (P)<br />
5. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization<br />
<strong>of</strong> other healthcare pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> dyspnea. (P, SBP)<br />
6. Show understanding for the difficulties patients face with smoking cessation. (P)<br />
D. REFERENCES:<br />
Ingram RH and Braunwald E. (2005). Dyspnea and pulmonary edema. In Kasper DL,<br />
Braunwald EB, Fauci AS, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles<br />
94
<strong>of</strong> Internal <strong>Medicine</strong>. 16 th ed. New York, NY: McGraw-Hill; 2005:201-5.<br />
Zoorob RJ. Campbell JS. Acute dyspnea in the <strong>of</strong>fice. Am Fam Physician.<br />
2003;68:1803-10.<br />
Fedullo PF. Tapson VF. Clinical practice. The evaluation <strong>of</strong> suspected pulmonary<br />
embolism. N Engl J Med. 2003;349:1247-56.<br />
Manning HL. Schwartzstein RM. Pathophysiology <strong>of</strong> dyspnea. N Engl J Med.<br />
1995;333:1547-53.<br />
95
TRAINING PROBLEM #9: DYSURIA<br />
RATIONALE:<br />
Dysuria is a very common presentation in the outpatient setting. Given the amount <strong>of</strong> health care<br />
dollars that are spent on antibiotic treatment <strong>of</strong> urinary tract infections as well as the emergence <strong>of</strong><br />
resistance, it is important for third year medical students to have a working knowledge <strong>of</strong> how to<br />
approach the patient with this complaint, and how to differentiate patients with cystitis from other<br />
common causes <strong>of</strong> dysuria.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> genitourinary anatomy, physiology and pathophysiology.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Presenting signs and symptoms <strong>of</strong> the common causes <strong>of</strong> dysuria, including:<br />
Cystitis. (MK)<br />
Urethritis, gonococcal and non-gonococcal (e.g. chlamydia, trichomonas, HSV). (MK)<br />
Pyelonephritis. (MK)<br />
Acute and chronic prostatitis. (MK)<br />
Epididymitis. (MK)<br />
Vaginitis (yeast, bacterial vaginosis, trichomonas, atrophic, irritant). (MK)<br />
Interstitial cystitis. (MK)<br />
2. Symptoms and signs <strong>of</strong> pyelonephritis and how to distinguish an upper from a lower UTI. (MK)<br />
3. Common bacteria that cause UTI. (MK)<br />
4. Aspects <strong>of</strong> pathogenesis that affect UTI, including gender, sexual activity, diabetes, anatomic<br />
anomalies, instrumentation, and use <strong>of</strong> an indwelling catheter. (MK)<br />
5. Indications for pursuing further work up for patients with UTI. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
history that differentiates among etiologies <strong>of</strong> dysuria, including:<br />
Timing, frequency, severity, and location <strong>of</strong> dysuria. (PC, CS)<br />
Fever, chills, sweats. (PC, CS)<br />
Frequency, urgency, hesitancy, incomplete voiding. (PC, CS)<br />
Back, abdominal, and groin pain. (PC, CS)<br />
History <strong>of</strong> nephrolithiasis. (PC, CS)<br />
Hematuria. (PC, CS)<br />
Vaginal or penile discharge. (PC, CS)<br />
Penile skin lesions. (PC, CS)<br />
Sexual activity. (PC, CS)<br />
History <strong>of</strong> sexual transmitted diseases. (PC, CS)<br />
96
Dyspareunia. (PC, CS)<br />
Scrotal, testicular, and perineal pain. (PC, CS)<br />
Use <strong>of</strong> topical hygiene products. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Percussion and palpation <strong>of</strong> the bladder to accurately recognize distention and tenderness.<br />
(PC)<br />
Palpation over the kidneys to elicit flank tenderness. (PC)<br />
Palpation <strong>of</strong> the abdomen to elicit tenderness. (PC)<br />
Palpation and massage <strong>of</strong> the male prostate to obtain discharge. (PC)<br />
Accurate recognition <strong>of</strong> perineal or vaginal atrophy and inflammation. (PC)<br />
Techniques <strong>of</strong> the pelvic examination to assess for causes <strong>of</strong> vaginitis. (PC)<br />
3. Differential diagnosis: Students should be able to generate a differential diagnosis<br />
recognizing specific history, physical exam, and laboratory findings that suggest a specific<br />
etiology <strong>of</strong> dysuria. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Urinalysis interpretation including cells and casts, urine dipstick and Gram stain when<br />
appropriate. (PC, MK)<br />
Urine culture. (PC, MK)<br />
Gram stain and culture <strong>of</strong> urethral or cervical discharge. (PC, MK)<br />
KOH stain and normal saline wet prep <strong>of</strong> vaginal discharge. (PC, MK)<br />
Urinary or cervical PCR to test for gonorrhea and Chlamydia. (PC, MK)<br />
KUB radiograph. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit input and questions from the patient and his or her family about the management<br />
plan. (PC, CS)<br />
Counsel patients about safe sexual activity. (PC, CS)<br />
Explain the risk <strong>of</strong> recurrent UTI and counsel regarding preventative measures. (PC, CS)<br />
6. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Selecting appropriate empiric antibiotic therapy for cystitis, pyelonephritis or urethritis prior<br />
to culture results. (PC, MK)<br />
Counseling patients on symptomatic therapies for acute cystitis. (PC, MK)<br />
Selecting the appropriate duration <strong>of</strong> therapy for cystitis and pyelonephritis. (PC, MK)<br />
Evaluating and managing patients with recurrent urinary tract infections including<br />
prophylaxis. (PC, MK)<br />
Choosing appropriate treatment for vaginitis depending on results <strong>of</strong> evaluation. (PC, MK)<br />
Understanding the treatment <strong>of</strong> prostatitis based on probable organisms and age. (PC, MK)<br />
Determining when to obtain consultation from a urologist or gynecologist. (PC, MK)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to dysuria. (PC, PLI)<br />
97
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for dysuria. (PLI, P)<br />
2. Recognize the importance <strong>of</strong> patient needs and preferences when selecting among diagnostic<br />
and therapeutic options for dysuria. (P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding dysuria. (PLI, P)<br />
4. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essionals in the treatment <strong>of</strong> dysuria. (P, SBP)<br />
D. REFERENCES:<br />
32.<br />
Bremnor JD, Sadovsky R. Evaluation <strong>of</strong> dysuria in adults. Am Fam Physician.<br />
2002;65:1589-96.<br />
Bent S, Nallamothu BK, Simel DL, et al. Does this woman have an acute<br />
uncomplicated urinary tract infection? JAMA. 2002;287:2701-10.<br />
Owen MK, Clenney TL. Management <strong>of</strong> vaginitis. Am Fam Physician. 2004;70:2125-<br />
Fihn SD. Clinical practice. Acute uncomplicated urinary tract infection in<br />
women. N Engl J Med. 2003;349:259-66.<br />
98
TRAINING PROBLEM #10: FEVER<br />
RATIONALE:<br />
Because fever can have many infectious or noninfectious causes, patients with fever should be<br />
stratified by host susceptibility factors and evaluated in a systematic manner. A rational approach to<br />
patients with fever will help clinicians recognize presentations that need immediate attention, limit<br />
unnecessary diagnostic testing in less seriously ill patients, and help inform therapeutic decision<br />
making.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Physiology and pathophysiology <strong>of</strong> thermoregulation and the immune response.<br />
Pharmacology <strong>of</strong> antipyretics.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Physiology <strong>of</strong> the acute febrile response, including the:<br />
Beneficial and detrimental effects <strong>of</strong> fever upon the host. (MK)<br />
The differences in clinical manifestations between immunocompetent and<br />
immunocompromised patients. (MK)<br />
2. Risk factors and co-morbidities that are important in determining the host response to infection<br />
(e.g. neutropenia, asplenia, cirrhosis, alcoholism, diabetes, corticosteroid use, malnutrition, T<br />
cell dysfunction) (MK)<br />
3. Etiology <strong>of</strong> fever in special populations, including patients with a history <strong>of</strong>:<br />
Neutropenia due to cancer-related myelosuppression. (MK)<br />
HIV disease. (MK)<br />
Intravenous drug abuse. (MK)<br />
Recent international travel or immigration. (MK)<br />
Concomitant skin rash and lymphadenopathy. (MK)<br />
4. Pathophysiology and clinical presentation <strong>of</strong> patients with sepsis syndromes. (MK)<br />
5. Common causes <strong>of</strong> prolonged fever without apparent source, including:<br />
FUO in a normal host. (MK)<br />
Nosocomial FUO. (MK)<br />
Neutropenic FUO. (MK)<br />
FUO associated with HIV disease. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Chronology, duration and pattern <strong>of</strong> fever. (PC, CS)<br />
Associated symptoms. (PC, CS)<br />
Immune status and baseline co-morbidities. (PC, CS)<br />
Immunization status. (PC, CS)<br />
99
Relevant history <strong>of</strong> exposures. (PC, CS)<br />
Occupational, travel, family, and sexual history. (PC, CS)<br />
Medication history, including use <strong>of</strong> over-the-counter and illicit drugs. (PC, CS)<br />
3. Physical exam skills: Students should be able to perform a complete physical exam to<br />
determine the severity <strong>of</strong> disease and establish a preliminary hypothesis about the cause <strong>of</strong><br />
fever. (PC)<br />
4. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology:<br />
Infection. (PC, MK)<br />
Rheumatologic disease/inflammatory disorder. (PC, MK)<br />
Malignancy. (PC, MK)<br />
Drug reaction. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
CBC with differential. (PC, MK)<br />
UA with exam <strong>of</strong> urinary sediment. (PC, MK)<br />
Chest radiography. (PC, MK)<br />
Blood cultures. (PC, MK)<br />
Urine cultures. (PC, MK)<br />
Sputum Gram stain and cultures. (PC, MK)<br />
Sputum AFB stain and culture. (PC, MK)<br />
ESR and/or specific rheumatologic tests. (PC, MK)<br />
PPD. (PC, MK)<br />
Cerebrospinal fluid analysis (color, opening pressure, chemistries, cell<br />
counts, staining, cultures, cytology, cryptococcal antigen, VDRL). (PC, MK)<br />
Chemistries, Gram stain, and culture <strong>of</strong> abnormal fluid collections<br />
(e.g. pleural effusion, ascites, abscesses). (PC, MK)<br />
Stool culture <strong>of</strong> enteric pathogens. (PC, MK)<br />
Stool Clostridium difficile toxin assay. (PC, MK)<br />
Stains and cultures from the throat, urethra, anus, cervix, vagina. (PC, MK)<br />
HIV ELISA and western blot. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
results <strong>of</strong>:<br />
CT imaging. (PC, MK)<br />
Echocardiography. (PC, MK)<br />
Tissue biopsy. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up patients. (PC, CS)<br />
Elicit questions from the patient and their family about the management plan. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Obtain blood, wound, and throat cultures. (PC)<br />
Place and interpret a PPD. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
100
Developing an appropriate evaluation plan for patients with fever including ordering and<br />
interpreting appropriate laboratory and radiographic studies. (PC)<br />
Assessing the severity <strong>of</strong> presentation based on the history, host factors, physical exam<br />
and laboratory results and recognizing presentations that need immediate attention. (PC)<br />
Developing an appropriate treatment plan for patients with fever including the selection <strong>of</strong><br />
an initial, empiric treatment regimen for neutropenic patients with fever and/or patients with<br />
life threatening sepsis. (PC)<br />
Determining when to obtain consultation from an appropriate specialist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to fever. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
3. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for fever. (P, PLI)<br />
4. Appreciate the impact fever has on a patient’s quality <strong>of</strong> life, well-being, ability to work, and<br />
family; recognize the emotional impact <strong>of</strong> differential diagnosis. (P)<br />
5. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essions in the diagnosis and treatment <strong>of</strong> fever. (P, SBP)<br />
D. REFERENCES:<br />
Dinarello CA, Gelfand JA. (2005). Fever and hyperthermia. In Kasper DL, Braunwald<br />
EB, Fauci AS, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal<br />
<strong>Medicine</strong>. 16 th ed. New York, NY: McGraw-Hill; 2005:104-8.<br />
Kaye ET, Kaye KM. (2005). Fever and rash. In Kasper DL, Braunwald EB, Fauci AS,<br />
Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16 th<br />
ed. New York, NY: McGraw-Hill; 2005:108-16.<br />
Gelfand JA, Callahan MV. (2005). Fever <strong>of</strong> unknown origin. In Kasper DL, Braunwald<br />
EB, Fauci AS, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal<br />
<strong>Medicine</strong>. 16 th ed. New York, NY: McGraw-Hill; 2005:116-21.<br />
Roth AR, Basello GM. Approach to the adult patient with fever <strong>of</strong> unknown origin. Am<br />
Fam Physician. 2003;68:2223-8.<br />
101
TRAINING PROBLEM #11: FLUID, ELECTROLYTE AND<br />
ACID-BASE DISORDERS<br />
RATIONALE:<br />
Many disease processes can cause serious disturbances in the fluid, electrolyte and acid-base<br />
status <strong>of</strong> patients. Clinicians must be prepared to identify and correct these disturbances as<br />
efficiently as possible, thus making it an important training problem for third year medical students.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> pathogenesis and pathophysiology <strong>of</strong> fluid, electrolyte and acid-base disorders.<br />
Knowledge <strong>of</strong> medications that can cause alterations in fluid and electrolyte status as well as<br />
disturbance <strong>of</strong> acid-base status.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe and discuss:<br />
1. The pathophysiology <strong>of</strong>:<br />
Hypo- and hypervolemia. (MK)<br />
Hypo- and hypernatremia. (MK)<br />
Hypo- and hyperkalemia. (MK)<br />
Hypo- and hypercalcemia. (MK)<br />
Simple and mixed acid-base disorders. (MK)<br />
Hypo- and hyperphosphatemia. (MK)<br />
Hypo- and hypermagnesemia. (MK)<br />
Respiratory acidosis and alkalosis. (MK)<br />
Metabolic acidosis and alkalosis. (MK)<br />
2. Presenting symptoms and signs <strong>of</strong> the above disorders. (MK)<br />
3. The importance <strong>of</strong> total body water and its distribution. (MK)<br />
4. The differential diagnosis <strong>of</strong> hypo- and hypernatremia in the setting <strong>of</strong> volume depletion,<br />
euvolemia, and hypervolemia. (MK)<br />
5. How to distinguish hyponatremia from pseudohyponatremia. (MK)<br />
6. How to identify spurious hyperkalemia or acidosis-related hyperkalemia. (MK)<br />
7. Risks <strong>of</strong> too rapid or delayed therapy for hyponatremia. (MK)<br />
8. The most common causes <strong>of</strong> respiratory acidosis, respiratory alkalosis, metabolic acidosis and<br />
metabolic alkalosis. (MK)<br />
9. How to calculate the anion gap and explain its relevance to determining the cause <strong>of</strong> a<br />
metabolic acidosis. (MK)<br />
10. Changes in total body water distribution that occur with aging. (MK)<br />
11. How altered mental status can contribute to electrolyte disorders. (MK)<br />
12. Tests to use in the evaluation <strong>of</strong> fluid, electrolyte, and acid-base disorders. (MK)<br />
13. Indications for obtaining an ABG. (MK)<br />
102
14. The types <strong>of</strong> fluid preparations to use in the treatment <strong>of</strong> fluid and electrolyte disorders. (MK)<br />
B. SKILLS: Students should demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Eliciting appropriate information from patients with volume overload, including recent weight<br />
gain, edema or ascites, symptoms <strong>of</strong> heart failure, dietary sodium intake, changes in<br />
medications, noncompliance and intravenous fluid regimens. (PC, CS)<br />
Eliciting appropriate information from patients with volume depletion, including recent<br />
weight loss, thirst, gastrointestinal losses, urinary losses, oral intake, insensible losses, and<br />
intravenous fluid regimens. (PC, CS)<br />
Eliciting appropriate information from patients with electrolyte problems, including use <strong>of</strong><br />
diuretics and other medications, gastrointestinal losses, and history <strong>of</strong> relevant medical<br />
conditions (e.g., heart failure, liver disease, renal disease, pulmonary disease, central<br />
nervous system disease, and malignancy). (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Measurement <strong>of</strong> orthostatic vital signs. (PC)<br />
Identification <strong>of</strong> signs <strong>of</strong> volume overload including peripheral edema, pulmonary edema,<br />
ascites, edema. (PC)<br />
Identification <strong>of</strong> signs <strong>of</strong> volume depletion including tachycardia, orthostatic hypotension,<br />
dry mucous membranes, poor skin turgor. (PC)<br />
Identification <strong>of</strong> signs <strong>of</strong> sodium disorders including lethargy, weakness, encephalopathy,<br />
delirium, seizures. (PC)<br />
Identification <strong>of</strong> signs <strong>of</strong> potassium disorders including weakness, fatigue, constipation,<br />
ileus, cramping, tetany, hypo- or hyperreflexia. (PC)<br />
Identification <strong>of</strong> signs <strong>of</strong> calcium disorders including cramping, tetany, Chvostek’s and<br />
Trousseau’s sign, seizures, anorexia, constipation, polyuria, hypo- or hyperreflexia, stupor,<br />
coma. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
diagnosis recognizing specific history, physical exam, and laboratory findings that<br />
distinguish between:<br />
Hypo- and hypervolemia. (PC, MK)<br />
Hypo- and hypernatremia. (PC, MK)<br />
Hypo- and hyperkalemia. (PC, MK)<br />
Hypo- and hypercalcemia. (PC, MK)<br />
Hypo- and hyperphosphatemia. (PC, MK)<br />
Hypo- and hypermagnesemia. (PC, MK)<br />
Respiratory acidosis and alkalosis. (PC, MK)<br />
Metabolic acidosis and alkalosis. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
Serum electrolytes, BUN/Cr. (PC, MK)<br />
Anion gap. (PC, MK)<br />
103
ABG. (PC, MK)<br />
Serum and urine osmolality. (PC, MK)<br />
Urinary sodium. (PC, MK)<br />
Fractional excretion <strong>of</strong> sodium. (PC, MK)<br />
ECG findings in hyper- and hypokalemia. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Explain to a patient and his or her family why intravenous fluids are needed. (PC, CS)<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit input and questions from the patient and their family about the management plan.<br />
(PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Insert a peripheral intravenous catheter. (PC)<br />
Obtain an ABG. (PC)<br />
Assist in the insertion <strong>of</strong> a central venous catheter. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Writing appropriate fluid orders for the treatment <strong>of</strong> hypo- and hypervolemia, hypo- and<br />
hypernatremia, hypo- and hyperkalemia, hypo- and hypercalcemia. (PC, MK)<br />
Writing appropriate orders for replacing sodium, potassium, calcium, phosphates, and<br />
magnesium. (PC, MK)<br />
Writing appropriate orders for correcting hyperkalemia, hypercalcemia, hyperphosphatemia<br />
and hypermagnesemia. (PC, MK)<br />
Calculating the water deficit that needs to be corrected to treat hypernatremia. (PC, MK)<br />
Identifying indications for administration <strong>of</strong> bicarbonate. (PC, MK)<br />
Determining when to obtain consultation from a nephrologist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to fluid, electrolyte, and acid-base disorders. (PC SBP)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for problems related<br />
to fluid, electrolyte and acid-base disorders. (PLI, P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding fluid, electrolyte and<br />
acid-based disorders. (PLI, P)<br />
4. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> problems related to fluid, electrolyte and acid-base disorders.<br />
(P, SBP)<br />
D. REFERENCES:<br />
Singer GG, Brenner BM. Fluid and Electrolyte Disturbances. In Kasper DL, Braunwald<br />
EB, Fauci AS, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal<br />
<strong>Medicine</strong>. 16 th ed. New York, NY: McGraw-Hill; 2005:252-63.<br />
DuBose TD. (2005). Acidosis and Alkalosis. In Kasper DL, Braunwald EB, Fauci AS,<br />
104
Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16 th<br />
ed. New York, NY: McGraw-Hill; 2005:263-71.<br />
Preston RA. Acid-Base, Fluids, and Electrolytes Made Ridiculously Simple. Miami, FL:<br />
MedMaster Incorporated; 2002.<br />
Adrogue HJ. Madias NE. Hyponatremia. N Engl J Med. 2000;342:1581-9.<br />
Adrogue HJ. Madias NE. Hypernatremia. N Engl J Med. 2000;342:1493-9.<br />
Stewart AF. Clinical practice: Hypercalcemia associated with cancer. N Engl J Med.<br />
2005;352:373-9.<br />
Carroll MF. Schade DS. A practical approach to hypercalcemia. Am Fam Physician.<br />
2003;67:1959-66.<br />
Gennari FJ. Hypokalemia. N Engl J Med. 1998;339:451-8.<br />
105
TRAINING PROBLEM #12: GASTROINTESTINAL BLEEDING<br />
RATIONALE:<br />
Gastrointestinal bleeding is a common disorder which can be life-threatening if not properly<br />
diagnosed and treated. Knowledge <strong>of</strong> etiology, risk factors, approach, and management is<br />
integral to internal medicine training.<br />
Prerequisites:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy, physiology, and pathophysiology <strong>of</strong> the gastrointestinal tract.<br />
Pharmacology <strong>of</strong> non-steroidal anti-inflammatory medication (a major contributing factor in<br />
etiology <strong>of</strong> gastrointestinal bleeding) as well as proton pump inhibitors and other agents used<br />
in the acute setting for treatment <strong>of</strong> gastrointestinal bleeding.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The common causes for and symptoms <strong>of</strong> upper and lower gastrointestinal blood loss,<br />
including:<br />
Esophagitis/esophageal erosions. (MK)<br />
Mallory Weiss tear. (MK)<br />
Peptic and duodenal ulcer disease. (MK)<br />
Esophageal/gastric varices. (MK)<br />
Erosive gastritis. (MK)<br />
Arteriovenous malformations. (MK)<br />
Gastrointestinal tumors, benign and malignant. (MK)<br />
Diverticulosis. (MK)<br />
Ischemic colitis. (MK)<br />
Hemorrhoids. (MK)<br />
Anal fissures. (MK)<br />
2. The distinguishing features <strong>of</strong> upper versus lower GI bleeding (MK)<br />
3. The indications for inpatient versus outpatient evaluation and treatment (MK)<br />
4. The principles <strong>of</strong> stabilization and treatment <strong>of</strong> acute massive GI blood loss. (MK)<br />
5. The role <strong>of</strong> contributing factors in GI bleeding such as H. pylori infection; NSAIDs, alcohol,<br />
cigarette use, coagulopathies; and chronic liver disease. (MK)<br />
B. SKILLS: Students should demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an age<br />
appropriate history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Features that distinguish upper from lower GI bleeding. (PC, CS)<br />
Quantification <strong>of</strong> degree <strong>of</strong> blood loss. (PC, CS)<br />
Chronology and duration <strong>of</strong> bleeding. (PC, CS)<br />
Associated symptoms. (PC, CS)<br />
106
Relevant past medical history. (PC, CS)<br />
Medication history, including use <strong>of</strong> tobacco and alcohol. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical examination to<br />
establish the diagnosis and severity <strong>of</strong> disease, including:<br />
Postural blood pressure and pulse. (PC, MK)<br />
Abdominal palpation for organomegaly, masses, and tenderness. (PC, MK)<br />
Search for stigmata <strong>of</strong> chronic liver disease. (PC, CS)<br />
Anal and rectal examination. (PC, CS)<br />
3. Differential diagnosis: Students should be able to generate a differential diagnosis<br />
recognizing specific history and physical examination findings that suggest a specific etiology<br />
for GI bleeding. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order<br />
diagnostic and laboratory tests and be able to interpret them, both prior to and after initiating<br />
treatment based on the differential diagnosis, including consideration <strong>of</strong> test cost and<br />
performance characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Stool and gastric fluid tests for occult blood. (MK, PC)<br />
CBC. (MK, PC)<br />
PT/PTT. (MK, PC)<br />
Hepatic function panel. (MK, PC)<br />
Tests for Helicobacter pylori. (MK, PC)<br />
Students should be able to define the indications for and interpret (with consultation) results<br />
<strong>of</strong>:<br />
Esophagogastroduodenoscopy (EGD). (MK, PC)<br />
Colonoscopy. (MK, PC)<br />
Barium studies <strong>of</strong> the gastrointestinal tract. (MK, PC)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Start an IV line using a large bore (i.e. 18 gauge) needle. (MK, PC)<br />
Perform a stool or emesis occult blood testing. (MK, PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Establishing adequate venous access. (PC, MK)<br />
Administering crystalloid fluid resuscitation. (PC, MK)<br />
Ordering blood and blood product transfusion. (PC, MK)<br />
Determining when to obtain consultation from a gastroenterologist or a general surgeon.<br />
(PC, MK)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to gastrointestinal bleeding. (PC, PLI)<br />
Incorporating patient preferences. (PC,P)<br />
Outlining long-term management when appropriate (e.g. Helicobacter pylori eradication,<br />
antacid, H-2 blocker or proton pump inhibitor therapy, smoking /alcohol cessation, NSAID<br />
107
estriction, and dietary modification. (MK, CS)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for gastrointestinal<br />
bleeding. (PLI, P)<br />
2. Respond appropriately to patients who are nonadherent to treatment for gastrointestinal<br />
bleeding. (CS, P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding gastrointestinal bleeding.<br />
(PLI, P)<br />
4. Appreciate the impact gastrointestinal bleeding has on a patient’s quality <strong>of</strong> life, well-being,<br />
ability to work, and the family. (P)<br />
5. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong><br />
6. other health care pr<strong>of</strong>essions in the treatment <strong>of</strong> gastrointestinal bleeding. (P, SBP)<br />
D. RESOURCES:<br />
Fallah, MA, Prakash, C, Edmundowicz, S. Acute gastrointestinal bleeding. Med Clin<br />
North Am. 2000;84:1183-208.<br />
Laine L. (2005). Gastrointestinal bleeding. In Kasper DL, Braunwald EB, Fauci AS,<br />
Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16 th ed.<br />
New York, NY: McGraw-Hill; 2005:235-8.<br />
Del Valle J. (2005). Peptic ulcer disease and related disorders. In Kasper DL,<br />
Braunwald EB, Fauci AS, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong><br />
Internal <strong>Medicine</strong>. 16 th ed. New York, NY: McGraw-Hill; 2005:1746-62.<br />
Gearhart SL, Bulkley G. (2005). Common diseases <strong>of</strong> the colon and anorectum and<br />
mesenteric vascular insufficiency. In Kasper DL, Braunwald EB, Fauci AS, Hauser SL, Longo<br />
DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16 th ed. New York, NY:<br />
McGraw-Hill; 2005:1795-803.<br />
Mitchell SH, Schaefer DC. A new view <strong>of</strong> occult and obscure gastrointestinal<br />
bleeding. Am Fam Physician. 2004;69:875-81.<br />
108
TRAINING PROBLEM #13: KNEE PAIN<br />
RATIONALE:<br />
Musculoskeletal complaints are some <strong>of</strong> the most common problems for which patients seek medical<br />
attention, and the knee is the single most common joint pain. Many <strong>of</strong> these problems can be<br />
effectively tackled in the primary care setting without need for consultation. The principles presented<br />
in this training problem can be readily applied to other joint pains.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy and physiology <strong>of</strong> the musculoskeletal system.<br />
Pharmacology <strong>of</strong> acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), topical<br />
medications (capsaicin and lidocaine) and glucocorticoids.<br />
Basic bone radiograph interpretation.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
11. A systematic approach to joint pain based on an understanding <strong>of</strong> pathophysiology to classify<br />
potential causes. (MK)<br />
12. The effect <strong>of</strong> the time course <strong>of</strong> symptoms on the potential causes <strong>of</strong> joint pain (acute vs.<br />
subacute vs. chronic). (MK)<br />
13. The difference between and pathophysiology <strong>of</strong> arthralgia vs. arthritis and mechanical vs.<br />
inflammatory joint pain. (MK)<br />
14. The distinguishing features <strong>of</strong> intra-articular and periarticular complaints (joint pain vs. bursitis<br />
and tendonitis). (MK)<br />
15. The effect <strong>of</strong> the features <strong>of</strong> joint involvement on the potential causes <strong>of</strong> joint pain<br />
(monoarticular vs. oligoarticular vs. polyarticular, symmetric vs. asymmetric, axial and/or<br />
appendicular, small vs. large joints, additive vs. migratory vs. intermittent). (MK)<br />
16. Indications for performing an arthrocentesis and the results <strong>of</strong> synovial fluid analysis. (MK)<br />
17. The utility <strong>of</strong> describing the relative location <strong>of</strong> knee pain (anterior, medial, lateral, posterior).<br />
(MK)<br />
18. The relative frequency <strong>of</strong> the various causes <strong>of</strong> knee pain. (MK)<br />
19. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common intraarticular<br />
causes <strong>of</strong> knee pain:<br />
Osteoarthritis. (MK)<br />
Inflammatory arthropathies. (MK)<br />
Crystalline arthropathies. (MK)<br />
Septic arthritis. (MK)<br />
Patell<strong>of</strong>emoral pain syndrome. (MK)<br />
Cruciate ligament tear. (MK)<br />
Meniscal damage. (MK)<br />
10. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common<br />
periarticular causes <strong>of</strong> knee pain:<br />
109
Collateral ligament sprain/tear. (MK)<br />
Ileotibial band syndrome. (MK)<br />
Prepatellar bursitis. (MK)<br />
Popliteal (Baker) cyst. (MK)<br />
11. Basic symptomatic treatment for knee pain, including:<br />
Relative rest. (MK)<br />
Ice/heat. (MK)<br />
Compression. (MK)<br />
Elevation. (MK)<br />
Acetaminophen. (MK)<br />
Nonsteroidal anti-inflammatory drugs. (MK)<br />
Glucosamine and chondroitin sulfate. (MK)<br />
Physical therapy. (MK)<br />
Assistive devices. (MK)<br />
Topical “analgesics.” (MK)<br />
Corticosteroid injection. (MK)<br />
12. Indications for and efficacy <strong>of</strong> intra-articular corticosteroid injections. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Delineation <strong>of</strong> the specific features <strong>of</strong> the pain. (PC, CS)<br />
Presence <strong>of</strong> stiffness, swelling, warmth, redness. (PC, CS)<br />
Symptoms <strong>of</strong> instability, locking, clicking/popping, and weakness. (PC, CS)<br />
History <strong>of</strong> trauma, new activities, repetitive motion. (PC, CS)<br />
Impact on the patient’s ability to carry out activities <strong>of</strong> daily living. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Examination <strong>of</strong> the knee, including:<br />
o Inspection. (PC)<br />
o Palpation. (PC)<br />
o Range <strong>of</strong> motion. (PC)<br />
o Gait assessment. (PC)<br />
o Evaluation for effusion. (PC)<br />
o Assessment <strong>of</strong> ligamentous and cartilaginous stability. (PC)<br />
3 Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology for<br />
knee pain. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Synovial fluid analysis. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
results <strong>of</strong>:<br />
Plain radiographs <strong>of</strong> the knee. (PC, MK)<br />
CT and MRI <strong>of</strong> the knee. (PC, MK)<br />
110
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
6. Basic and advanced procedure skills: Students should be able to:<br />
Assist in the performance <strong>of</strong> an arthrocentesis and intra-articular corticosteroid injection.<br />
(PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and treatment<br />
plan for patients that includes:<br />
Determining when to perform an arthrocentesis. (PC, MK)<br />
Prescribing simple, nonmedicinal symptomatic measures such as rest, ice/heat,<br />
compression, and elevation. (PC, MK)<br />
Prescribing physical therapy and assistive devices (PC, MK)<br />
Prescribing exercise. (PC, MK)<br />
Counseling patients regarding weight loss. (PC, MK)<br />
Prescribing non-narcotic analgesics and anti-inflammatory agents. (PC, MK)<br />
Determining when to prescribe narcotic analgesics. (PC, MK)<br />
Determining when to prescribe intra-articular corticosteroid injection. (PC, MK)<br />
Determining when to obtain consultation from an orthopedic surgeon and rheumatologist.<br />
(PC, MK)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to knee pain. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for knee pain. (PLI, P)<br />
2. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic<br />
and therapeutic options for knee pain. (P)<br />
3. Respond appropriately to patients who are nonadherent to treatment for knee pain.<br />
(CS, P)<br />
4. Appreciate the impact chronic knee pain has on a patient’s quality <strong>of</strong> life,<br />
psychological well-being, ability to work, and the family. (P)<br />
5. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong><br />
other health care pr<strong>of</strong>essions in the treatment <strong>of</strong> knee pain. (P, SBP)<br />
6. Appreciate the difficulty patients with limited mobility have in achieving weight loss.<br />
(P)<br />
7. Demonstrate an appropriate attitude in managing patients with chronic pain. (P)<br />
D. REFERENCES:<br />
Cush JJ, Lipsky PE. (2005). Approach to articular and musculoskeletal disorders. In<br />
Kasper DL, Braunwald EB, Fauci AS, Hauser SL, Longo DL, Jameson JL, eds.<br />
111
Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16 th ed. New York, NY: McGraw-Hill;<br />
2005:2029-36.<br />
Brandt KD. (2005). Osteoarthritis. In Kasper DL, Braunwald EB, Fauci AS, Hauser SL,<br />
Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16 th ed. New<br />
York, NY: McGraw-Hill; 2005:2036-45.<br />
Principles <strong>of</strong> diagnosis and management: Pattern recognition in arthritis. In Klippel JH,<br />
Dieppe PA, Ferri FF, eds. Primary Care Rheumatology. St. Louis, MO: Mosby; 1999:11-<br />
7.<br />
Regional pain and monoarticular disorders: Pain in the knee. (1999). In Klippel JH,<br />
Dieppe PA, Ferri FF, eds. Primary Care Rheumatology. St. Louis, MO: Mosby; 1999:99-<br />
107.<br />
DeHaven KE. Knee and lower leg. In Greene WB, ed. Essentials <strong>of</strong> Musculoskeletal<br />
Care. 2 nd ed. Rosemont, IL: American Academy <strong>of</strong> Orthopedic Surgeons; 2001:341-405.<br />
112
TRAINING PROBLEM #14: RASH<br />
RATIONALE:<br />
Rash is an extremely common complaint. It may be the manifestation <strong>of</strong> a primary cutaneous<br />
disorder or secondary to a systemic condition. Internists see many patients with both and,<br />
therefore, must be acquainted with the diagnosis and management.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy, physiology, and pathophysiology <strong>of</strong> the skin.<br />
Pharmacology <strong>of</strong> glucocorticoids, antifungals, antibiotics, benzoyl peroxide, salicylic acid, and<br />
retinoids and derivatives.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
3. The standard nomenclature used to describe rashes (macule, patch, papule, nodule, plaque,<br />
vesicle, pustule, bulla, cyst, wheal, telangiectasia, petechia, purpura, erosion, ulcer). (MK)<br />
4. The morphologic features used to describe potentially malignant skin lesions (Asymmetry,<br />
Border, Color, Diameter, Dynamic i.e. changing, Elevation, and Enlargement, “ABCDE”). (MK)<br />
5. The significance <strong>of</strong> focal, organ-based, and constitutional signs and symptoms in the context <strong>of</strong><br />
a rash (e.g. rash and fever, rash and arthritis, rash and renal failure). (MK)<br />
4. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
eczematous dermatoses:<br />
Atopic dermatitis. (MK)<br />
Contact dermatitis. (MK)<br />
Stasis dermatitis. (MK)<br />
Seborrheic dermatitis. (MK)<br />
5. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
maculopapular eruptions:<br />
viral exanthems. (MK)<br />
bacterial exanthems. (MK)<br />
erythema multiforme. (MK)<br />
6. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
papulosquamous dermatoses:<br />
Psoriasis. (MK)<br />
Pityriasis rosea. (MK)<br />
7. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
cutaneous infections:<br />
Impetigo. (MK)<br />
Cellulitis. (MK)<br />
Folliculitis. (MK)<br />
Dermatophytosis (tinea corporis, tinea capitis, tinea cruris, tinea pedis, onychomycosis).<br />
(MK)<br />
113
Tinea versicolor. (MK)<br />
Candidiasis. (MK)<br />
Condylomata. (MK)<br />
Herpes zoster. (MK)<br />
8. The prevention <strong>of</strong> community acquisition <strong>of</strong> Methicillin-resistant Staphylococcus aureus<br />
(MRSA), including good hygiene practices:<br />
Keeping hands clean by washing thoroughly with soap and water or using an alcohol-based<br />
sanitizer. (MK)<br />
Keeping cuts and scrapes clean and covered with a bandage until healed. (MK)<br />
Avoiding contact with other people’s wounds or bandages. (MK)<br />
Avoiding sharing personal items such as towels and razors. (MK)<br />
9. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
pustular diseases:<br />
Acne. (MK)<br />
Rosacea. (MK)<br />
10. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
cutaneous ulcers.<br />
Venous insufficiency. (MK)<br />
Peripheral arterial disease. (MK)<br />
Neuropathic. (MK)<br />
11. The significance <strong>of</strong> palpable purpura and other cutaneous findings <strong>of</strong> vasculitis. (MK)<br />
12. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
urticaria and angioedema. (MK)<br />
13. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> drug eruptions. (MK)<br />
14. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
benign neoplasms and hyperplasias:<br />
Seborrheic keratosis. (MK)<br />
Epidermoid cyst. (MK)<br />
15. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the common causes <strong>of</strong><br />
premalignant lesions and malignancies:<br />
Actinic keratosis. (MK)<br />
Basal cell carcinoma. (MK)<br />
Squamous cell carcinoma. (MK)<br />
Malignant melanoma. (MK)<br />
16. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the cutaneous<br />
manifestations <strong>of</strong> sexually transmitted diseases.<br />
Syphilis. (MK)<br />
Disseminated gonorrhea infection. (MK)<br />
Human papilloma virus. (MK)<br />
Herpes simplex virus. (MK)<br />
17. The differential diagnosis, pathophysiology, and typical presentations <strong>of</strong> the cutaneous<br />
manifestations <strong>of</strong> internal/systemic diseases. (MK)<br />
18. The general indications for skin biopsy. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Evolution (site <strong>of</strong> onset, manner <strong>of</strong> spread, duration). (PC, CS)<br />
114
Symptoms associated with the rash (pruritis, pain, photosensitivity, malaise, fever,<br />
arthralgias). (PC, CS)<br />
Past medical history <strong>of</strong> systemic diseases known to have cutaneous manifestation. (PC,<br />
CS)<br />
Sexual history. (PC, CS)<br />
Medication usage and allergies. (PC, CS)<br />
Skin care product usage. (PC, CS)<br />
Chemical skin exposure. (PC, CS)<br />
Sun exposure. (PC, CS)<br />
Travel history. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease including:<br />
Description <strong>of</strong> the type <strong>of</strong> primary skin lesion (macule, patch, papule, nodule, plaque,<br />
vesicle, pustule, bulla, cyst, wheal, telangiectasia, petechia, purpura, erosion, ulcer). (PC)<br />
Description <strong>of</strong> the shape, margination, color, arrangement, and distribution <strong>of</strong> the individual<br />
lesions. (PC)<br />
Describe potentially malignant lesions in terms <strong>of</strong> Asymmetry, Border, Color, Diameter,<br />
Elevation, and Enlargement (“ABCDE”). (PC)<br />
Presence <strong>of</strong> exudates: dry (crust) or wet (weeping) exudates. (PC)<br />
Presence <strong>of</strong> scale or lichenification. (PC)<br />
Palpation <strong>of</strong> lesions for consistency, alteration <strong>of</strong> temperature, mobility, and tenderness.<br />
(PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
diagnosis recognizing specific history and physical exam findings that suggest a specific<br />
etiology for a rash. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order<br />
diagnostic and laboratory tests and be able to interpret them, both prior to and after initiating<br />
treatment based on the differential diagnosis, including consideration <strong>of</strong> test cost and<br />
performance characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
KOH preparation. (PC, MK)<br />
CBC with differential. (PC, MK)<br />
RPR and VDRL. (PC, MK)<br />
Bacterial culture. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
significance <strong>of</strong> the results <strong>of</strong>:<br />
• Skin biopsy. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Explain the dangers <strong>of</strong> excess sun exposure. (PC, CS)<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Counsel patients regarding the prevention <strong>of</strong> community acquisition <strong>of</strong> MRSA. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Perform a skin scraping and KOH preparation. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Determining when to perform a skin scraping and KOH preparation. (MK, PC)<br />
Determining when to obtain tests appropriate for the diagnosis <strong>of</strong> systemic medical<br />
115
conditions suspected as the cause <strong>of</strong> rash. (MK, PC)<br />
Prescribing a simple hypoallergenic skin care regimen. (MK, PC)<br />
Prescribing appropriate moisturizing/emollient treatment. (MK, PC)<br />
Discussing the importance <strong>of</strong> and prescribing sunscreen use. (PC, MK, CS)<br />
Prescribing appropriate treatment for eczematous dermatoses, mild psoriasis, common<br />
cutaneous skin infections, acne, rosacea, venous stasis dermatitis and ulcers, and common<br />
drug eruptions. (PC, MK)<br />
Determining when to obtain a consultation from a dermatologist. (PC)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to common dermatologic complaints. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
3. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for rashes. (PLI, P)<br />
4. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for rashes. (P)<br />
5. Appreciate the impact rashes have on a patient’s quality <strong>of</strong> life, well-being, ability to work,<br />
and the family. (P)<br />
D. REFERENCES:<br />
Drage LA. Life-threatening rashes: dermatologic signs <strong>of</strong> four infectious diseases. Mayo<br />
Clin Proc. 199;74:68-72.<br />
Williams HC. Clinical practice. Atopic dermatitis. N Engl J Med. 2005;352:2314-24.<br />
Abbasi NR. Shaw HM. Rigel DS. Friedman RJ. McCarthy WH. Osman I. Kopf AW.<br />
Polsky D. Early diagnosis <strong>of</strong> cutaneous melanoma: revisiting the ABCD criteria. JAMA.<br />
2004;292:2771-6.<br />
James WD. Clinical practice. Acne. N Engl J Med. 2005;352:1463-72.<br />
Wolff K, Johnson AJ, Suurmond R. Fitzpatrick’s Color Atlas & Synopsis <strong>of</strong> Clinical<br />
Dermatology. 4 th ed. New York, NY; 2005.<br />
American Academy <strong>of</strong> Dermatology<br />
Medical Student Core Curriculum<br />
www.aad.org/pr<strong>of</strong>essionals/Residents/MedStudCoreCurr/MedStudCoreC urr.htm<br />
Community-Associated MRSA<br />
Division <strong>of</strong> Healthcare Quality Promotion<br />
National Center for Infectious Diseases<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/ncidod/dhqp/ar_mrsa_ca.html<br />
116
TRAINING PROBLEM #15: UPPER RESPIRATORY COMPLAINTS<br />
RATIONALE:<br />
Upper respiratory tract infections (URIs) are some <strong>of</strong> the most common problems for which patients<br />
seek medical attention. Many patients inappropriately receive antibiotic therapy for these mostly<br />
viral infections.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy and physiology <strong>of</strong> the upper airway, Eustachian tubes, and sinuses.<br />
Anatomy and physiology <strong>of</strong> the respiratory system.<br />
Pathogenesis and pathophysiology <strong>of</strong> upper respiratory tract diseases.<br />
Microbial pathogens associated with upper respiratory tract infections.<br />
Pharmacology <strong>of</strong> antibiotics.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. A rational approach to the common URIs: nasal congestion, rhinorrhea, facial pain/tenderness,<br />
cough, sputum production, sore throat, and ear pain. (MK)<br />
2. Common constitutional symptoms that accompany URIs: generalized weakness, fatigue,<br />
malaise, headache, mild myalgias, and modest fever. (MK)<br />
3. The microbiology <strong>of</strong> URIs, highlighting the relative frequencies <strong>of</strong> viral and bacterial etiologies.<br />
(MK)<br />
4. The most common microbiologic agents that cause the common URIs. (MK)<br />
5. The pathophysiology and typical clinical presentation <strong>of</strong> the common URIs:<br />
Common cold. (MK)<br />
Acute bronchitis. (MK)<br />
Pharyngitis. (MK)<br />
Acute sinusitis. (MK)<br />
Otitis media. (MK)<br />
6. The pathophysiologic similarities between the common cold and acute sinusitis. (MK)<br />
7. The clinical features and microbiology <strong>of</strong> acute compared to chronic sinusitis. (MK)<br />
8. The pathophysiology and symptomatology <strong>of</strong> allergic rhinitis and the clinical features that may<br />
help differentiate it from the common cold and acute sinusitis. (MK)<br />
9. The clinical features that may help differentiate the common URIs from influenza. (MK)<br />
10. The pathophysiology and clinical features <strong>of</strong> acute compared to chronic bronchitis. (MK)<br />
11. The pathophysiology and clinical features <strong>of</strong> acute bronchitis compared to pneumonia. (MK)<br />
12. The pathophysiology and clinical features <strong>of</strong> otitis media and Eustachian tube malfunction.<br />
(MK)<br />
13. The signs and symptoms that may help distinguish viral from bacterial pharyngitis. (MK)<br />
14. Symptomatic treatment for URIs and the major side effects/contraindications for these<br />
treatments, including:<br />
Decongestants. (MK)<br />
Non-selective antihistamines. (MK)<br />
117
Mucolytics. (MK)<br />
Cough suppressants. (MK)<br />
Pain relievers/fever reducers. (MK)<br />
15. The general role <strong>of</strong> antibiotics in the treatment <strong>of</strong> URIs and specific evidence-based indications<br />
for them. (MK)<br />
16. The basic elements <strong>of</strong> the treatment <strong>of</strong> allergic rhinitis. (MK)<br />
17. The use <strong>of</strong> antiviral agents in the prophylaxis and treatment <strong>of</strong> influenza. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history, that differentiates among etiologies <strong>of</strong> disease, including:<br />
The predominant symptom (nasal congestion/rhinorrhea, purulent nasal discharge with<br />
facial pain/tenderness, sore throat, cough with or without sputum, sore throat or ear pain).<br />
(PC, CS)<br />
Constitutional symptoms. (PC, CS)<br />
Symptoms <strong>of</strong> potential pneumonia. (PC, CS)<br />
History <strong>of</strong> or symptoms <strong>of</strong> serious cardiopulmonary diseases (e.g. asthma, chronic<br />
obstructive pulmonary disease, congestive heart failure) that may alter the treatment plan.<br />
(PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Examination <strong>of</strong> the nasal cavity, pharynx, and sinuses. (PC)<br />
Otoscopic examination. (PC)<br />
Evaluation <strong>of</strong> the head and neck for lymphadenopathy. (PC)<br />
Auscultation <strong>of</strong> the lungs to distinguish pulmonary consolidation, pleural effusion,<br />
pulmonary congestion, and chronic obstructive pulmonary disease. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology <strong>of</strong><br />
upper respiratory complaints:<br />
Common cold. (PC, MK)<br />
Acute sinusitis. (PC, MK)<br />
Chronic sinusitis. (PC, MK)<br />
Allergic rhinitis. (PC, MK)<br />
Pharyngitis. (PC, MK)<br />
Otitis media. (PC, MK)<br />
Otitis externa. (PC, MK)<br />
Acute bronchitis. (PC, MK)<br />
Chronic bronchitis. (PC, MK)<br />
Influenza. (PC, MK)<br />
Pneumonia. (PC, MK)<br />
Infectious mononucleosis. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
CBC with differential. (PC)<br />
Rapid strep test. (PC)<br />
118
Throat culture. (PC)<br />
Chest radiograph. (PC)<br />
PFTs. (PC)<br />
Monospot/heterophile antibody. (PC)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (CS)<br />
Elicit questions from the patient and his or her family about the management plan. (CS)<br />
Explain the microbiologic origin <strong>of</strong> most URIs and why antibiotics are generally ineffective.<br />
(CS)<br />
Explain the importance <strong>of</strong> antimicrobial resistance. (CS)<br />
6. Basic and advanced procedure skills:<br />
• Throat culture. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Determining when to obtain a chest radiograph. (PC, MK)<br />
Determining when to prescribe antibiotics. (PC, MK)<br />
Selecting the most appropriate antibiotic for acute bacterial sinusitis, streptococcal<br />
pharyngitis, and bacterial otitis media. (PC, MK)<br />
Prescribing symptomatic treatments. (PC, MK)<br />
Determining when to obtain consultation from an allergist, otolaryngologist, or<br />
pulmonologist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to URIs. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1 Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for common URI complaints.<br />
(P, PLI)<br />
2 Appreciate the impact common URI complaints have on a patient’s quality <strong>of</strong> life, well-being,<br />
ability to work, and the family. (P)<br />
3 Discuss the patient’s perspective regarding the use <strong>of</strong> antibiotics for URIs. (CS, P)<br />
4 Discuss the role physicians play in the over-prescribing <strong>of</strong> antibiotics for URIs. (P)<br />
5 Discuss the importance <strong>of</strong> antimicrobial resistance from the point <strong>of</strong> view <strong>of</strong> the individual and<br />
society at large. (P)<br />
D. REFERENCES:<br />
Arroll B, Kenealy T. Antibiotics for the common cold and acute purulent rhinitis.<br />
Cochrane Database Syst Rev. 2005;(3):CD000247.<br />
Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344:205-11.<br />
Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat. Cochrane Database<br />
Syst Rev. 2004;(2):CD000023.<br />
Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired<br />
pneumonia? Diagnosing pneumonia by history and physical examination. JAMA.<br />
1997;278:1440-5.<br />
119
Smucny J, Fahey T, Becker L, et al. Antibiotics for acute bronchitis. Cochrane<br />
Database Syst Rev. 2004;(4):CD000245.<br />
Snow V, Mottur-Pilson C, Gonzales R, et al. Principles <strong>of</strong> appropriate antibiotic use for<br />
treatment <strong>of</strong> acute bronchitis in adults. Ann Intern Med. 2001;134:518-20.<br />
Guidelines for the Control <strong>of</strong> Pertussis Outbreaks<br />
National Immunization Program<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/nip/publications/pertussis/guide.htm<br />
Get Smart. Know When Antibiotics Work<br />
National Campaign for Appropriate Antibiotic Use<br />
Division <strong>of</strong> Bacterial and Mycotic Diseases<br />
National Center for Infectious Diseases<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/drugresistance/community/<br />
120
TRAINING PROBLEM #16: ACUTE MYOCARDIAL INFARCTION<br />
RATIONALE:<br />
Cardiovascular disease is the number one killer <strong>of</strong> Americans. Many associated risk factors are<br />
quite modifiable. Proper urgent management <strong>of</strong> acute myocardial infarctions significantly reduces<br />
mortality.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy and physiology <strong>of</strong> the heart and coronary vessels.<br />
Risk factors for and pathogenesis/pathophysiology <strong>of</strong> atherosclerosis.<br />
Pharmacology <strong>of</strong> aspirin, morphine, nitroglycerine, heparin, antiplatelet agents, thrombolytic<br />
agents, beta-blockers, angiotensin converting enzyme inhibitors (ACE-I), angiotensin II<br />
receptor blockers (ARB), and HMG-CoA reductase inhibitors.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The primary and secondary prevention <strong>of</strong> ischemic heart disease through the reduction <strong>of</strong><br />
cardiovascular risk factors (e.g. controlling hypertension and dyslipidemia, aggressive diabetes<br />
management, avoiding tobacco, and aspirin prophylaxis). (MK)<br />
2. The basic principles <strong>of</strong> the role <strong>of</strong> genetics in CAD. (MK)<br />
3. Pathogenesis, signs, and symptoms <strong>of</strong> the acute coronary syndromes:<br />
Unstable angina. (MK)<br />
Non-ST-elevation myocardial infarction (NSTEMI). (MK)<br />
ST-elevation myocardial infarction (STEMI). (MK)<br />
4. Atypical presentations <strong>of</strong> cardiac ischemia/infraction. (MK)<br />
5. The typical clinical course <strong>of</strong> the acute coronary syndromes. (MK)<br />
6. ECG findings and macromolecular markers (myoglobin, CK-MB, Troponin-I, Troponin-T) <strong>of</strong><br />
acute ischemia/MI. (MK)<br />
7. The utility <strong>of</strong> echocardiography in acute MI. (MK)<br />
8. The importance <strong>of</strong> monitoring for and immediate treatment <strong>of</strong> ventricular fibrillation in acute MI.<br />
(MK)<br />
9. Therapeutic options for acute MI and how they may differ for NSTEMI and STEMI, including:<br />
Aspirin. (MK)<br />
Morphine. (MK)<br />
Nitroglycerine. (MK)<br />
Oxygen. (MK)<br />
Heparin. (MK)<br />
Antiplatelet agents (glycoprotein IIb/IIIa inhibitors). (MK)<br />
Beta-blockers. (MK)<br />
ACE-I/ARB. (MK)<br />
HMG-CoA reductase inhibitors. (MK)<br />
Thrombolytic agents. (MK)<br />
121
Emergent cardiac catheterization with percutaneous coronary intervention. (MK)<br />
10. Pathogenesis, signs, and symptoms <strong>of</strong> the complications <strong>of</strong> acute MI, including arrhythmias,<br />
reduced ventricular function, cardiogenic shock, pericarditis, papillary muscle<br />
dysfunction/rupture, acute valvular dysfunction, and cardiac free wall rupture. (MK)<br />
11. The general approach to the evaluation and treatment <strong>of</strong> ventricular tachycardia and fibrillation.<br />
(MK)<br />
12. The importance <strong>of</strong> post-MI risk stratification, including the burden <strong>of</strong> residual coronary disease<br />
and assessment <strong>of</strong> left ventricular function. (MK)<br />
13. Basic principles <strong>of</strong> cardiac rehabilitation. (MK)<br />
14. Indications for coronary artery bypass grafting (CABG). (MK)<br />
15. The Centers for Medicare & Medicaid Services (CMS) and the Joint Commission on the<br />
Accreditation <strong>of</strong> Healthcare Organizations (JCAHO) quality measures for acute MI treatment.<br />
(MK, PLI, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Cardiac risk factors. (PC, CS)<br />
Location, duration, intensity, exacerbating/ameliorating factors, radiation <strong>of</strong> chest pain. (PC,<br />
CS)<br />
Symptoms associated with chest pain (e.g. nausea, emesis, dyspnea, diaphoresis,<br />
palpitations, dizziness, syncope, heartburn belching, etc.). (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease including:<br />
Recognition <strong>of</strong> dyspnea and anxiety. (PC)<br />
Accurate measurement <strong>of</strong> vital signs. (PC)<br />
Examination <strong>of</strong> the heart and vascular system. (PC)<br />
Examination <strong>of</strong> the lungs. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
diagnosis recognizing specific history and physical exam findings that suggest a specific<br />
etiology <strong>of</strong> chest pain:<br />
Stable angina. (PC, MK)<br />
Coronary vasospasm. (PC, MK)<br />
Unstable angina. (PC, MK)<br />
Acute MI. (PC, MK)<br />
Pericarditis. (PC, MK)<br />
Aortic dissection. (PC, MK)<br />
Pulmonary embolism. (PC, MK)<br />
Other noncardiac causes <strong>of</strong> chest pain. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
ECG. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
Macromolecular markers (myoglobin, CK-MB, Troponin-I, Troponin- T). (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
122
esults <strong>of</strong>:<br />
Echocardiogram. (PC, MK)<br />
Cardiac stress testing. (PC, MK)<br />
Coronary angiography. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient and his or her family about the diagnostic and management<br />
plan. (PC, CS)<br />
Educate patients about modifying cardiac risk factors. (PC, CS)<br />
6. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Medical management <strong>of</strong> acute MI. (PC, MK)<br />
CCU monitoring. (PC, MK)<br />
Indications for and complications <strong>of</strong> thrombolytic therapy, cardiac catheterization with<br />
percutaneous coronary intervention, and CABG. (PC, MK)<br />
Proper pre-discharge risk stratification. (PC, MK)<br />
Secondary risk factor modification. (PC, MK)<br />
Determining when to obtain consultation from a cardiologist and cardiothoracic surgeon.<br />
(PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to acute MI. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate a commitment to meeting national quality standards for the care <strong>of</strong><br />
patient with acute MI. (P, PLI, SBP)<br />
2. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for acute MI. (PLI, P)<br />
3. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic<br />
and therapeutic options for acute MI. (P)<br />
4. Demonstrate ongoing commitment to self-directed learning regarding acute MI. (PLI,<br />
P)<br />
5. Appreciate the impact acute MI has on a patient’s quality <strong>of</strong> life, well-being, ability to<br />
work, and the family. (P)<br />
6. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong><br />
other healthcare pr<strong>of</strong>essionals in the treatment <strong>of</strong> acute MI. (P, SBP)<br />
D. REFERENCES:<br />
ACC/AHA 2002 guideline update for the management <strong>of</strong> patients with chronic stable<br />
angina--summary article: a report <strong>of</strong> the American College <strong>of</strong> Cardiology/American<br />
Heart Association Task Force on practice guidelines (Committee on the Management<br />
<strong>of</strong> Patients with Chronic Stable Angina). J Am Coll Cardiol 2003; 41:159-68.<br />
www.acc.org/clinical/topic/topic.htm#guidelines<br />
ACC/AHA 2002 guideline update for the management <strong>of</strong> patients with unstable<br />
angina and non-ST-segment elevation myocardial infarction-summary article: a report<br />
123
<strong>of</strong> the American College <strong>of</strong> Cardiology/American Heart Association task force on<br />
practice guidelines (Committee on the Management <strong>of</strong> Patients With Unstable<br />
Angina). J Am Coll Cardiol. 2002;40:1366-74.<br />
www.acc.org/clinical/topic/topic.htm#guidelines<br />
ACC/AHA guidelines for the management <strong>of</strong> patients with ST-elevation myocardial<br />
infarction--executive summary. A report <strong>of</strong> the American College <strong>of</strong><br />
Cardiology/American Heart Association Task Force on Practice Guidelines (Writing<br />
Committee to revise the 1999 guidelines for the management <strong>of</strong> patients with acute<br />
myocardial infarction). J Am Coll Cardiol. 2004;44:671-719.<br />
Erratum in: J Am Coll Cardiol. 2005;45(8):1376.<br />
www.acc.org/clinical/topic/topic.htm#guidelines<br />
AHA/ACC Scientific Statement: AHA/ACC guidelines for preventing heart attack and<br />
death in patients with atherosclerotic cardiovascular disease: 2001 update: A<br />
statement for healthcare pr<strong>of</strong>essionals from the American Heart Association and the<br />
American College <strong>of</strong> Cardiology. Circulation. 2001;25:1577-9.<br />
www.acc.org/clinical/topic/topic.htm#guidelines<br />
124
TRAINING PROBLEM #17: ACUTE RENAL FAILURE AND<br />
CHRONIC KIDNEY DISEASE<br />
RATIONALE:<br />
Renal disease is a common problem in internal medicine and may manifest with symptoms<br />
referable to the kidney as well as other systems. Patients who go on to end-stage renal disease<br />
have high morbidity and mortality, despite advances in dialysis treatment. Thus, an understanding<br />
<strong>of</strong> chronic kidney disease is useful to all physicians. A rational approach to patients with suspected<br />
or known acute renal failure allows students and clinicians to quickly assess the etiology and initiate<br />
treatment without unnecessary delay in an effort to prevent the development <strong>of</strong> chronic kidney<br />
disease.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> pathogenesis and pathophysiology <strong>of</strong> acute renal failure and the development <strong>of</strong><br />
chronic kidney disease.<br />
Understanding <strong>of</strong> drugs that can have adverse effect on renal function.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe and discuss:<br />
1. The distinction between the three major pathophysiologic etiologies for acute renal failure<br />
(ARF):<br />
Decreased renal perfusion (prerenal). (MK)<br />
Intrinsic renal disease (renal). (MK)<br />
Acute renal obstruction (postrenal). (MK)<br />
2. The pathophysiology <strong>of</strong> the major etiologies <strong>of</strong> “prerenal” ARF, including:<br />
Hypovolemia. (MK)<br />
Decreased cardiac output. (MK)<br />
Systemic vasodilation. (MK)<br />
Renal vasoconstriction. (MK)<br />
3. The pathophysiology <strong>of</strong> the major etiologies <strong>of</strong> intrinsic “renal” ARF, including:<br />
Vascular lesions. (MK)<br />
Glomerular lesions. (MK)<br />
interstitial nephritis. (MK)<br />
Intra-tubule deposition/obstruction. (MK)<br />
Acute tubular necrosis (ATN). (MK)<br />
4. The pathophysiology <strong>of</strong> the major etiologies <strong>of</strong> “postrenal” ARF, including:<br />
Urethral (e.g. tumors, calculi, clot, sloughed papillae, retroperitoneal fibrosis,<br />
lymphadenopathy). (MK)<br />
Bladder neck (e.g. tumors, calculi, prostatic hypertrophy or carcinoma, neurogenic). (MK)<br />
Urethral (e.g. stricture, tumors, obstructed indwelling catheters). (MK)<br />
125
5. The pathophysiology and clinical findings <strong>of</strong> uremia. (MK)<br />
6. The natural history, initial evaluation and treatment, and complications <strong>of</strong> ARF. (MK)<br />
7. The most common etiologies <strong>of</strong> chronic kidney disease (CKD):<br />
DM. (MK)<br />
Hypertension. (MK)<br />
Glomerulonephritis. (MK)<br />
Polycystic kidney disease. (MK)<br />
Autoimmune diseases (e.g. systemic lupus erythematosus). (MK)<br />
The staging scheme for CKD. (MK)<br />
8. The significance for proteinuria in CKD. (MK)<br />
9. The use <strong>of</strong> ACE-Is and ARBs in the management <strong>of</strong> CKD. (MK)<br />
10. The importance <strong>of</strong> secondary hyperparathyroidism in CKD. (MK)<br />
11. The pathophysiology <strong>of</strong> anemia in CKD. (MK)<br />
12. The value <strong>of</strong> glycemic and hypertension control in limiting the progression <strong>of</strong> CKD.<br />
(MK)<br />
13. The value <strong>of</strong> CAD risk factor modification in patients with CKD, particularly those<br />
treated with dialysis. (MK)<br />
14. The basic principles <strong>of</strong> renal replacement therapy (e.g., hemodialysis and peritoneal<br />
dialysis) as well as the complications. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1 History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
history that distinguishes among the three major reasons for ARF (pre-renal, renal,<br />
post-renal), including the predisposing conditions, nephrotoxic drugs or agents, and systemic<br />
disease and the major causes <strong>of</strong> CKD. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical examination to establish<br />
the diagnosis and severity <strong>of</strong> disease, including:<br />
The determination <strong>of</strong> a patient’s volume status through estimation <strong>of</strong> the central venous<br />
pressure using the height <strong>of</strong> jugular venous distention and measurement <strong>of</strong> pulse and blood<br />
pressure in the lying/standing position. (PC)<br />
Palpation and percussion <strong>of</strong> the bladder to recognize bladder distention. (PC)<br />
Palpation <strong>of</strong> the prostate. (PC)<br />
Determination <strong>of</strong> the presence <strong>of</strong> pulmonary edema, peripheral edema, ascites, and signs<br />
<strong>of</strong> heart failure. (PC)<br />
Findings consistent with uremia. (PC)<br />
Examination for evidence <strong>of</strong> systemic disease, including but not limited to: skin, joints, and<br />
nails. (PC)<br />
3. Differential diagnosis: Students should be able to generate a differential diagnosis for a<br />
patient with ARF or CKD recognizing specific history, physical exam, and laboratory findings<br />
that suggest a specific etiology. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
Serum electrolytes, BUN/Cr, calcium, phosphorus. (PC, MK)<br />
Urine sodium. (PC, MK)<br />
Serum and urine osmolality. (PC, MK)<br />
126
Anion gap. (PC, MK)<br />
ABG (PC, MK)<br />
Serum BUN to Cr ratio. (PC, MK)<br />
CBC, ferritin. (PC, MK)<br />
Performing and interpreting a urinalysis, including microscopic examination for casts, red<br />
blood cells, white blood cells, and crystals. (PC, MK)<br />
Calculating fractional excretion <strong>of</strong> sodium and appreciate its usefulness in distinguishing<br />
between pre-renal and intrinsic renal disease. (PC, MK)<br />
Calculating creatinine clearance using the Cockcr<strong>of</strong>t-Gault or MDRD (“modification <strong>of</strong> diet<br />
in renal disease study”) equations. (PC, MK)<br />
Serum parathyroid hormone level. (PC, MK)<br />
ECG findings in hyperkalemia. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) results<br />
<strong>of</strong>:<br />
Renal ultrasonography. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Counsel patients regarding a renal diet. (PC, CS)<br />
6. Basic and advanced procedure skills: Students should be able to:<br />
Insert a peripheral intravenous catheter. (PC)<br />
Place a urinary catheter. (PC)<br />
Obtain an ABG. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients, including:<br />
Designing an appropriate management plan for initial management <strong>of</strong> ARF, including<br />
volume management, dietary recommendations, drug dosage alterations, electrolyte<br />
monitoring, and indications for dialysis. (PC, MK)<br />
Developing a management plan to effectively treat HTN and DM. (PC, MK)<br />
Recommending treatment with phosphate binders, calcium replacement, and vitamin D<br />
replacement. (PC, MK)<br />
Recommending treatment for dyslipidemia. (PC, MK)<br />
Recommending treatment for anemia secondary to CKD. (PC, MK)<br />
Recommending acute treatment for hyperkalemia. (PC, MK)<br />
Determining when to obtain consultation from a nephrologist. (PC, MK)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to renal failure. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
3. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based considerations in<br />
the selection <strong>of</strong> diagnostic and therapeutic interventions for ARF and CKD. (PLI, P)<br />
4. Respond appropriately to patients who are nonadherent to treatment for renal failure. (CS, P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding renal failure. (PLI, P)<br />
4. Appreciate the impact renal failure has on a patient’s quality <strong>of</strong> life, wellbeing, ability to work,<br />
127
and the family. (P)<br />
5. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> renal failure. (P, SBP)<br />
D. REFERENCES:<br />
11.<br />
Lamiere N, Van Breson W, Vanholder R. Acute renal failure. Lancet. 2005;365:417-30.<br />
Singri N, Ahya SN, Levin ML. Acute renal failure. JAMA. 2003;289:747-51.<br />
Schrier RW, Wang W, Poole B, Mitra A. Acute renal failure: definitions, diagnosis,<br />
pathogenesis, and therapy. J Clin Invest. 2004;114:5-14.<br />
Esson ML, Schrier RW. Diagnosis and treatment <strong>of</strong> acute tubular necrosis. Ann Intern<br />
Med. 2002;137:744-52.<br />
Levey AS. Clinical practice. Nondiabetic kidney disease. N Engl J Med. 2002;347:1505-<br />
Palmer BF. Renal dysfunction complicating the treatment <strong>of</strong> hypertension. N Engl J<br />
Med. 2002;347:1256-61.<br />
128
TRAINING PROBLEM #18: COMMON CANCERS<br />
RATIONALE:<br />
A skillful initial workup for suspected cancer is an essential part <strong>of</strong> effective primary care practice.<br />
Developing a logical and practical diagnostic approach to the more common cancers (e.g. skin,<br />
colorectal, lung, breast, cervical, and prostate) is an excellent means <strong>of</strong> honing basic history-taking,<br />
physical examination, and communication skills and learning how to use diagnostic studies in a cost<br />
effective manner. Encountering patients in whom cancer is a diagnostic possibility will stimulate<br />
learning <strong>of</strong> the important clinical presentations and natural histories <strong>of</strong> these life-threatening<br />
conditions. Focusing on cancer diagnosis helps to concentrate the student’s learning and avoids<br />
premature immersion in the <strong>of</strong>ten very technical and specialized issues <strong>of</strong> cancer treatment.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy, physiology, and pathophysiology <strong>of</strong> common cancers.<br />
Basic knowledge <strong>of</strong> the common symptoms and signs <strong>of</strong> the most common cancers.<br />
Knowledge <strong>of</strong> basic concepts <strong>of</strong> clinical epidemiology pertinent to test selection and<br />
interpretation (e.g. sensitivity, specificity, positive predictive value, negative predictive value).<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
3. Primary prevention measures for common cancers. (MK)<br />
4. Current screening recommendations for skin, colorectal, lung, breast, cervical, and<br />
prostate cancer. (MK)<br />
3. Principle clinical presentations, clinical courses, complications, and causes <strong>of</strong> death for the<br />
most common cancers (e.g. skin, colorectal, lung, breast, cervical, and prostate). (MK)<br />
4. Basic methods <strong>of</strong> initial evaluation, including the sensitivity and specificity <strong>of</strong> basic diagnostic<br />
studies and indication for their use, including:<br />
Indications for skin biopsy in a patient with a suspicious skin lesion. (MK)<br />
Indications for colonoscopy in individuals a risk for colon cancer. (MK)<br />
Indications for breast biopsy in a patient with a breast nodule or abnormal screening<br />
mammogram. (MK) Indications for a lymph node biopsy in a patent with suspicious<br />
lymphadenopathy. (MK)<br />
Initial cost-effective workups for: isolated pleural effusion, pulmonary nodule, liver nodule,<br />
prostate nodule, elevated prostate-specific antigen, testicular nodule, stool test positive for<br />
occult blood, abnormal<br />
Pap smear, and other findings suggestive <strong>of</strong> gastrointestinal and urogenital cancers.<br />
(MK)<br />
5. Genetic considerations <strong>of</strong> selected cancers (e.g. hereditary nonpolyposis colon cancer, familial<br />
adenomatous polyposis, BRCA1/BRCA2, HER2, Philadelphia chromosome/BRC-ABL). (MK)<br />
6. The role <strong>of</strong> human papilloma virus in cervical cancer. (MK)<br />
7. The similarities and differences between curative and palliative cancer care. (MK)<br />
8. The principles <strong>of</strong> palliative care and hospice care. (MK)<br />
9. Symptoms sometimes seen during end-<strong>of</strong>-life care and the basic principles <strong>of</strong> their<br />
129
management (e.g., pain, dyspnea, nausea and vomiting, anorexia, fatigue, depression,<br />
delirium, constipation). (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, that differentiates among etiologies <strong>of</strong> disease,<br />
including:<br />
Unintentional weight loss, fever, bone pain. (PC, CS)<br />
Sun exposure history, abnormal skin lesions. (PC, CS)<br />
Blood in the stool, alterations in bowel movements, abdominal pain, abdominal mass. (PC,<br />
CS)<br />
Smoking, cough, hemoptysis, chest pain, dyspnea. (PC, CS)<br />
Breast nodules and secondary signs <strong>of</strong> breast cancer. (PC, CS)<br />
Abnormal vaginal bleeding. (PC, CS)<br />
Abnormal urinary symptoms. (PC, CS)<br />
Lymphadenopathy. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Skin examination. (PC)<br />
Digital rectal examination. (PC)<br />
Breast examination. (PC)<br />
Lymph node examination. (PC)<br />
Male genital examination and prostate examination. (PC)<br />
Pelvic examination and Pap smear. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
diagnosis recognizing specific history and physical exam findings that suggest a specific<br />
etiology for:<br />
Unintentional weight loss. (PC, MK)<br />
Fever. (PC, MK)<br />
Abnormal skin lesions. (PC, MK)<br />
Occult blood positive stool. (PC, MK)<br />
Colorectal mass. (PC, MK)<br />
Chronic cough, hemoptysis, pulmonary nodule, and pleural effusion. (PC, MK)<br />
Breast mass. (PC, MK)<br />
Abnormal Pap smear. (PC, MK)<br />
Abdominal or pelvic mass. (PC, MK)<br />
Prostate nodule and elevated prostate specific antigen. (PC, MK)<br />
Lymphadenopathy. (PC, MK)<br />
5. Laboratory interpretation: Students should be able to recommend when to order<br />
diagnostic and laboratory tests and be able to interpret them, both prior to and after<br />
initiating treatment based on the differential diagnosis, including consideration <strong>of</strong> test<br />
cost and performance characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
CBC. (PC)<br />
Electrolytes, BUN/Cr, Ca, hepatic function panel. (PC)<br />
Stool occult blood testing. (PC)<br />
PSA. (PC)<br />
130
Students should be able to define the indications for and interpret (with consultation) the<br />
significance <strong>of</strong> the results <strong>of</strong>:<br />
Skin biopsy. (PC)<br />
Mammogram. (PC)<br />
Breast biopsy. (PC)<br />
Colon/rectal biopsy. (PC)<br />
Lung biopsy. (PC)<br />
Pap smear. (PC)<br />
Prostate biopsy. (PC)<br />
Lymph node biopsy. (PC)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnostic plan and subsequent follow-up to patients. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
With guidance and direct supervision, participate in breaking bad news to patients. (PC,<br />
CS)<br />
With guidance and direct supervision, participate in discussing basic issues regarding<br />
advance directives with the patient and his or her family. (PC, CS)<br />
With guidance and direct supervision participate in discussing basic end-<strong>of</strong>-life issues with<br />
the patient and his or her family. (PC, CS)<br />
6. Basic and advanced procedure skills: Students should be able to:<br />
Cervical Pap smear. (PC)<br />
Stool occult blood testing. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Initial work-up <strong>of</strong> the symptom, sign, or abnormal laboratory value suspected to be due to<br />
cancer. (PC)<br />
Provision <strong>of</strong> support and information for the patient. (PC)<br />
Coordination <strong>of</strong> care for workup. (PC, SBP)<br />
Determining when to obtain consultation from appropriate specialists. (PC, SBP)<br />
A cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to common cancers. (PC, PLI)<br />
Incorporating patient needs and preferences. (PC, P)<br />
Appropriately assessing and treating pain when necessary with nonnarctoic and narcotic<br />
analgesics. (PC)<br />
Anticipating and treating narcotic side effects if necessary. (PC)<br />
Adjusting the therapeutic plan when goals <strong>of</strong> care change (e.g., a shift toward palliative<br />
care). (PC)<br />
Alleviation <strong>of</strong> symptoms sometimes seen during end <strong>of</strong> life care (e.g., pain, dyspnea,<br />
nausea and vomiting, anorexia, fatigue, depression, delirium, constipation). (PC)<br />
Utilizing supportive care or hospice service when appropriate. (PC, SBP)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Appreciate the uncertainty and fear patients experience when cancer is a significant diagnostic<br />
possibility. (P)<br />
2. Respect the patient’s right to refuse cancer screening. (P)<br />
3. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
131
considerations in the selection diagnostic and therapeutic interventions for common cancers. (PLI, P)<br />
4. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic options for<br />
common cancers. (P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding common cancers. (PLI,<br />
P)<br />
6. Appreciate the impact common cancers have on a patient’s quality <strong>of</strong> life, well-being, ability to<br />
work, and the family. (P)<br />
7. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essions in the workup and treatment <strong>of</strong> common cancers. (P, SBP)<br />
D. REFERENCES:<br />
National Cancer Institute<br />
National Institutes <strong>of</strong> Health<br />
www.cancer.gov<br />
Guide to Clinical Preventive Services<br />
U.S. Preventative Services Task Force (USPSTF)<br />
Agency for Healthcare Research and Quality<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.ahrq.gov/clinic/cps3dix.htm#cancer<br />
American Cancer Society<br />
www.cancer.org<br />
NCCN Clinical Practice Guidelines in Oncology National Comprehensive<br />
Cancer Network<br />
www.nccn.org/pr<strong>of</strong>essionals/physician_gls/default.asp<br />
132
TRAINING PROBLEM #19: COPD/OBSTRUCTIVE AIRWAYS<br />
DISEASE<br />
RATIONALE:<br />
The chronic obstructive pulmonary diseases (chronic bronchitis and emphysema) are important<br />
causes <strong>of</strong> morbidity and mortality and are a major cause <strong>of</strong> total disability, second only to coronary<br />
artery disease. Cigarette smoking plays a major role in the progression <strong>of</strong> the disease, with survival<br />
rates lower among patients who continue to smoke cigarettes. The severity and debilitation <strong>of</strong> these<br />
disorders make them an important training problem for all third year medical students. The number<br />
<strong>of</strong> new cases <strong>of</strong> asthma is dramatically increasing. Most cases with appropriate treatment can have<br />
minimal symptoms.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Normal structure and function <strong>of</strong> the heart and lungs and how these are altered in respiratory<br />
system diseases.<br />
Pathogenesis and pathophysiology <strong>of</strong> pulmonary diseases.<br />
Pharmacology <strong>of</strong> bronchodilators, corticosteroids, and antibiotics.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The epidemiology, risk factors, symptoms, signs, and typical clinical course <strong>of</strong> the common<br />
forms <strong>of</strong> COPD, including chronic bronchitis and emphysema. (MK)<br />
2. Common causes <strong>of</strong> acute exacerbations <strong>of</strong> COPD (AECOPD), including:<br />
Acute infectious bronchitis. (MK)<br />
Pneumonia. (MK)<br />
Pulmonary edema. (MK)<br />
Poor air quality (e.g. ozone, pollutants, tobacco smoke). (MK)<br />
Occupational exposures. (MK)<br />
Medical noncompliance. (MK)<br />
3. The etiology, pathogenesis, evaluation, and management <strong>of</strong> hypoxemia and hypercapnia.<br />
(MK)<br />
4. The genetics and role <strong>of</strong> alpha-1 antitrypsin deficiency in some patients with emphysema. (MK)<br />
5. The epidemiology, risk factors, symptoms, signs, and typical clinical course <strong>of</strong> asthma. (MK)<br />
6. Allergic and non-allergic factors that may precipitate bronchospasm and exacerbate asthma,<br />
including:<br />
Grass and tree pollen. (MK)<br />
Animal dander. (MK)<br />
Cockroaches. (MK)<br />
Dust mites. (MK)<br />
Allergic rhinitis/post-nasal drip. (MK)<br />
133
Acute/chronic infectious sinusitis. (MK)<br />
Acute infectious bronchitis. (MK)<br />
Pneumonia. (MK)<br />
Pulmonary edema. (MK)<br />
Exercise. (MK)<br />
Anxiety/stress. (MK)<br />
Poor air quality (e.g. ozone, pollutants, tobacco smoke). (MK)<br />
Occupational exposures. (MK)<br />
Medical noncompliance. (MK)<br />
7. Therapies for COPD and asthma, including:<br />
Beta-agonist bronchodilators. (MK)<br />
Anticholinergic bronchodilators. (MK)<br />
Leukotriene inhibitors. (MK)<br />
Mast cell stabilizers. (MK)<br />
Theophylline. (MK)<br />
Inhaled corticosteroids. (MK)<br />
Systemic corticosteroids. (MK)<br />
Antimicrobial agents. (MK)<br />
Supplemental oxygen. (MK)<br />
Immunotherapy. (MK)<br />
8. The indications for and the efficacy <strong>of</strong> influenza and pneumococcal vaccines.<br />
(MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history, that differentiates among etiologies <strong>of</strong> disease including:<br />
Existence, duration, and severity <strong>of</strong> dyspnea, orthopnea, paroxysmal nocturnal dyspnea,<br />
cough, sputum production, wheezing, fever, chills, sweats, chest pain, hemoptysis. (PC,<br />
CS)<br />
Smoking history and passive exposure to tobacco smoke. (PC, CS)<br />
Occupational history. (PC, CS)<br />
Family history <strong>of</strong> pulmonary problems. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease including:<br />
Accurately determining respiratory rate and level <strong>of</strong> respiratory distress. (PC)<br />
Assessing the use <strong>of</strong> accessory muscles for breathing. (PC)<br />
Identifying bronchial breath sounds, rales, rhonchi, and wheezes. (PC)<br />
Identifying signs <strong>of</strong> pulmonary consolidation, pleural effusion, and pneumothorax. (PC)<br />
Identifying the signs <strong>of</strong> pulmonary hyperresonance/hyperexpansion. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a diagnosis <strong>of</strong> chronic<br />
bronchitis, emphysema, asthma, or other conditions with similar findings.<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
134
Pulse oximitry. (PC, MK)<br />
ABG. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
Pulmonary function tests. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Counsel patients about smoking cessation. (PC, CS)<br />
Counsel patients about the performance <strong>of</strong> home peak flow monitoring. (PC, CS)<br />
Counsel patients about environmental controls. (PC, CS)<br />
Encourage asthma patients to be involved in their own disease management and counsel<br />
them about an “asthma action plan.” (PC, CS)<br />
6. Basic and advanced procedure skills: Students should be able to:<br />
Obtain an ABG. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and treatment<br />
plan for patients that includes:<br />
The use <strong>of</strong> bronchodilators and inhaled corticosteroids. (PC, MK)<br />
The key components <strong>of</strong> the care <strong>of</strong> patients admitted with acute exacerbations <strong>of</strong> COPD<br />
and asthma. (PC, MK)<br />
Using systemic corticosteroids appropriately. (PC, MK)<br />
Judicious use <strong>of</strong> antimicrobial agents. (PC, MK)<br />
The principles <strong>of</strong> oxygen therapy. (PC, MK)<br />
Determining when to obtain consultation from a pulmonologist or allergist/immunologist.<br />
(PC, SBP)<br />
Smoking cessation strategies. (PC)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to COPD and asthma. (PC, PLI)<br />
Incorporating patient preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1 Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for COPD and asthma.<br />
(PLI, P)<br />
2 Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for COPD and asthma (P)<br />
3 Respond appropriately to patients who are nonadherent to treatment for COPD and asthma.<br />
(CS, P)<br />
4 Appreciate the impact <strong>of</strong> working, living, and environmental conditions on the development and<br />
progression <strong>of</strong> respiratory tract disease; demonstrate understanding that patients are <strong>of</strong>ten<br />
unable to change these factors on their own. (P)<br />
5 Demonstrate ongoing commitment to self-directed learning regarding COPD and asthma. (PLI,<br />
P)<br />
6 Appreciate the impact COPD and asthma have on a patient’s quality <strong>of</strong> life, well-being, ability<br />
to work, and the family. (P)<br />
7 Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> COPD and asthma. (P, SBP)<br />
135
8 Appreciate the importance <strong>of</strong> antimicrobial resistance. (P)<br />
9. Show understanding for the difficulties patients face with smoking cessation. (P)<br />
D. REFERENCES:<br />
National Heart Lung and Blood Institute/World Health Organization Global Initiative for<br />
Chronic Obstructive Lung Disease Diagnosis, management, and prevention <strong>of</strong> chronic<br />
obstructive pulmonary disease<br />
www.goldcopd.com<br />
National Institutes <strong>of</strong> Health, National Heart, Lung, and Blood Institute National Asthma<br />
Education and Prevention Program Practical Guide for the Diagnosis and Management<br />
<strong>of</strong> Asthma NIH Publication 97-4074. Bethesda, MD. 2003.<br />
http://www.nhlbi.nih.gov/health/indexpro.htm<br />
Celli BR, MacNee W. Standards for the diagnosis and treatment <strong>of</strong> patients with<br />
COPD: a summary <strong>of</strong> the ATS/ERS position paper. Eur Respir J 2004;23:932-46.<br />
136
TRAINING PROBLEM #20: DIABETES MELLITUS<br />
RATIONALE:<br />
Diabetes mellitus is an increasingly prevalent illness in the United States. It is estimated that five to<br />
nine percent <strong>of</strong> American adults are diabetic with the illness appearing at earlier ages in some<br />
populations. It is a leading cause <strong>of</strong> disability and death. Over 130 billion health care dollars are<br />
spent on diabetes annually. All internists must identify those at risk and institute appropriate<br />
management to ameliorate the potentially fatal complications <strong>of</strong> this illness.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Pathogenesis and pathophysiology <strong>of</strong> type I and II diabetes mellitus, diabetic ketoacidosis,<br />
nonketotic hyperglycemia.<br />
Effects <strong>of</strong> insulin on glucose and fat metabolism.<br />
Pharmacology <strong>of</strong> insulin, sulfonylureas, metformin, thiazolidinediones, and glucose absorption<br />
inhibitors.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Diagnostic criteria for impaired fasting glucose and impaired glucose tolerance. (MK)<br />
2. Diagnostic criteria for type I and type II diabetes mellitus, based on a history, physical<br />
examination, and laboratory testing. (MK)<br />
3. Pathophysiology, risk factors, and epidemiology <strong>of</strong> type I and type II diabetes mellitus. (MK)<br />
4. The basic principles <strong>of</strong> the role <strong>of</strong> genetics in diabetes mellitus. (MK)<br />
5. Presenting symptoms and signs <strong>of</strong> type I and type II diabetes mellitus. (MK)<br />
6. Presenting symptoms and signs <strong>of</strong> diabetic ketoacidosis (DKA) and nonketotic hyperglycemic<br />
(NKH). (MK)<br />
7. Pathophysiology for the abnormal laboratory values in DKA and NKH including plasma<br />
sodium, potassium, and bicarbonate. (MK)<br />
8. Precipitants <strong>of</strong> DKA and NKH. (MK)<br />
9. Major causes <strong>of</strong> morbidity and mortality in diabetes mellitus (coronary artery disease,<br />
peripheral vascular disease, hypoglycemia, DKA, NKH coma, retinopathy, neuropathy—<br />
peripheral and autonomic, nephropathy, foot disorders, infections). (MK)<br />
10. Laboratory tests needed to screen, diagnose, and follow diabetic patients including: glucose,<br />
electrolytes, blood urea nitrogen/creatinine, fasting lipid pr<strong>of</strong>ile, HgA1c, urine<br />
microalbumin/creatinine ratio, urine dipstick for protein. (MK)<br />
11. Non-pharmacologic and pharmacologic (drugs and side effects) treatment <strong>of</strong> diabetes mellitus<br />
to maintain acceptable levels <strong>of</strong> glycemic control, prevent target organ disease, and other<br />
associated complications. (MK)<br />
12. The specific components <strong>of</strong> the American Diabetes Association (ADA) dietary recommendations<br />
for type I and type II diabetes mellitus. (MK)<br />
13. Basic management <strong>of</strong> diabetic ketoacidosis and nonketotic hyperglycemic states, including the<br />
similarities and differences in fluid and electrolyte replacement. (MK)<br />
14. Basic management <strong>of</strong> blood glucoses in the hospitalized patient. (MK)<br />
137
15. The Somogyi effect and the Dawn phenomenon and the implications <strong>of</strong> each in diabetes<br />
pharmacologic management. (MK)<br />
16. The fundamental aspects <strong>of</strong> the American Diabetes Association (ADA) clinical practice<br />
recommendations and how they encourage high quality diabetes care. (MK, PLI, SBP)<br />
17. Basic management <strong>of</strong> hypertension and hyperlipidemia in the diabetic patient. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, that differentiates among etiologies <strong>of</strong> disease,<br />
including:<br />
Weight changes. (PC, CS)<br />
Hypo- or hyperglycemic symptoms. (PC, CS)<br />
Medication history (adherence, side effects, other medications). (PC, CS)<br />
Home glucose monitoring results. (PC, CS)<br />
Target organ disease complications (cardiovascular, foot, gastrointestinal, infectious,<br />
neurological, sexual, skin, urinary, or vision symptoms). (PC, CS)<br />
Diet history (total caloric intake, intake <strong>of</strong> sugar-containing foods, intake <strong>of</strong> saturated fat and<br />
cholesterol, physical activity level, timing <strong>of</strong> meals). (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Skin examination for diabetic dermopathy, furuncles/carbuncles, candidiasis, necrobiosis<br />
lipoidica diabeticorum, dermatophytosis, and acanthosis nigricans. (PC)<br />
Fundoscopic exam. (PC)<br />
Arterial pulses. (PC)<br />
Peripheral nerves (e.g. mon<strong>of</strong>ilament testing). (PC)<br />
Examination <strong>of</strong> the feet for corns, calluses, and ulcerations. (PC)<br />
In patients with DKA or NKH evaluate for mental status alterations, Kussmaul’s<br />
respirations, fruity breath, and signs <strong>of</strong> volume depletion. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology for:<br />
Hyperglycemia. (PC, MK)<br />
Hypoglycemia. (PC, MK)<br />
Anion gap acidosis. (PC, MK)<br />
Ketosis. (PC, MK)<br />
Hyperosmolality. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
Fasting serum GLC. (PC, MK)<br />
Electrolytes, BUN/Cr. (PC, MK)<br />
Serum and urine ketones. (PC, MK)<br />
Serum and urine osmolality. (PC, MK)<br />
HbA1c. (PC, MK)<br />
Fasting lipid pr<strong>of</strong>ile. (PC, MK)<br />
UA. (PC, MK)<br />
Urine microalbumin/creatinine ratio. (PC, MK)<br />
138
24-hour urine for protein and creatinine clearance. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient and their family about the management plan. (PC, CS)<br />
Counsel patients appropriately on dietary measures, exercise, medication adherence,<br />
proper foot care, and prevention <strong>of</strong> other target organ disease. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Finger-stick capillary blood glucose determination. (PC)<br />
Obtain an ABG. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Writing appropriate fluid and insulin orders and outline critical steps for the treatment <strong>of</strong><br />
DKA and DKH. (PC, MK)<br />
Counseling patients regarding basic features <strong>of</strong> ADA diabetic diet recommendations. (PC,<br />
CS)<br />
Instructing patients in home blood glucose monitoring. (PC, CS)<br />
Counseling patients on behavior changes (smoking cessation, medication adherence, poor<br />
glycemic control, obesity, hypertension, dyslipidemia, and infection) to avoid the<br />
complications <strong>of</strong> diabetes. (PC, CS)<br />
Counseling patients regarding basic foot care. (PC, CS)<br />
Determining when to institute diet therapy, oral hypoglycemic agents, and insulin therapy.<br />
(PC, MK)<br />
Calculating an appropriate insulin dose for a diabetic patient. (PC, MK)<br />
Using community resources (ADA, hospital and community-based education programs) to<br />
aid the patient in understanding and managing his or her illness. (PC, SBP)<br />
Determining when to obtain consultation from an endocrinologist, nephrologist,<br />
ophthalmologist, podiatrist, and dietician. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to diabetes mellitus. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate a commitment to meeting ADA clinical practice<br />
recommendations to insure quality diabetes care. (PLI, P, SBP)<br />
2. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based considerations in<br />
the selection diagnostic and therapeutic interventions for diabetes mellitus. (PLI, P)<br />
3. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for diabetes mellitus. (P)<br />
4. Respond appropriately to patients who are nonadherent to treatment for diabetes mellitus. (CS, P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding diabetes mellitus. (PLI, P)<br />
6. Appreciate the impact diabetes mellitus has on a patient’s quality <strong>of</strong> life, wellbeing, ability to work,<br />
and the family. (P)<br />
7. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essionals in the treatment <strong>of</strong> diabetes mellitus. (P, SBP)<br />
D. REFERENCES:<br />
139
The Diabetes Control and Complication Trail Research Group. The effect <strong>of</strong> intensive<br />
treatment <strong>of</strong> diabetes on the development and progression <strong>of</strong> long-term complications in<br />
insulin-dependent diabetes mellitus. N Engl JMed. 1993;329:977-86.<br />
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with<br />
sulphonylureas or insulin compared with conventional treatment and risk <strong>of</strong><br />
complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837-53.<br />
Clinical Practice Recommendations American Diabetes Association<br />
www.diabetes.org/for-health-pr<strong>of</strong>essionals-and-scientists/cpr.jsp<br />
Kitabchi AE. Wall BM. Management <strong>of</strong> diabetic ketoacidosis. Am Fam Physician.<br />
1999;60:455-64.<br />
140
TRAINING PROBLEM #21: DYSLIPIDEMIA<br />
RATIONALE:<br />
Dyslipidemia is a common, important, and treatable cardiovascular risk factor. Its pathophysiology is<br />
increasingly understood, diagnostic tests are readily available, and treatment modalities range from<br />
diet and exercise to a multitude <strong>of</strong> pharmacotherapies. Competency in the evaluation and<br />
management <strong>of</strong> this problem helps develop skills in rational test selection, patient education, and<br />
design <strong>of</strong> cost-effective treatment strategies. It also draws attention to the importance <strong>of</strong> community<br />
health education and nutrition.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy and physiology <strong>of</strong> the vascular system.<br />
Basic cholesterol and lipoprotein metabolism.<br />
Pathogenesis and pathophysiology <strong>of</strong> atherosclerosis.<br />
Pharmacology <strong>of</strong> bile acid sequestrants (resins), nicotinic acid, fibric acid derivatives, HMG-<br />
CoA reductase inhibitors (statins), and cholesterol absorption inhibitors (ezetimibe).<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1 The contribution <strong>of</strong> lipoproteins to atherogenesis and CAD risk, including the importance <strong>of</strong><br />
elevations in total cholesterol, LDL cholesterol, ratio <strong>of</strong> total to HDL cholesterol, and<br />
Lipoprotein a. (MK)<br />
2 The classification and etiologies <strong>of</strong> primary dyslipidemias. (MK)<br />
3 Etiologies and underlying pathophysiology <strong>of</strong> secondary dyslipidemias. (MK)<br />
4. The basic principles <strong>of</strong> the role <strong>of</strong> genetics in dyslipidemia, particularly familial combined<br />
hyperlipidemia. (MK)<br />
5. Screening recommendations for dyslipidemias in American adults. (MK)<br />
6. The importance <strong>of</strong> identifying and treating asymptomatic patients at high risk for CAD as<br />
aggressively as those with symptomatic disease. (MK)<br />
7. The available diagnostic studies and their use, particularly determinations <strong>of</strong> HDL, LDL, and total<br />
cholesterol, as well as the need to test for other cardiovascular risk factors. (MK)<br />
8. The current National Cholesterol Education Program (NCEP, ATP III) guidelines for risk factor<br />
assessment, diagnosis and management <strong>of</strong> dyslipidemias, including goal LDL cholesterol, goal<br />
non-HDL cholesterol, and the concept <strong>of</strong> coronary artery disease equivalent based on risk<br />
factors for coronary artery disease. (MK, PLI, SBP)<br />
9. Basic management <strong>of</strong> the common dyslipidemias, including diet, fiber, exercise, and<br />
risk/benefits/cost <strong>of</strong> drug therapy (statins, fibrates, ezetimide, nicotinic acid, resins). (MK)<br />
10. Diagnosis and implications <strong>of</strong> the “metabolic syndrome.” (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an age-<br />
141
appropriate medical history, that differentiates among etiologies <strong>of</strong> disease including:<br />
Prior patient or family history <strong>of</strong> dyslipidemia. (PC, CS)<br />
Other coronary risk factors. (PC, CS)<br />
Family history <strong>of</strong> early cardiovascular disease. (PC, CS)<br />
Dietary fat, saturated fat, fiber, cholesterol, and refined carbohydrate intake. (PC, CS)<br />
Exercise habits. (PC, CS)<br />
Alcohol use. (PC, CS)<br />
Past history <strong>of</strong> established CAD, cerebral vascular disease, and other vascular disease.<br />
(PC, CS)<br />
Presence <strong>of</strong> symptoms <strong>of</strong> angina and peripheral vascular disease. (PC, CS)<br />
History <strong>of</strong> renal, hepatic, or myopathic disease. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Blood pressure elevation. (PC)<br />
Xanthomata. (PC)<br />
Atherosclerotic fundoscopic changes. (PC)<br />
Carotid or femoral bruits. (PC, CS)<br />
Diminished peripheral pulses. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest primary or secondary<br />
causes <strong>of</strong> dyslipidemia. (PC, CS)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Fasting lipid pr<strong>of</strong>ile. (PC, MK)<br />
TSH (PC, MK)<br />
Fasting GLC, electrolytes, BUN/Cr. (PC, MK)<br />
Hepatic function panel. (PC, MK)<br />
CK. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Counsel patients about dietary measures to reduce cholesterol and saturated fats. (PC,<br />
CS)<br />
Counsel patients about ways to increase exercise. (PC, CS)<br />
Counsel patients about other modifiable cardiovascular risk factors. (PC, CS)<br />
6. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
An individual treatment plan that follows the NCEP ATP III guidelines. (PC, MK)<br />
Lifestyle modification (diet, exercise). (PC, MK)<br />
Appropriate pharmacologic interventions, including bile acid sequestrants (resins), nicotinic<br />
acid, fibric acid derivatives, HMG-CoA reductase inhibitors (statins), and cholesterol<br />
absorption inhibitors (ezetimibe). (PC, MK)<br />
Monitoring for adherence and side effects due to pharmacologic management. (PC, MK)<br />
142
Laboratory response to therapy. (PC, MK)<br />
Identifying barriers that prevent patients from adhering to recommended dietary, exercise,<br />
and pharmacologic plans. (PC, MK)<br />
Determining when to obtain consultation from an endocrinologist, or dietician. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to dyslipidemia. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1 Demonstrate a commitment to meeting NCEP ATP III guidelines to insure quality care <strong>of</strong><br />
patients with dyslipidemia. (PLI, P, SBP)<br />
2 Appreciate the importance <strong>of</strong> encouraging patients to assume responsibility for modifying their<br />
diet and increasing their exercise level. (P, CS)<br />
3 Appreciate the difficulties and frustrations that patients and health care providers face with<br />
recommended dietary changes. (P)<br />
4 Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for dyslipidemia. (PLI,<br />
P)<br />
5 Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for dyslipidemia. (P)<br />
6 Respond appropriately to patients who are nonadherent to treatment for dyslipidemia. (CS, P)<br />
7 Demonstrate ongoing commitment to self-directed learning regarding dyslipidemia. (PLI, P)<br />
8 Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essionals in the treatment <strong>of</strong> dyslipidemia. (P, SBP)<br />
D. REFERENCES:<br />
National Institutes <strong>of</strong> Health, National Heart, Lung, and Blood Institute National<br />
Cholesterol Education Program Clinical Practice Guidelines for Cholesterol<br />
Management in Adults (ATP III)<br />
www.nhlbi.nih.gov/about/ncep<br />
Grundy SM, Cleeman JI, Merz CN, et al; National Heart, Lung, and Blood Institute;<br />
American College <strong>of</strong> Cardiology Foundation; American Heart Association. Implications<br />
<strong>of</strong> recent clinical trials for the National Cholesterol Education Program Adult Treatment<br />
Panel III guidelines. Circulation. 2004;110:227-39.<br />
Ashen MD, Blumenthal RS. Clinical practice. Low HDL cholesterol levels. N Engl J<br />
Med. 2005;353:1252-60.<br />
Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J<br />
Med. 2005;352:1685-95.<br />
143
TRAINING PROBLEM #22: HEART FAILURE<br />
RATIONALE:<br />
Chronic heart failure (HF) is one <strong>of</strong> the most common cardiac problems encountered in clinical<br />
practice. Identification and correction <strong>of</strong> treatable underlying causes, control <strong>of</strong> precipitating factors<br />
and judicious use <strong>of</strong> multi-drug regimens for individuals with HF are important issues for third-year<br />
medical students.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> years should include:<br />
Knowledge <strong>of</strong> the structure and function <strong>of</strong> the heart and lungs.<br />
Understanding <strong>of</strong> the epidemiology <strong>of</strong> heart disease.<br />
Knowledge <strong>of</strong> the atherogenesis and pathophysiology <strong>of</strong> cardiovascular disease.<br />
Knowledge <strong>of</strong> the pharmacology <strong>of</strong> cardiovascular drugs.<br />
Ability to communicate appropriately with all types <strong>of</strong> patients including the elderly and those<br />
with diverse backgrounds.<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to perform a cardiovascular risk assessment and understand issues related to primary<br />
and secondary prevention <strong>of</strong> cardiovascular disease.<br />
Ability to understand the impact <strong>of</strong> illness on individuals and their families and, when<br />
appropriate, to address issues related to end-<strong>of</strong>-life care.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Types <strong>of</strong> processes and most common disease entities that cause HF (i.e. ischemic, valvular,<br />
hypertrophic, infiltrative, inflammatory, etc.). (MK)<br />
2. The basic role <strong>of</strong> genetics in certain forms <strong>of</strong> cardiomyopathy. (MK)<br />
3. Staging system for heart failure:<br />
Stage A: high risk for HF but no structural heart disease is present. (MK)<br />
Stage B: structural heart disease is present but never any symptoms. (MK)<br />
Stage C: past or current symptoms associated with structural heart disease. (MK)<br />
Stage D: end-stage disease with requirements for specialized treatment. (MK)<br />
4. Types <strong>of</strong> processes that cause systolic vs. diastolic dysfunction. (MK)<br />
5. Symptoms and signs <strong>of</strong> left-sided vs. right-sided heart failure. (MK)<br />
6. Compensatory mechanisms <strong>of</strong> heart failure including cardiac remodeling and activation <strong>of</strong><br />
endogenous neurohormonal systems. (MK)<br />
7. Factors leading to symptomatic exacerbation <strong>of</strong> HF, including ischemia, arrhythmias,<br />
hypoxemia, anemia, fever, hypertension, thyroid disorders, non-compliance with medications<br />
and dietary restrictions and use <strong>of</strong> nonsteroidal anti-inflammatory drugs. (MK)<br />
8. Importance <strong>of</strong> age, gender and ethnicity on the prevalence and<br />
prognosis <strong>of</strong> HF. (MK)<br />
9. Physiological basis and scientific evidence supporting each type<br />
<strong>of</strong> treatment, intervention, or procedure commonly used in the management <strong>of</strong> patients who<br />
present with HF. (MK)<br />
10. The general approach to the evaluation and treatment <strong>of</strong> atrial<br />
144
fibrillation (MK)<br />
11. Role <strong>of</strong> critical pathways or practice guidelines in delivering<br />
high-quality, cost effective care for patients presenting with new or recurrent heart failure. (PC,<br />
SBP)<br />
12. The Centers for Medicare & Medicaid Services (CMS) and the<br />
Joint Commission on the Accreditation <strong>of</strong> Healthcare Organizations (JCAHO) quality measures<br />
for HF treatment. (MK, PLI, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, including:<br />
Differentiating between various etiologies <strong>of</strong> heart failure (answers the question: Why is the<br />
patient in heart failure?). (PC, CS)<br />
Identifying clinical factors responsible for symptomatic exacerbation (answers the question:<br />
Why is the patient worse now?). (PC, CS)<br />
Exercise intolerance (fatigue, dyspnea on exertion). (PC, CS)<br />
Fluid retention (peripheral edema, dyspnea). (PC, CS)<br />
Changes in sleep pattern (orthopnea, paroxysmal nocturnal dyspnea [PND], nocturia). (PC,<br />
CS)<br />
Assessing the functional capacity <strong>of</strong> patients with HF (walking distance, New York Heart<br />
classification). (PC, CS)<br />
Cardiac risk factors. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a focused physical exam to<br />
help establish the diagnosis <strong>of</strong> HF and estimate its severity:<br />
Measurement <strong>of</strong> vital signs including weight and respiratory rate/pattern. (PC)<br />
Accurate measurement <strong>of</strong> arterial blood pressure and recognition <strong>of</strong> the typical blood<br />
pressure findings that occur in patients with aortic stenosis, aortic insufficiency and pulsus<br />
paradoxus. (PC)<br />
Assessment <strong>of</strong> major arterial pulses for abnormalities, including bruits. (PC)<br />
Assessment <strong>of</strong> the neck veins for jugular venous distention and, when necessary,<br />
evaluation for abdominal jugular reflux. (PC)<br />
Assessment <strong>of</strong> the conjunctiva and optic fundus. (PC)<br />
Assessment <strong>of</strong> the extremities to ascertain for skin conditions, including color, temperature<br />
and the presence <strong>of</strong> edema, cyanosis or clubbing. (PC)<br />
Assessment <strong>of</strong> the lungs for crackles, rhonchi and decreased breath sounds. (PC)<br />
Inspection and palpation <strong>of</strong> the anterior chest to identify right and left sided heaves, lifts and<br />
thrills. (PC)<br />
Auscultation <strong>of</strong> the heart to determine rhythm, intensity <strong>of</strong> heart sounds, splitting <strong>of</strong> S2 and<br />
the presence <strong>of</strong> rubs, gallops (S3, S4, summation) or extra heart sounds (e.g. clicks). (PC)<br />
Auscultation <strong>of</strong> the heart to detect the presence <strong>of</strong> heart murmurs; when a murmur is<br />
present, students should be able to:<br />
o Identify timing (systolic vs. diastolic, holosystolic vs. ejection). (PC)<br />
o Describe pitch, location and pattern <strong>of</strong> radiation. (PC)<br />
o Gauge significance (innocent vs. pathologic, sclerosis vs. stenosis). (PC)<br />
Assessment <strong>of</strong> the abdomen to determine the presence <strong>of</strong> hepatomegaly,<br />
ascites, abnormal pulsations and bruits. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
145
diagnosis and recognize specific history, physical exam and/or laboratory findings that:<br />
Help support or refute a clinical diagnosis <strong>of</strong> heart failure. (PC, MK)<br />
Distinguish between various underlying etiologies <strong>of</strong> HF, including disease processes that<br />
primarily affect:<br />
o Pericardium (constrictive pericarditis, pericardial tamponade). (PC, MK)<br />
o Endocardium (valvular [congenital, acquired], endocarditis). (PC, MK)<br />
o Myocardium (hypertrophic, restrictive, congestive). (PC, MK)<br />
4. Laboratory interpretation: Students should be able interpret specific diagnostic tests and<br />
procedures that are commonly ordered to evaluate patients who present with heart failure.<br />
Test interpretation should take into account: Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
12-lead ECG. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
B-type natriuretic peptide. (PC, MK)<br />
Students should be able to define the indications for, and interpret (with consultation) the<br />
results <strong>of</strong> the following diagnostic tests and procedures:<br />
Echocardiography. (PC, MK)<br />
Treadmill and nuclear exercise testing. (PC, MK)<br />
Radionuclide ventriculogram. (PC, MK)<br />
Cardiac. (PC, MK)<br />
Coronary angiography. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, prognosis and treatment plan to the patient and his or her<br />
family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Educate patients about cardiovascular risk factors. (PC, CS)<br />
Council patients regarding a sodium-restricted diet. (PC, CS)<br />
Address palliative care and end-<strong>of</strong>-life issues with patients who have<br />
intractable symptoms associated with end-stage heart failure. (PC, CS, P)<br />
6. Basic and advanced procedural skills: students should be able to:<br />
Perform a 12-lead ECG. (PC)<br />
Obtain an ABG. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Recognize the importance <strong>of</strong> early detection and treatment <strong>of</strong> risk factors that may lead to<br />
the development <strong>of</strong> heart failure. (PC)<br />
Identifying the indications, contraindications, mechanisms <strong>of</strong> action, adverse reactions,<br />
significant interactions, and relative costs <strong>of</strong> the following treatments/interventions:<br />
o Non-pharmacological management. (PC, MK)<br />
-Sodium restriction. (PC, MK)<br />
-Physical activity and limitations. (PC, MK)<br />
o Pharmacological management (recommended for routine use). (PC, MK)<br />
-Diuretics. (PC, MK)<br />
-ACE-I/ARB. (PC, MK)<br />
-Beta-blockers. (PC, MK)<br />
-Aldosterone antagonists (spironolactone, eplerenone). (PC, MK)<br />
-digoxin. (PC, MK)<br />
o Interventions considered for use in selected patients. (PC, MK)<br />
-Hydralazine and isosorbide dinitrate. (PC,MK)<br />
146
-Angoitensin receptor blockers. (PC, MK)<br />
-Calcium channel blockers. (PC, MK)<br />
-Anti-arrhythmic agents. (PC, MK)<br />
-Anticoagulants/anti a thrombotic agents. (PC, MK)<br />
o other modalities(PC, MK)<br />
-Coronary revascularization. (PC, MK)<br />
-Synchronized biventricular pacing. (PC, MK)<br />
-Implantable cardiac defibrillators. (PC, MK)<br />
Developing a timely and appropriate evaluation and treatment plan for patients with heart<br />
failure due to diastolic dysfunction, including:<br />
o Control <strong>of</strong> physiologic factors (blood pressure, heart rate). (PC, MK)<br />
o Reduction in central blood volume by judicious use <strong>of</strong> diuretics. (PC, MK)<br />
o Alleviation <strong>of</strong> myocardial ischemia. (PC, MK)<br />
o Use <strong>of</strong> calcium channel blockers. (PC, MK)<br />
Describing use <strong>of</strong> other agents and interventions that may be useful in treating patients with<br />
refractory, end-stage heart failure:<br />
o Intravenous vasodilators. (PC, MK)<br />
o Intravenous positive inotropic agents. (PC, MK)<br />
o Infusion <strong>of</strong> B-type natriuretic peptide (nesiritide). (PC, MK)<br />
o Ventricular assist devices. (PC, MK)<br />
o Heart transplantation. (PC, MK)<br />
Defining and describing how the diagnosis and treatment <strong>of</strong> HF in special<br />
populations may differ (e.g. very elderly, associated co-morbidities). (PC, MK)<br />
Demonstrating how critical pathways or practice guidelines in ambulatory or hospitalized<br />
patients with HF can be used to guide diagnostic test ordering and medical decision<br />
making. (PC, PLI, SBP)<br />
Determining when to consult a cardiologist. (PC, SBP)<br />
Identifying when palliative care may be appropriate for patients with refractory symptoms<br />
associated with end-stage disease. (PC)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to HF. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for HF. (PLI, P)<br />
2. Recognize the significant morbidity and mortality associated with HF (P)<br />
3. Recognize the impact <strong>of</strong> lifestyle limitations caused by HF. (P)<br />
4. Respond appropriately to patients who are non-adherent to treatment for HF. (CS, P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding heart failure. (PLI, P)<br />
6. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> heart failure. (P, SBP)<br />
7. Appreciate the importance <strong>of</strong> and demonstrate a commitment to meeting national health care<br />
quality measures for the treatment <strong>of</strong> HF. (PLI, P, SBP)<br />
147
D. REFERENCES:<br />
ACC/AHA 2005 guideline update for the diagnosis and management <strong>of</strong> chronic<br />
heart failure in the adult: a report <strong>of</strong> the American College <strong>of</strong> Cardiology/American<br />
Heart Association Task Force on Practice Guidelines (Writing Committee to<br />
Update the 2001 Guidelines for the Evaluation and Management <strong>of</strong> Heart Failure).<br />
J Am Coll Cardiol. 2005;46:1116-43.<br />
http://www.acc.org/clinical/guidelines/failure/update/index.pdf<br />
Cook DJ, Simel DL. Does this patient have abnormal central venous pressure? JAMA.<br />
1996; 275: 630-634.<br />
Wang CS. FitzGerald JM. Schulzer M. Mak E. Ayas NT. Does this dyspneic patient in<br />
the emergency department have congestive heart failure? JAMA. 2005;294:1944-56.<br />
Doust JA. Glasziou PP. Pietrzak E. Dobson AJ. A systematic review <strong>of</strong> the diagnostic<br />
accuracy <strong>of</strong> natriuretic peptides for heart failure. Arch Intern Med. 2004;164:1978-84.<br />
Yan AT. Yan RT. Liu PP. Narrative review: pharmacotherapy for chronic heart failure:<br />
evidence from recent clinical trials. Ann Intern Med. 2005;142(2):132-45.<br />
Aurigemma GP. Gaasch WH. Clinical practice. Diastolic heart failure. N Engl J Med.<br />
2004;351:1097-105.<br />
148
TRAINING PROBLEM #23: HIV INFECTION<br />
RATIONALE:<br />
HIV infection and AIDS represent one <strong>of</strong> the most difficult challenges in clinical medicine today. An<br />
HIV specialist (usually an infectious diseases physician) cares for the vast majority <strong>of</strong> patients with<br />
HIV infection and AIDS. Given that there is no proven cure, this remains an important training<br />
problem for third year medical students. The enormous and continuously evolving complexities <strong>of</strong><br />
antiretroviral treatment are generally beyond the level <strong>of</strong> the third year medical student and for that<br />
matter most general internists. Rather, an approach to HIV infection, AIDS, and its most common<br />
and serious complications are stressed.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> the worldwide epidemiology, biology, and immunology <strong>of</strong> HIV.<br />
Microbiology <strong>of</strong> common opportunistic organisms.<br />
Pharmacology <strong>of</strong> antimicrobial agents and antiretrovirals.<br />
Understanding <strong>of</strong> universal precautions.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Symptoms and signs <strong>of</strong> acute HIV seroconversion. (MK)<br />
2. CDC AIDS case definition. (MK)<br />
3. Specific tests for HIV (e.g. HIV ELISA, confirmatory western blot, quantitative PCR) and their<br />
operating characteristics. (MK)<br />
4. Relationship <strong>of</strong> CD4 lymphocyte count to opportunistic infections as well as relationship between<br />
CD4 lymphocyte count and viral load to overall disease progression. (MK)<br />
5. The basic principles <strong>of</strong> highly active antiretroviral therapy (HAART), including the different classes<br />
<strong>of</strong> antiviral medications and their use, as well as common side effects and drug-drug<br />
interactions. (MK)<br />
6. Basics <strong>of</strong> post-exposure prophylaxis. (MK)<br />
7. The marked importance <strong>of</strong> antiretroviral medication adherence and the potential consequences <strong>of</strong><br />
erratic or poor adherence. (MK)<br />
8. Vaccination recommendation for patients infected with HIV. (MK)<br />
9. Indications for and utility and risks <strong>of</strong> prophylaxis <strong>of</strong> HIV-related opportunistic infections. (MK)<br />
10. Pathogenesis, symptoms, signs, typical clinical course, and management <strong>of</strong> HIV-related<br />
opportunistic infections with a recognition <strong>of</strong> which are most common:<br />
Pneumocystis jiroveci. (MK)<br />
Candidiasis (oral, esophageal, vaginal). (MK)<br />
Cryptococcus ne<strong>of</strong>ormans. (MK)<br />
Cryptosporidium parvum. (MK)<br />
Cytomegalovirus infection (gastrointestinal, neurologic, retinal). (MK)<br />
Varicella-zoster virus. (MK)<br />
Isospora belli. (MK)<br />
149
Microsporidiosis. (MK)<br />
Mycobacterium avium complex. (MK)<br />
Mycobacterium tuberculosis. (MK)<br />
Toxoplasma gondii. (MK)<br />
11. Symptoms and signs <strong>of</strong> the following HIV-related malignancies:<br />
Kaposi’s sarcoma. (MK)<br />
Non-Hodgkin’s lymphoma. (MK)<br />
Cervical carcinoma. (MK)<br />
12. Common skin and oral manifestations <strong>of</strong> HIV infection and AIDS:<br />
Molluscum contagiosum. (MK)<br />
Cryptococcus ne<strong>of</strong>ormans. (MK)<br />
Viral warts. (MK)<br />
Lipodystrophy. (MK)<br />
Herpes zoster. (MK)<br />
Seborrhoeic dermatitis. (MK)<br />
Buccal candidiasis. (MK)<br />
Oral hairy leukoplakia. (MK)<br />
13. “Safe sex” practices (MK)<br />
14. The importance <strong>of</strong> proper ongoing dental care. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
HIV infection risk factors. (PC, CS)<br />
Sexual contacts. (PC, CS)<br />
Parenteral exposure to infected blood by needle sharing or transfusion. (PC, CS)<br />
Occupational exposures. (PC, CS)<br />
Other sexually transmitted diseases. (PC, CS)<br />
Tuberculosis exposure. (PC, CS)<br />
Prior HIV serology results, CD4 lymphocyte count and viral load. (PC, CS)<br />
Prior HIV-related opportunistic infections. (PC, CS)<br />
Current/prior antiretroviral medications and their side effects. (PC, CS)<br />
Fever, sweats, anorexia, unintentional weight loss, rash/skin lesions, lymphadenopathy.<br />
(PC, CS)<br />
Cough, sputum production, dyspnea, chest pain. (PC, CS)<br />
Headache, altered mental status, psychiatric complaints. (PC, CS)<br />
Odynophagia, dysphagia. (PC, CS)<br />
Vaginal discharge, history <strong>of</strong> cervical dysplasia or neoplasia. (PC, CS)<br />
Diarrhea. (PC, CS)<br />
Visual changes. (PC, CS)<br />
A dietary history to determine caloric intake. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
General appearance regarding atrophy/wasting/cachexia. (PC)<br />
Complete neurologic examination. (PC)<br />
150
Mental status examination. (PC)<br />
Fundoscopic examination. (PC)<br />
Lymph node examination. (PC)<br />
Skin and oral examination. (PC)<br />
Pelvic and male genital examination. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology in an<br />
potentially or known HIV-infected patient for the following:<br />
Fever. (PC, MK)<br />
Unintentional weight loss/wasting/cachexia. (PC, MK)<br />
Lymphadenopathy. (PC, MK)<br />
Rash and skin lesions. (PC, MK)<br />
Cough, sputum production, dyspnea, abnormal chest radiography. (PC, MK)<br />
Diarrhea, odynophagia, dysphagia. (PC, MK)<br />
Altered mental status and psychiatric changes. (PC, MK)<br />
Headache. (PC, MK)<br />
Oral lesions. (PC, MK)<br />
Visual/retinal abnormalities. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Specific tests for HIV (e.g. HIV ELISA, confirmatory western blot, quantitative PCR). (PC,<br />
MK)<br />
CD4 lymphocyte count. (PC, MK)<br />
CBC with differential. (PC, MK)<br />
Sputum staining and cultures. (PC, MK)<br />
Blood cultures. (PC, MK)<br />
Cerebrospinal fluid analysis (color, opening pressure, chemistries, cell counts, staining,<br />
cultures, cytology, cryptococcal antigen, VDRL,<br />
Ebstein Barr virus, cytomegalovirus, toxoplasmosis, JC virus). (PC, MK)<br />
Stool for ova and parasites, cryptosporium, isospora, microsporidia, cytomegalovirus<br />
antigen. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
results <strong>of</strong>:<br />
Chest CT. (PC, MK)<br />
Cranial CT. (PC, MK)<br />
Cranial MRI. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit input and questions from the patient and his or her family about the management<br />
plan. (PC, CS)<br />
counsel and educate patients about HIV exposure prevention (PC, CS)<br />
Counsel an exposed patient about seroconversion rates and, in appropriate situations, the<br />
availability <strong>of</strong> post-exposure prophylaxis. (PC, CS)<br />
151
Counsel and educate patients about complications <strong>of</strong> HIV drug therapy, drug-drug<br />
interactions, and the marked importance <strong>of</strong> adherence. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Obtain blood cultures. (PC)<br />
Obtain an ABG. (PC)<br />
Place and interpret a PPD. (PC)<br />
Assist in performing a lumbar puncture after explaining the procedure to the patient. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Ordering appropriate laboratory tests. (PC, MK)<br />
Advising patients regarding HIV transmission prevention. (PC, MK)<br />
Insuring antiretroviral adherence. (PC, MK)<br />
Following parameters <strong>of</strong> disease progression/activity. (e.g. CD4 lymphocyte count, viral<br />
load). (PC, MK)<br />
Monitoring for the development <strong>of</strong> side effects from antiretroviral treatment and drug-drug<br />
interactions. (PC, MK)<br />
Insuring the administration <strong>of</strong> appropriate vaccinations. (PC, MK)<br />
Assessing PPD status. (PC, MK)<br />
Prescribing and monitoring appropriate opportunist infection prophylaxis. (PC, MK)<br />
Ordering nutritional supplements to manage and prevent malnutrition. (PC, MK)<br />
Assisting in the procurement <strong>of</strong> proper and ongoing dental care. (PC, MK)<br />
Identifying and recommending community health care resources available for the care <strong>of</strong><br />
AIDS patients. (PC, SBP)<br />
Determining when to obtain consultation from an infectious diseases specialist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to HIV infection and AIDS. (PC, PLI)<br />
Incorporating patient need and preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Appreciate the bioethical, social, and legal issues concerning patient confidentiality <strong>of</strong> HIV<br />
infection. (PC, CS)<br />
2. Demonstrate a nonjudgmental attitude regarding the mode <strong>of</strong> HIV acquisition. (P)<br />
3 Appreciate the sometimes severe social stigma <strong>of</strong> HIV infection and AIDS. (P)<br />
4 Show respect <strong>of</strong> “alternative lifestyles.” (P)<br />
5 Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for HIV infection and<br />
AIDS. (PLI, P)<br />
6 Recognize the importance <strong>of</strong> patient needs and preferences when selecting among diagnostic<br />
and therapeutic options for patients with HIV infection or AIDS. (P)<br />
7 Respond appropriately to patients who are nonadherent to antiretroviral treatment. (CS, P)<br />
8 Demonstrate ongoing commitment to self-directed learning regarding HIV infection and AIDS.<br />
(PLI, P)<br />
9 Appreciate the impact HIV infection and AIDS have on a patient’s quality <strong>of</strong> life, well-being,<br />
ability to work, and the family. (P)<br />
10 Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other health<br />
care pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> HIV infection and AIDS. (P, SBP)<br />
152
D. REFERENCES:<br />
Guidelines for preventing Opportunistic Infections Among HIV-Infected Persons-2002.<br />
Recommendations <strong>of</strong> the U.S. Public Health Service and the Infectious Diseases Society <strong>of</strong><br />
America. MMWR 51(RR-08);1-60. Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/mmwr/PDF/RR/RR5108.pdf<br />
Guidelines for Using Antiretroviral Agents Among HIV-Infected Adults and Adolescents-<br />
2002. Recommendations <strong>of</strong> the Panel on Clinical Practices for Treatment <strong>of</strong> HIV. MMWR<br />
51(RR-07);1-64.<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/mmwr/PDF/RR/RR5107<br />
Aberg JA, Gallant JE, Anderson J, Oleske JM, Libman H, Currier JS, Stone VE, Kaplan,<br />
JE. Primary care guideline for the management <strong>of</strong> persons infected with human<br />
immunodeficiency virus: recommendation <strong>of</strong> the HIV <strong>Medicine</strong> Association <strong>of</strong> the Infectious<br />
Diseases Society <strong>of</strong> America. Clin Infect Dis. 2004;39:609-29.<br />
www.journals.uchicago.edu/CID/journal/issues/v39n5/34135/34135.web.p df<br />
www.guideline.gov/summary/summary.aspx?view_id=1&doc_id=5625<br />
AIDSinfo National Institutes <strong>of</strong> Health<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.aidsinfo.nih.gov<br />
Divisions <strong>of</strong> HIV/AIDS Prevention National Center for HIV, STD and TB Prevention Centers<br />
for Disease Control and Prevention U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/hiv/dhap.htm<br />
Hammer SM. Management <strong>of</strong> newly diagnosed HIV infection. N Engl J Med.<br />
2005;353:1702-10.<br />
153
TRAINING PROBLEM #24: HYPERTENSION<br />
RATIONALE:<br />
As many as 50 million Americans have elevated blood pressure (systolic pressure 140 mmHg or<br />
greater and/or diastolic blood pressure 90 mmHg or greater) or are taking antihypertensive<br />
medication. Nonfatal and fatal cardiovascular disease (CVD)— including coronary heart disease<br />
(CHD), peripheral vascular disease, stroke and renal disease—all increase progressively with higher<br />
levels <strong>of</strong> both systolic (SBP) and diastolic (DBP) blood pressure levels. These relationships are<br />
strong, continuous, independent, predictive and etiologically significant, and indicate that reduction <strong>of</strong><br />
blood pressure reduces these risks.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-clinical years should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> the pathogenesis and pathophysiology <strong>of</strong> hypertension.<br />
Knowledge <strong>of</strong> the epidemiology and risk factors for hypertension.<br />
Understanding <strong>of</strong> the pharmacologic management <strong>of</strong> acute and chronic hypertension.<br />
Understanding the behavioral issues by sex, race, culture, and age that relate to the<br />
management and treatment <strong>of</strong> hypertension.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe and discuss:<br />
1. The etiologies and relative prevalence <strong>of</strong> primary and secondary hypertension. (MK)<br />
2. The basic principles <strong>of</strong> the role <strong>of</strong> genetics in hypertension. (MK)<br />
3. The definition <strong>of</strong> hypertensive urgency and emergency, citing examples <strong>of</strong> both. (MK)<br />
4. The difference between essential (primary) and secondary hypertension. (MK)<br />
5. Symptoms and signs <strong>of</strong> the following disorders associated with secondary hypertension:<br />
Renovascular hypertension. (MK)<br />
Renal failure. (MK)<br />
Polycystic kidney disease. (MK)<br />
Cushing’s disease or syndrome. (MK)<br />
Hyperaldosteronism. (MK)<br />
Hyperthyroidism. (MK)<br />
Hypercalcemia. (MK)<br />
Medication, alcohol, and illicit drug use. (MK)<br />
Coarctation <strong>of</strong> the aorta. (MK)<br />
Sleep apnea. (MK)<br />
6. The manifestations <strong>of</strong> target-organ disease due to hypertension. (MK)<br />
7. Classification <strong>of</strong> blood pressure (SBP and DBP for all age 18 or older). (MK)<br />
8. Basic approaches to the pharmacological management <strong>of</strong> acute and chronic hypertension,<br />
including the physiologic basis and scientific evidence supporting these approaches, and<br />
causes for lack <strong>of</strong> responsiveness to therapy. (MK)<br />
9. Prevention strategies for reducing hypertension (including lifestyle factors, such as dietary<br />
intake <strong>of</strong> sodium, weight, and exercise level), and explain the physiologic basis and/or<br />
154
scientific evidence supporting each strategy. (MK)<br />
10. Steps in management <strong>of</strong> patients with a hypertensive emergency. (MK)<br />
11. Factors that contribute to non-adherence with antihypertensive medications. (MK)<br />
B. SKILLS: Students should demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Duration and levels <strong>of</strong> elevated blood pressure. (PC, CS)<br />
History <strong>of</strong> symptoms <strong>of</strong> cardiovascular, cerebrovascular, peripheral vascular or renal<br />
disease; diabetes; dyslipidemia; or gout. (PC, CS)<br />
History <strong>of</strong> symptoms suggesting secondary hypertension. (PC, CS)<br />
History <strong>of</strong> weight gain, leisure-time physical activities, and smoking or other tobacco use.<br />
(PC, CS)<br />
Family history <strong>of</strong> high blood pressure, premature CHD, stroke, CVD, diabetes mellitus and<br />
dyslipidemia. (PC, CS)<br />
Psychosocial and environmental factors that may elevate blood pressure (family situation,<br />
employment status, working conditions, education level). (PC, CS)<br />
Dietary assessment, including sodium intake and intake <strong>of</strong> saturated fat and cholesterol.<br />
(PC, CS)<br />
Results and side effects <strong>of</strong> previous antihypertensive therapy. (PC, CS)<br />
Use <strong>of</strong> commonly prescribed, over-the -counter, and illicit medications that may raise blood<br />
pressure or interfere with the effectiveness <strong>of</strong> antihypertensive medications. (PC, CS)<br />
Alcohol intake. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Blood pressure measurements to detect and confirm the presence <strong>of</strong> high blood pressure.<br />
(PC)<br />
Examination <strong>of</strong> the fundus for arteriolar narrowing, arteriovenous nicking, hemorrhages,<br />
exudates, or papilledema. (PC)<br />
Neck for carotid bruits, distended veins, or an enlarged thyroid gland. ((PC)<br />
Heart for increased rate, increased size, precordial heave, clicks, murmurs, arrhythmias,<br />
and third (S3) and fourth (S4) sounds. (PC)<br />
Abdomen for bruits, enlarged kidneys, masses, and abnormal aortic pulsation. (PC)<br />
Extremities for diminished, delayed, or absent peripheral arterial pulsations, bruits, and<br />
edema. (PC)<br />
Peripheral pulses specifically femoral arterial pulses. (PC)<br />
Body habitus, looking for changes associated with secondary hypertension. (PC)<br />
Peripheral and central nervous system for ischemic changes. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
diagnosis recognizing specific history, physical exam, and laboratory findings that suggest a<br />
specific etiology <strong>of</strong> hypertension. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend and interpret<br />
diagnostic and laboratory tests, both prior to and after initiating treatment based on the<br />
differential diagnosis, including consideration <strong>of</strong> test cost and performance characteristics as<br />
well as patient preferences. Laboratory and diagnostic tests should include, when appropriate:<br />
UA. (PC, MK)<br />
CBC. (PC, MK)<br />
Blood glucose (fasting if possible). (PC, MK)<br />
155
Electrolytes, BUN/Cr. (PC, MK)<br />
Uric acid. (PC, MK)<br />
Fasting lipid pr<strong>of</strong>ile. (PC, MK)<br />
ECG. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan and prognosis <strong>of</strong> the disease to the patient and<br />
his or her family, taking into account the patient’s knowledge <strong>of</strong> hypertension and his or her<br />
preferences regarding treatment options. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Educate patients about hypertension risk factors, taking into account:<br />
o Demographics. (PC, CS)<br />
o Concomitant diseases and therapies. (PC, CS)<br />
o Quality <strong>of</strong> life. (PC, CS)<br />
o Physiologic and biochemical measurements. (PC, CS)<br />
o Economic considerations. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to perform:<br />
UA (dipstick and microscopic). (PC)<br />
12-lead ECG. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Treating acute and chronic hypertension. (PC, MK)<br />
Treating primary (essential) hypertension versus secondary hypertension. (PC, MK)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Prescribing preventative strategies to diminish hypertension, including:<br />
o Weight reduction. (PC, MK)<br />
o Moderation <strong>of</strong> alcohol intake. (PC, MK)<br />
o Regular physical activity. (PC, MK)<br />
o Reduction <strong>of</strong> sodium intake. (PC, MK)<br />
o Increase in potassium intake. (PC, MK)<br />
o Smoking cessation. (PC, MK)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to hypertension. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Appreciate the importance <strong>of</strong> patient preferences and adherence with management plans for<br />
those with hypertension. (P)<br />
2. Recognize the responsibility <strong>of</strong> the physician with regard to non-adherence. (P)<br />
3. Respond appropriately to patients who are non-adherent to treatment for hypertension. (CS, P)<br />
4. Appreciate how preventative strategies may diminish need for medications. (P)<br />
5. Appreciate the importance <strong>of</strong> side effects <strong>of</strong> medications and their impact on quality <strong>of</strong> life and<br />
adherence (including those side effects to which the geriatric population may be more prone)<br />
and demonstrate a commitment to limiting the whenever possible. (P)<br />
6. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for hypertension.<br />
(PLI, P)<br />
7. Demonstrate ongoing commitment to self-directed learning regarding hypertension. (PLI, P)<br />
8. Appreciate the impact hypertension has on a patient’s quality <strong>of</strong> life, wellbeing, ability to work,<br />
156
and the family. (P)<br />
9. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> hypertension. (P, SBP)<br />
D. REFERENCES:<br />
Chobanian, AV, Bakris, GL, Black, HR, et al. The seventh report <strong>of</strong> the joint national<br />
committee on prevention, detection, evaluation, and treatment <strong>of</strong> high blood pressure:<br />
the JNC 7 report. JAMA. 2003; 289:2560-72.<br />
www.nhlbi.nih.gov/guidelines/hypertension/jncintro.htm<br />
Major cardiovascular events in hypertensive patients randomized to doxazosin vs<br />
chlorthalidone: the antihypertensive and lipid-lowering treatment to prevent<br />
heart attack trial (ALLHAT). ALLHAT Collaborative Research Group. JAMA.<br />
2000;283:1967-75.<br />
ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. The<br />
Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major<br />
outcomes in high-risk hypertensive patients randomized to angiotensin-converting<br />
enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-<br />
Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981-97.<br />
Davis BR, Furberg CD, Wright JT Jr, Cutler JA, Whelton P. ALLHAT Collaborative<br />
Research Group. ALLHAT: setting the record straight. Ann Intern Med. 2004;141:39-<br />
46.<br />
Eisenberg MJ, Brox A, Bestawros AN. Calcium channel blockers: an update. Am J<br />
Med. 2004;116:35-43.<br />
Wing LM, Reid CM, Ryan P, et al. Second Australian National Blood Pressure Study<br />
Group. A comparison <strong>of</strong> outcomes with angiotensin-converting--enzyme inhibitors and<br />
diuretics for hypertension in the elderly. N Engl J Med. 2003;348:583-92.<br />
Agodoa LY, Appel L, Bakris GL, et al. African American Study <strong>of</strong> Kidney Disease and<br />
Hypertension (AASK) Study Group. Effect <strong>of</strong> ramipril vs amlodipine on renal outcomes<br />
in hypertensive nephrosclerosis: a randomized controlled trial. JAMA. 2001;285:2719-<br />
28.<br />
Brenner BM, Cooper ME, de Zeeuw D, et al. RENAAL Study Investigators. Effects <strong>of</strong><br />
losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and<br />
nephropathy. N Engl J Med. 2001;345:861-9.<br />
Lewis EJ, Hunsicker LG, Clarke WR, et al. Collaborative Study Group. Renoprotective<br />
effect <strong>of</strong> the angiotensin-receptor antagonist irbesartan in patients with nephropathy due<br />
to type 2 diabetes. N Engl J Med. 2001;345:851-60.<br />
Tuomilehto J, Rastenyte D, Birkenhager WH, et al. Effects <strong>of</strong> calcium-channel blockade<br />
in older patients with diabetes and systolic hypertension. Systolic Hypertension in<br />
Europe Trial Investigators. N Engl J Med. 1999;340:677-84.<br />
Anonymous. Tight blood pressure control and risk <strong>of</strong> macrovascular and microvascular<br />
complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group.<br />
BMJ. 1998;317:703-13.<br />
Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects <strong>of</strong> an angiotensinconverting-enzyme<br />
inhibitor, ramipril, on cardiovascular events in high-risk patients. The<br />
Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med.<br />
2000;342:145-53.<br />
Dahl<strong>of</strong> B, Devereux RB, Kjeldsen SE, et al. LIFE Study Group. Cardiovascular<br />
morbidity and mortality in the Losartan Intervention For Endpoint reduction in<br />
hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359:995-<br />
157
1003.<br />
158
TRAINING PROBLEM #25: LIVER DISEASE<br />
RATIONALE:<br />
The causes <strong>of</strong> hepatobiliary disease are many and can be quite overwhelming to the internal<br />
medicine clerk. A thorough understanding <strong>of</strong> a systematic approach to hyperbilirubinemia/jaundice is<br />
by far preferable to random knowledge <strong>of</strong> highly specific etiologies. The liver responds pathologically<br />
to injury in characteristic ways and knowledge <strong>of</strong> these patterns can also be very useful in differential<br />
diagnosis. Several etiologies <strong>of</strong> liver disease such as acute/chronic viral hepatitis and alcoholinduced<br />
liver disease are sufficiently common as to require specific attention. In addition, many liver<br />
diseases can result in cirrhosis and its complications and, therefore, understanding this end-stage<br />
development is important.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy, physiology, and pathophysiology <strong>of</strong> the hepatobiliary system.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The biochemical/physiologic/mechanistic approach to hyperbilirubinemia, including:<br />
Increased production. (MK)<br />
Decreased hepatocyte uptake. (MK)<br />
Decreased conjugation. (MK)<br />
Decreased excretion from the hepatocyte. (MK)<br />
Decreased small duct transport (intrahepatic cholestasis). (MK)<br />
Decreased large duct transport (extrahepatic cholestasis, obstructive jaundice). (MK)<br />
2. The biochemistry and common causes <strong>of</strong> unconjugated and conjugated hyperbilirubinemia.<br />
(MK)<br />
3. The use <strong>of</strong> serum markers <strong>of</strong> liver injury (e.g. AST, ALT, GGT, Alk Phos) and function (e.g.<br />
bilirubin, ALB, PT/INR) in the diagnostic evaluation <strong>of</strong> hepatobiliary disease. (MK)<br />
4. The clinical significance <strong>of</strong> asymptomatic, isolated elevation <strong>of</strong> AST, ALT, GGT, and/or Alk<br />
Phos. (MK)<br />
5. The common pathologic patterns <strong>of</strong> liver disease and their common causes, including:<br />
Steatosis (fatty liver). (MK)<br />
Hepatitis. (MK)<br />
Cirrhosis. (MK)<br />
Infiltrative. (MK)<br />
Intrahepatic cholestasis. (MK)<br />
Extrahepatic cholestasis (obstructive jaundice). (MK)<br />
6. The epidemiology, symptoms, signs, typical clinical course, and prevention <strong>of</strong> viral hepatitis.<br />
(MK)<br />
7. The distinctions between acute and chronic hepatitis. (MK)<br />
8. The indications for and efficacy <strong>of</strong> hepatitis A and B vaccinations. (MK)<br />
9. The common causes and clinical significance <strong>of</strong> hepatic steatosis and steatohepatis. (MK)<br />
159
10. The epidemiology, symptoms, signs, and typical clinical course <strong>of</strong> autoimmune liver diseases<br />
such as autoimmune hepatitis, primary biliary cirrhosis, and primary sclerosing cholangitis.<br />
(MK)<br />
11. The epidemiology, symptoms, signs, and typical clinical course <strong>of</strong> cirrhosis. (MK)<br />
12. The pathophysiologic manifestations, symptoms, signs, and complications <strong>of</strong> alcohol-induced<br />
liver disease. (MK)<br />
13. The symptoms, signs, and complications <strong>of</strong> portal hypertension. (MK)<br />
14. The pathophysiology and common causes <strong>of</strong> ascites. (MK)<br />
15. The pathophysiologic manifestations, symptoms, and signs <strong>of</strong> spontaneous bacterial<br />
peritonitis. (MK)<br />
16. The basic pathophysiology, symptoms, signs, typical clinical course, and precipitants <strong>of</strong><br />
hepatic encephalopathy. (MK)<br />
17. The basic pathophysiology, symptoms, signs, and typical clinical course <strong>of</strong> the hepatorenal<br />
syndrome. (MK)<br />
18. The analysis <strong>of</strong> ascitic fluid and its use in the diagnostic evaluation <strong>of</strong> liver disease. (MK)<br />
19. Common causes <strong>of</strong> drug-induced liver injury. (MK)<br />
20. Genetic considerations in liver disease (i.e. hemochromatosis, Wilson’s disease, alpha-1<br />
antitrypsin deficiency, Gilbert’s syndrome). (MK)<br />
21. The epidemiology, pathophysiology, symptoms, signs, and typical clinical course <strong>of</strong><br />
cholelithiasis and cholecystitis. (MK)<br />
22. The clinical syndrome <strong>of</strong> “ascending cholangitis” including its common causes and typical<br />
clinical course. (MK)<br />
23. The indications for and risks <strong>of</strong> paracentesis and liver biopsy. (MK)<br />
24. The indications for and utility <strong>of</strong> hepatobiliary imaging studies, including:<br />
Ultrasound. (MK)<br />
Nuclear medicine studies. (MK)<br />
CT. (MK)<br />
MRI. (MK)<br />
Magnetic resonance cholangiopancreatography (MRCP). (MK)<br />
Endoscopic retrograde cholangiopancreatography (ERCP). (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, that differentiates among etiologies <strong>of</strong> disease,<br />
including:<br />
Jaundice, discolored urine, pruritis, light-colored stool, unintentional weight loss, fever,<br />
nausea, emesis, diarrhea, altered mental status, abdominal pain, increased abdominal<br />
girth, edema, rectal bleeding, hematemesis. (PC, CS)<br />
DM. (PC, CS)<br />
Alcohol use. (PC, CS)<br />
Prescription, over-the-counter, and illicit drug use. (PC, CS)<br />
Transfusions and other sources <strong>of</strong> potential blood-born pathogen exposure. (PC, CS)<br />
Consumption <strong>of</strong> uncooked shellfish and other food items potentially contaminated with fecal<br />
matter. (PC, CS)<br />
Sexual history. (PC, CS)<br />
Vaccination history. (PC, CS)<br />
Family history <strong>of</strong> liver diseases. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
160
diagnosis and severity <strong>of</strong> disease, including:<br />
Jaundice. (PC)<br />
Complete abdominal examination including findings consistent with ascites (e.g. bulging<br />
flanks, shifting dullness, fluid wave). (PC)<br />
Findings compatible with chronic alcohol use and portal hypertension (e.g. palmar<br />
erythema, spider angiomas, gynecomastia, testicular atrophy, Dupuytren’s contracture,<br />
muscle wasting, splenomegaly, ascites, edema, caput medusa, hemorrhoids). (PC)<br />
Findings compatible with hepatic (portosystemic) encephalopathy (e.g. disturbances <strong>of</strong><br />
consciousness and behavior, fluctuating neurologic signs, asterixis). (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology <strong>of</strong> liver<br />
disease. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
CBC. (PC, MK)<br />
Electrolytes, BUN/Cr, GLC. (PC, MK)<br />
ALB, TP, total bilirubin, direct bilirubin, PT/INR, AST, ALT, Alk Phos. (PC, MK)<br />
Hepatitis serology. (PC, MK)<br />
Ascitic fluid ALB, amylase, cell counts, staining, cultures, and the<br />
serum-ascites albumin gradient (SAAG). (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
results <strong>of</strong>:<br />
Ultrasound. (PC, MK)<br />
Nuclear medicine studies. (PC, MK)<br />
CT. (PC, MK)<br />
MRI. (PC, MK)<br />
Magnetic resonance cholangiopancreatography (MRCP). (PC, MK)<br />
Endoscopic retrograde cholangiopancreatography (ERCP). (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit input and questions from the patient and his or her family about the management<br />
plan. (PC, CS)<br />
Discuss the avoidance <strong>of</strong> known hepatotoxins. (PC, CS)<br />
Counsel patients regarding alcohol abstinence. (PC, CS)<br />
Discuss the importance <strong>of</strong> hepatitis A and B vaccinations for nonimmune patients. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Assist in performing a paracentesis after explaining the procedure to the patient. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
The diagnostic evaluation <strong>of</strong> asymptomatic, isolated elevation <strong>of</strong> the transaminases and/or<br />
Alk Phos. (PC, MK)<br />
The diagnostic evaluation <strong>of</strong> patients with jaundice and unconjugated or conjugated<br />
hyperbilirubinemia. (PC, MK)<br />
The basic management <strong>of</strong> steatosis, hepatitis, cirrhosis, intra- and extra hepatic<br />
cholestasis, acute cholecystitis, ascites, portal hypertension, spontaneous bacterial<br />
161
peritonitis, and hepatic encephalopathy. (PC, MK)<br />
Determining when to obtain consultation from a gastroenterologist, hepatologist, or biliary<br />
surgeon. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to liver disease. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for liver disease. (PLI, P)<br />
2. Recognize the importance <strong>of</strong> patient needs and preferences when selecting among diagnostic<br />
and therapeutic options for liver disease. (P)<br />
3. Respond appropriately to patients who are nonadherent to treatment for liver disease. (CS, P)<br />
4. Demonstrate ongoing commitment to self-directed learning regarding liver disease. (PLI, P)<br />
5. Appreciate the impact liver disease has on a patient’s quality <strong>of</strong> life, wellbeing, ability to work,<br />
and the family. (P)<br />
6. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> liver disease. (P, SBP)<br />
7. Discuss the public health role physicians play in the prevention <strong>of</strong> viral hepatitis. (P, SBP)<br />
8. Appreciate the difficulties patient face with alcohol abstinence. (P)<br />
D. REFERENCES:<br />
Viral Hepatitis<br />
National Center for Infectious Diseases<br />
Center for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/ncidod/diseases/hepatits/index.htm<br />
Practice Guidelines<br />
American Association for the Study <strong>of</strong> Liver Diseases<br />
www.aasld.org<br />
National Institute on Alcohol Abuse and Alcoholism<br />
National Institutes <strong>of</strong> Health<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.niaaa.nih.gov<br />
Pratt DS, Kaplan MM. Evaluation <strong>of</strong> abnormal liver-enzyme results in asymptomatic<br />
patients. N Engl J Med. 2000;342:1266-71.<br />
Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346:1221-31.<br />
Trowbridge RL, Rutkowski NK, Shojania. Does this patient have acute cholecystitis?<br />
JAMA. 2003;289:80-6.<br />
Indar AA, Beckingham IJ. Acute cholecystitis. BMJ. 2002;325:639-43.<br />
Krige JE, Bechingham IJ. ABC <strong>of</strong> diseases <strong>of</strong> liver, pancreas, and biliary system.<br />
Portal hypertension-1: varices.<br />
Krige JE, Bechingham IJ. ABC <strong>of</strong> diseases <strong>of</strong> liver, pancreas, and biliary system.<br />
Portal hypertension-2. Ascites, encephalopathy, and other conditions. BMJ.<br />
2001;322:416-8.<br />
162
TRAINING PROBLEM #26: MAJOR DEPRESSION<br />
RATIONALE:<br />
Major depression is a very common problem in adults, resulting in significant morbidity and mortality.<br />
Most <strong>of</strong>ten the primary care provider is the first health care pr<strong>of</strong>essional to see a depressed patient.<br />
Frequently, the initial presentation is associated with somatic complaints that bring the patient to the<br />
physician. Major depression is also a relatively common accompaniment to serious medical<br />
conditions. There is significant evidence that primary care physicians commonly fail to diagnose<br />
major depression. With relatively recent improvements in available treatment, it is even more<br />
important for internists to screen for major depression and to know the common presenting<br />
symptoms. The internist should also be familiar with available therapeutic options and be prepared to<br />
treat selected patients, including those who decline consultation with a mental health pr<strong>of</strong>essional.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Neurochemistry <strong>of</strong> major depression.<br />
Pharmacology <strong>of</strong> the major classes <strong>of</strong> antidepressants.<br />
Basic understanding <strong>of</strong> the efficacy <strong>of</strong> psychotherapy, antidepressants, and electroconvulsive<br />
therapy.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The epidemiology <strong>of</strong> major depression in the general population and the impact <strong>of</strong> major illness<br />
on the prevalence <strong>of</strong> major depression (e.g. stroke, heart disease, DM, cancer, Parkinson’s<br />
disease, HIV/AIDS). (MK)<br />
2. The impact <strong>of</strong> major depression on the outcome <strong>of</strong> medical illness. (MK)<br />
3. The American Psychiatric Associations’ Diagnostic and Statistical Manual 4 th edition (DSM-IV)<br />
diagnostic criteria for major depression. (MK)<br />
4. Common psychological symptoms and signs <strong>of</strong> major depression (e.g. low mood/affect,<br />
anxiety, irritability/anger, disinterest, anhedonia, decreased libido, guilt, poor self-esteem, poor<br />
concentration, rumination, helplessness, hopelessness, thoughts <strong>of</strong> death and suicide, somatic<br />
complaints). (MK)<br />
5. Common neurovegetative symptoms and signs <strong>of</strong> major depression (e.g. appetite disturbance,<br />
decreased energy, psychomotor retardation or agitation, sleep disturbance). (MK)<br />
6. Common somatic complaints that accompany depressive disorders and the potential for the<br />
occurrence <strong>of</strong> these symptoms without obvious psychological symptoms (e.g. fatigue,<br />
weakness, myalgias, arthralgias, headache, nausea, dyspnea, palpitations, chest<br />
pain/discomfort, lightheadedness/dizziness, bowel movement alterations). (MK)<br />
7. The distinguishing features <strong>of</strong> major depression with psychotic features, bipolar disorder,<br />
dementia, and delirium. (MK)<br />
8. The differential diagnosis <strong>of</strong> major depression, including:<br />
Other psychiatric disorders. (MK)<br />
Drug-induced (e.g. corticosteroids, cimetidine, metoclopramide, clonidine, etc.). (MK)<br />
163
Drug withdrawal (e.g. amphetamine, cocaine). (MK)<br />
Infection (e.g. tertiary syphilis). (MK)<br />
Endocrine/metabolic (e.g. hypo/hyperthyroidism, Cushing’s, Addison’s). (MK)<br />
Collagen vascular diseases (e.g. lupus, fibromyalgia). (MK)<br />
Neurologic (e.g. stoke, multiple sclerosis, Parkinson’s disease, head trauma, complex<br />
partial seizures). (MK)<br />
Nutritional (e.g. B12, folate, niacin, thiamine deficiencies). (MK)<br />
Neoplastic (e.g. pancreatic cancer, disseminated carcinomatosis). (MK)<br />
9. US Preventive Services Task Force (USPSTF) depression screening recommendations. (MK)<br />
10. The risks <strong>of</strong> untreated major depression. (MK)<br />
11. Assessment <strong>of</strong> the risk <strong>of</strong> suicide. (MK)<br />
12. The demographics and risk factors for completed suicide. (MK)<br />
13. The potential link between major depression and substance abuse. (MK)<br />
14. The potential role <strong>of</strong> genetics in depression.(MK)<br />
15. Indications and efficacy <strong>of</strong> the basic therapeutic options for major depression, including:<br />
Psychotherapy (cognitive behavioral therapy or interpersonal psychotherapy). (MK)<br />
Pharmacotherapy. (MK)<br />
Electroconvulsive therapy. (MK)<br />
16. The side effects <strong>of</strong> the major classes <strong>of</strong> antidepressants and common interaction with other<br />
medications. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history, that differentiates among etiologies <strong>of</strong> disease including:<br />
Eliciting the symptoms <strong>of</strong> major depression. (PC, CS)<br />
Determining the presence or absence <strong>of</strong> underlying dementia, anxiety disorders, adverse<br />
drug effects, and grief in any patient suspected <strong>of</strong> having major depression. (PC, CS)<br />
Obtaining a complete drug history (including illicit drugs). (PC, CS)<br />
Identifying chronic diseases that are associated with increased risk <strong>of</strong> major depression.<br />
(PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
A complete neurologic examination. (PC)<br />
A complete mental status exam. (PC)<br />
5. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology for<br />
major depression (psychiatric and nonpsychiatric). (PC, MK)<br />
6. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Blood and urine drug screening. (PC, MK)<br />
Thyroid function tests. (PC, MK)<br />
Serum RPR and VDRL. (PC, MK)<br />
B12, folate, and thiamine levels. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation) the<br />
results <strong>of</strong>:<br />
164
Cranial CT. (PC, MK)<br />
Cranial MRI. (PC, MK)<br />
7. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit input and questions from the patient and his or her family about the management<br />
plan. (PC, CS)<br />
Demonstrate effective listening skills and empathy. (PC, CS)<br />
Advise the patient <strong>of</strong> the delay in therapeutic benefit from antidepressant medications. (PC,<br />
CS)<br />
6. Management skills: Students should able to develop an appropriate evaluation and treatment<br />
plan for patients that includes:<br />
An appreciation <strong>of</strong> the fact that major depression is not generally a “diagnosis <strong>of</strong> exclusion”<br />
and that ruling out all other possible medical causes is typically not necessary. (PC, MK)<br />
Making an accurate diagnosis <strong>of</strong> major depression. (PC, MK)<br />
Assessing for the risk <strong>of</strong> suicide. (PC, MK)<br />
Recommending psychotherapy (cognitive behavioral therapy or interpersonal<br />
psychotherapy). (PC, MK)<br />
Selecting appropriate initial pharmacologic therapy considering efficacy, side effects, and<br />
potential drug-drug interactions. (PC, MK, SBP)<br />
Identifying barriers to major depression treatment. (PC, SBP)<br />
Anticipating potential resistance to seeing a psychiatrist and antidepressant treatment. (PC)<br />
Planning appropriate follow-up. (PC, MK)<br />
Recognizing success or failure <strong>of</strong> initial treatment and making appropriate adjustments.<br />
(PC, MK)<br />
Determining when to obtain consultation from a psychiatrist, psychologist, or other mental<br />
health pr<strong>of</strong>essional. (PC, SBP)<br />
Using a cost-effective approach to treatment. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to major depression. (PC, PLI)<br />
Incorporating patient needs and preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Recognize major depression as an important and potentially life-threatening disease. (P)<br />
2. Appreciate the social stigma <strong>of</strong> psychiatric diagnoses and the ways non-psychiatric physicians<br />
may inadvertently contribute to this. (P)<br />
3. Appreciated the reluctance <strong>of</strong> some patients to see a psychiatrist. (P)<br />
4. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for major depression. (PLI,<br />
P)<br />
5. Recognize the importance <strong>of</strong> patient needs and preferences when selecting among diagnostic<br />
and therapeutic options for major depression. (P)<br />
6. Respond appropriately to patients who are nonadherent to treatment for major depression.<br />
(CS, P)<br />
7. Demonstrate ongoing commitment to self-directed learning regarding major depression. (PLI,<br />
P)<br />
8. Appreciate the impact major depression has on a patient’s quality <strong>of</strong> life, wellbeing, ability to<br />
work, and the family. (P)<br />
165
9. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other health<br />
care pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> major depression. (P, SBP)<br />
D. REFERENCES:<br />
Depression<br />
National Institute <strong>of</strong> Mental Health<br />
National Institutes <strong>of</strong> Health<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.nimh.nih.gov/publicat//defresssion.cfm<br />
Practice Guidelines<br />
American Psychiatric Association<br />
www.psych.org/psych_pract/treatg/pg/prac_guide.cfm<br />
The National Association on Mental Illness<br />
www.nami.org/Template.cfm?Section=By_Illness&Template=/TaggedPa<br />
ge/TaggedPageDisplay.cfm&TPLID=54&ContentID=26414<br />
Mann JJ. The medical management <strong>of</strong> depression. N Engl J Med. 2005;353:1819-34.<br />
166
TRAINING PROBLEM #27: NOSOCOMIAL INFECTIONS<br />
RATIONALE:<br />
Nosocomial infections have been occurring since the inception <strong>of</strong> the hospital. Despite many<br />
advances the incidence is still roughly five percent <strong>of</strong> all acute care hospitalizations or about two<br />
million cases a year. Nosocomial infections are estimated to approximately double the morbidity and<br />
mortality rates <strong>of</strong> any person admitted to the hospital. Directly attributable deaths can total up to<br />
88,000 per year with the expenditure <strong>of</strong> many millions <strong>of</strong> excess health care dollars. Preventing<br />
nosocomial infections is the responsibility <strong>of</strong> every heath care worker, including physicians, house<br />
<strong>of</strong>ficers, medical students, nurses, technicians, administrators, etc. Also considered here are<br />
occupational exposures for which health care workers are at risk.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Basic training in body substance isolation procedures.<br />
Microbiology and pathophysiology <strong>of</strong> the common nosocomial organisms, including<br />
Staphylococcus aureus (methicillin sensitive and resistant), Staphylococcus epidermidis,<br />
Enterococcus species (vancomycin sensitive and resistant), Pseudomonas aeruginosa and<br />
other nosocomial gram-negative bacilli, Clostridium difficile, and Candida species.<br />
The pharmacology <strong>of</strong> antimicrobial agents.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The epidemiology and significance <strong>of</strong> nosocomial infections in the United States. (MK)<br />
2. The general clinical risk factors for nosocomial infection. including:<br />
Immunocompromise. (MK)<br />
Immunosuppressive drugs. (MK)<br />
Extremes <strong>of</strong> age. (MK)<br />
Compromise <strong>of</strong> the skin and mucosal surfaces secondary to:<br />
o Drugs. (MK)<br />
o Irradiation. (MK)<br />
o Trauma. (MK)<br />
o Invasive diagnostic and therapeutic procedures. (MK)<br />
o Invasive indwelling devises (e.g. intravenous catheter, bladder catheter, endotracheal<br />
tube, etc.). (MK)<br />
3. The major routes <strong>of</strong> nosocomial infection transmission, including:<br />
Contact. (MK)<br />
Droplet. (MK)<br />
Airborne. (MK)<br />
Common vehicle. (MK)<br />
4. The epidemiology, pathophysiology, microbiology, symptoms, signs, typical clinical course,<br />
and preventive strategies for the most common nosocomial infections, including:<br />
Urinary tract infection. (MK)<br />
167
Pneumonia. (MK)<br />
Surgical site infection. (MK)<br />
Intravascular devised-related bloodstream infections. (MK)<br />
Skin infections. (MK)<br />
Health care associated diarrhea. (MK)<br />
5. Empiric antibiotic therapy for the most common nosocomial infections. (MK)<br />
6. The epidemiology, pathophysiology, microbiology, symptoms, signs, typical clinical course,<br />
and preventive strategies for colonization or infection with the following organisms:<br />
Vancomycin-resistant enterococci. (MK)<br />
Clostridium difficile. (MK)<br />
Methicillin-resistant Staphylococcus aureus. (MRSA) (MK)<br />
Multidrug-resistant Gram-negative bacteria. (MK)<br />
7. The crucial importance <strong>of</strong> judicious antibiotic use. (MK)<br />
8. The effect <strong>of</strong> widespread use <strong>of</strong> broad spectrum anti-microbial agents on endogenous body<br />
flora and the hospital microbial flora. (MK)<br />
9. The types <strong>of</strong> isolation procedures and their indications:<br />
Standard. (MK)<br />
Airborne. (MK)<br />
Contact. (MK)<br />
Droplet. (MK)<br />
10. The Centers for Disease Control and Prevention (CDC) guidelines for hand hygiene. (MK)<br />
11. Preventive strategies for needlestick and sharps injuries intended to reduce the transmission <strong>of</strong><br />
bloodborne pathogens (hepatitis B, hepatitis C, and HIV). (MK)<br />
12. Local hospital post-exposure (i.e. after an eye/mucous membrane splash, needlestick or other<br />
sharps injury) protocols for prompt reporting, evaluation, counseling, treatment, and follow-up.<br />
(MK, SBP)<br />
13. The indications, efficacy, and side effects <strong>of</strong> post-exposure prophylaxis for hepatitis B and<br />
HIV/AIDS. (MK)<br />
14. negative-pressure ventilation isolation for known or suspected tuberculosis patients (MK)<br />
15. National Institute for Occupational Safety and Health (NIOSH) approved personal respiratory<br />
protective equipment (i.e. N95 respirator) use for the prevention <strong>of</strong> transmission <strong>of</strong><br />
Mycobacterium tuberculosis to health care workers. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
3. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history, that differentiates among etiologies <strong>of</strong> disease in the organ systems<br />
likely to be involved with nosocomial infection. (PC, CS)<br />
4. Physical exam skills: Students should be able to perform a physical examination <strong>of</strong> skin,<br />
vascular access sites, lungs, abdomen, wounds, and catheter and drain sites and recognize signs<br />
<strong>of</strong> local or systemic infection (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
<strong>of</strong> the likely sites and organisms involved, recognizing specific history and physical exam<br />
findings that suggest a specific etiology. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based o the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
168
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Urinalysis and culture and sensitivities. (PC, MK)<br />
Sputum Gram stain and culture and sensitivities. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
Wound cultures and sensitivities. (PC, MK)<br />
Clostridium difficile toxin assay. (PC, MK)<br />
Hepatitis serologies. (PC, MK)<br />
HIV ELISA and western blot. (PC, MK)<br />
Sputum AFB staining and culture. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit input and questions from the patient and his or her family about the management<br />
plan. (PC, CS)<br />
Explain the necessity for isolation procedures. (PC, CS)<br />
Counsel patients about the need for judicious antibiotic usage and the potential patientspecific<br />
and public health risks <strong>of</strong> not doing so. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Obtain blood cultures. (PC)<br />
Place and interpret a PPD. (PC)<br />
Demonstrate proper sterile technique for invasive procedures. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Assessing a hospitalized patient who develops a new fever 48 or more hours after<br />
admission. (PC, MK)<br />
Developing a plan for the evaluation and treatment <strong>of</strong> hospital acquired infection. (PC, MK)<br />
Demonstrating appropriate choice <strong>of</strong> antimicrobial drugs which considers mechanisms <strong>of</strong><br />
action, spectrum <strong>of</strong> activity, pharmacokinetics, drug interactions, and adverse reactions.<br />
(PC, MK)<br />
Recognizing when indwelling intravascular and urinary collection devices should be<br />
removed. (PC, MK)<br />
Requesting appropriate isolation measures to protect other patients and health care<br />
workers. (PC, SBP)<br />
Determining when to obtain consultation from an infectious diseases specialist. (PC, SBP)<br />
Contacting hospital infection control experts when appropriate. (SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to nosocomial infections. (PC, PLI)<br />
Incorporating patient needs and preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Serve as a role model to all other health care providers by strictly following all infection control<br />
measures including hand hygiene and all isolation procedures. (P, SBP)<br />
2. Appreciate the role physicians play in the inappropriate prescribing <strong>of</strong> antimicrobial agents and<br />
the public health ramifications. (P, SBP)<br />
3. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for nosocomial infections.<br />
169
(PLI, P)<br />
4. Recognize the importance <strong>of</strong> patient needs and preferences when selecting among diagnostic<br />
and therapeutic options for nosocomial infections. (P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding nosocomial infections.<br />
(PLI, P)<br />
6. Appreciate the impact nosocomial infections have on a patient’s quality <strong>of</strong> life, well-being,<br />
ability to work, and the family. (P)<br />
7. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other health<br />
care pr<strong>of</strong>essionals in the diagnosis, treatment, and prevention <strong>of</strong> nosocomial infections. (P, SBP)<br />
D. REFERENCES:<br />
Infection Control Guidelines<br />
Division <strong>of</strong> Healthcare Quality Promotion<br />
National Center for Infectious Diseases<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/ncidod/hip/default.htm<br />
Vancomycin-Resistant Enterococci Division <strong>of</strong> Healthcare<br />
Quality Promotion National Center for Infectious Diseases<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/ncidod/hip/ARESIST/vre.htm<br />
Pautanen SM, Simor AE. Clostridium difficile associated diarrhea in adults. Can Med<br />
Assoc J. 2004;171:51-8.<br />
www.cmaj.ca/cgi/reprint/171/1/51<br />
Healthcare-Associated MRSA Division <strong>of</strong> Healthcare Quality Promotion National Center<br />
for Infectious Diseases Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/ncidod/dhqp/ar_mrsa.html<br />
170
TRAINING PROBLEM #28: OBESITY<br />
RATIONALE:<br />
Obesity and overweight are recognized as ever growing epidemics in the United States. These<br />
conditions have been correlated with the development <strong>of</strong> medical conditions such as diabetes,<br />
hypertension, heart disease, and osteoarthritis. Mastery <strong>of</strong> the approach to patients who are not at<br />
an ideal body weight is important to general internists because they <strong>of</strong>ten deal with the sequelae <strong>of</strong><br />
the comorbid illnesses.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Psychology associated with addictive behavior.<br />
Anatomy, physiology, and pathophysiology <strong>of</strong> the gastrointestinal tract and digestion.<br />
Pharmacology <strong>of</strong> the available drugs used to treat obesity.<br />
Nutrition and caloric requirements.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The etiology <strong>of</strong> obesity including excessive caloric intake, insufficient energy expenditure<br />
leading to low resting metabolic rate, genetic predisposition, environmental factors affecting weight<br />
gain, psychologic stressors, and lower socioeconomic status. (MK)<br />
2. The definition and classification <strong>of</strong> overweight and obese using BMI. (MK)<br />
3. The health implications that being overweight or obese may have on the patient. (MK)<br />
4. How daily caloric requirements are calculated and the caloric deficit required to achieve a five<br />
to 10 percent weight reduction in six to 12 months. (MK)<br />
5. The principles <strong>of</strong> behavior modification. (MK)<br />
6. How to develop an exercise program and assist the patient in setting goals for weight loss.<br />
(MK)<br />
7. Treatment options, including nonpharmacologic and pharmacologic treatment, behavioral<br />
therapy and surgical intervention. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, including:<br />
Reviewing the patient’s weight history from childhood. (PC, CS)<br />
Assessing the risk factors for obesity related conditions. (PC, CS)<br />
Assessing the patient’s motivation for losing weight. (PC, CS)<br />
Reviewing the patient’s past experience with losing weight and determining barriers<br />
encountered in prior attempts. (PC, CS)<br />
Reviewing the patient’s activity level and diet. (PC, CS)<br />
Obtaining an assessment <strong>of</strong> tobacco and drug use especially noting if the patient is in the<br />
171
process <strong>of</strong> stopping either. (PC, CS)<br />
Obtaining a family history focusing on weight related issues and comorbid illnesses<br />
associated with obesity. (PC, CS)<br />
Obtaining a focused review <strong>of</strong> systems including signs and symptoms <strong>of</strong> secondary causes<br />
<strong>of</strong> obesity such as Cushing’s syndrome, hypothyroidism, and hypogonadism. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Calculation <strong>of</strong> degree <strong>of</strong> obesity from the patient’s height and weight by calculating BMI.<br />
(PC)<br />
Noting the presence <strong>of</strong> abdominal obesity based on waist-to-hip circumference. (PC)<br />
Assessing the signs <strong>of</strong> vascular disease including hypertension, carotid bruits, abdominal<br />
aortic size, blood pressure and peripheral pulses. (PC)<br />
Assessing for signs <strong>of</strong> endocrine abnormalities, including: striae, peripheral neuropathy,<br />
depressed tendon reflexes, bruising, and signs <strong>of</strong> dyslipidemia (e.g. xanthomas and<br />
xanthalasma). (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology <strong>of</strong><br />
primary and secondary obesity. (MK, PC)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Serum GLC. (PC, MK)<br />
TSH. (PC, MK)<br />
Lipid pr<strong>of</strong>ile. (PC, MK)<br />
HbA1c. (PC, MK)<br />
BUN/Cr. (PC, MK)<br />
Urine microalbumin. (PC, MK)<br />
ECG. (PC, MK)<br />
24-hour urinary cortisol (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Adapt to the patient’s life-style and preferences, with emphasis on the patient’s role in<br />
treatment and maximizing compliance. (PC, CS)<br />
Assist the patient in understanding that attainment <strong>of</strong> ideal body weight may not necessarily<br />
be a realistic goal and that health benefits may be achieved with losses <strong>of</strong> five to 10<br />
percent body weight. (PC, CS)<br />
6. Management skills: Students should able to develop an appropriate evaluation and treatment<br />
plan for patients that includes:<br />
Determining when to obtain consultation from an endocrinologist, dietician, or obesity<br />
management specialist. (PC, SBP)<br />
Developing reasonable weight loss goals with the patient. (PC, MK)<br />
Developing a dietary plan. (PC, MK)<br />
Developing a prescription for physical activity. (PC, MK)<br />
Identifying indications for pharmacotherapy. (PC, MK)<br />
Identifying indications for bariatric surgery. (PC, MK)<br />
172
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to obesity. (PC, PLI)<br />
Incorporating patient preferences in the treatment plan. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for obesity. (PLI, P)<br />
2. Respond appropriately to patients who are nonadherent to treatment for obesity.<br />
(CS, P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding obesity. (PLI,<br />
P)<br />
4. Appreciate the impact obesity has on a patient’s quality <strong>of</strong> life, well-being, ability to<br />
work, and family. (P)<br />
5. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong><br />
other healthcare pr<strong>of</strong>essions in the treatment <strong>of</strong> obesity. (P, SBP)<br />
D. REFERENCES:<br />
Overweight and Obesity<br />
National Center for Chronic Disease Prevention and Health Promotion Center for Disease<br />
Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/nccdphp/dnpa/obesity<br />
Aim for a Healthy Weight National Heart, Lung, and Blood Institute Obesity Education<br />
Initiative National Institutes <strong>of</strong> Health<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.nhlbi.nih.gov/health/public/heart/obesity/lose_wt/index.htm<br />
Screening for Obesity in Adults<br />
Agency for Healthcare Research and Quality<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.ahrq.gov/clinic/uspstf/uspsobes.htm<br />
Tsai AG, Wadden TA. Systematic review: an evaluation <strong>of</strong> major commercial weight loss<br />
programs in the United States. Ann Intern Med. 2005;152-56-66.<br />
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and<br />
meta-analysis. JAMA. 2004;292:1724-37.<br />
Li Z, Maglione M, Tu W, et al. Meta-analysis: pharmacologic treatment <strong>of</strong> obesity. Ann<br />
Intern Med. 2005;142:532-46. \<br />
173
TRAINING PROBLEM #29: PNEUMONIA<br />
RATIONALE:<br />
Pneumonia continues to be a major public health issue, a leading reason for hospitalization, and<br />
a significant cause <strong>of</strong> mortality. Not only that, it is an important complication <strong>of</strong> admission for<br />
other causes. Many different specialties encounter pneumonia in the course <strong>of</strong> practice, the<br />
internist most particularly.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy and physiology <strong>of</strong> the pulmonary system.<br />
Pathogenesis and pathophysiology <strong>of</strong> pneumonia.<br />
Microbiology <strong>of</strong> the common pneumonia pathogens.<br />
Pharmacology <strong>of</strong> antimicrobial agents.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The epidemiology, pathophysiology, symptoms, signs, and typical clinical course <strong>of</strong><br />
community-acquired, nosocomial, and aspiration pneumonia and pneumonia in the<br />
immunocompromised host. (MK)<br />
2. The conceptualization <strong>of</strong> “typical” and “atypical” pneumonia and its limitations. (MK)<br />
3. Common pneumonia pathogens (viral, bacterial, mycobacterial, and fungal) in<br />
immunocompetent and immunocompromised hosts). (MK)<br />
4. Identify patients who are at risk for impaired immunity. (MK)<br />
5. Indications for hospitalization and ICU admission <strong>of</strong> patient with pneumonia. (MK)<br />
6. The radiographic findings <strong>of</strong> the various types <strong>of</strong> pneumonia. (MK)<br />
7. The antimicrobial treatments (e.g. antiviral, antibacterial, antimycobacterial, and antifungal)<br />
for community-acquired, nosocomial, and aspiration pneumonia, and pneumonia in the<br />
immunocompromised host. (MK)<br />
8. The implications <strong>of</strong> antimicrobial resistance. (MK)<br />
9. The pathogenesis, symptoms, and signs <strong>of</strong> the complications <strong>of</strong> acute bacterial pneumonia<br />
including: bacteremia, sepsis, parapneumonic effusion, empyema, meningitis, and<br />
metastatic microabscesses. (MK)<br />
10. The indications for and complications <strong>of</strong> chest tube placement. (MK)<br />
11. The indications for and efficacy <strong>of</strong> influenza and pneumococcal vaccinations. (MK)<br />
12. The indications and procedures for respiratory isolation. (MK)<br />
13. The Centers for Medicare & Medicaid Services (CMS) and the Joint Commission on the<br />
Accreditation <strong>of</strong> Healthcare Organizations (JCAHO) quality measures for communityacquired<br />
pneumonia treatment. (MK, PLI, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
174
The presence and quantification <strong>of</strong> fever, chills, sweats, cough, sputum, hemoptysis,<br />
dyspnea, and chest pain. (PC, CS)<br />
Historical features consistent with potential immunocompromise. (PC, CS)<br />
potential tuberculosis exposure (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Accurately determining respiratory rate and level <strong>of</strong> respiratory distress. (PC)<br />
Identifying bronchial breath sounds, rales, rhonchi, and wheezes. (PC)<br />
Identifying signs <strong>of</strong> pulmonary consolidation. (PC)<br />
Identifying signs <strong>of</strong> pleural effusion. (PC)<br />
Identifying signs <strong>of</strong> the complications <strong>of</strong> pneumonia. (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential<br />
diagnosis recognizing specific history and physical exam findings that suggest a specific<br />
etiology <strong>of</strong> pneumonia and other possible diagnoses, including:<br />
Common cold. (PC, MK)<br />
Acute bronchitis. (PC, MK)<br />
Influenza. (PC, MK)<br />
Acute exacerbation <strong>of</strong> COPD. (PC, MK)<br />
Asthma exacerbation. (PC, MK)<br />
CHF. (PC, MK)<br />
Pulmonary embolism. (PC, MK)<br />
Aspiration. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
CBC. (PC, MK)<br />
Blood cultures. (PC, MK)<br />
ABG. (PC, MK)<br />
Pleural fluid chemistry, cell counts, staining, and culture. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation)<br />
the results <strong>of</strong>:<br />
Chest CT. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, prognosis, and subsequent follow-up to the<br />
patient and his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
Educate the patient about pneumococcal and influenza immunizations. (PC, CS)<br />
Educate the patient about the importance <strong>of</strong> smoking cessation. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Place and interpret a tuberculin skin test (PPD). (PC)<br />
Obtain blood cultures. (PC)<br />
Obtain an ABG. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
175
Selecting an appropriate empiric antibiotic regimen for community-acquired, nosocomial,<br />
immunocompromised-host, and aspiration pneumonia, taking into account pertinent patient<br />
features. (PC, MK)<br />
Adjusting antimicrobial treatment according to the sputum staining and culture results. (PC,<br />
MK)<br />
Recognizing the complications <strong>of</strong> pneumonia. (PC, MK)<br />
Determining when to obtain consultation from a pulmonologist or infectious diseases<br />
specialist. (PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to pneumonia. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for the various types <strong>of</strong><br />
pneumonia. (PLI, P)<br />
2. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for pneumonia. (P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding pneumonia. (PLI, P)<br />
4. Appreciate the impact pneumonia has on a patient’s quality <strong>of</strong> life, well-being, ability to work,<br />
and the family. (P)<br />
5. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
healthcare pr<strong>of</strong>essionals in the treatment <strong>of</strong> pneumonia. (P, SBP)<br />
6. Appreciate the importance <strong>of</strong> antimicrobial resistance. (P)<br />
7. Appreciate the public health role <strong>of</strong> the physician when treating certain types <strong>of</strong> pneumonia<br />
(e.g. tuberculosis). (P)<br />
8. Appreciate the importance <strong>of</strong> and demonstrate a commitment to meeting national health care<br />
quality measures for the treatment <strong>of</strong> acute MI. (P, SBP, PLI)<br />
D. REFERENCES:<br />
Improving Treatment Decisions for Patients with Community-Acquired Pneumonia Agency<br />
for Healthcare Research and Quality<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.ahrq.gov/clinic/pneumonia/pneumonria.htm<br />
Ramsdell J, Narsavage GL, Fink JB. Management <strong>of</strong> community-acquired pneumonia<br />
in the home: an American College <strong>of</strong> Chest Physicians clinical position statement.<br />
Chest. 2005;127:1752-63.<br />
www.guideline.gov/summary/summary.aspx?ss=15&doc_id=7325&nbr=4 348<br />
Influenza<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/flu/<br />
Prevention <strong>of</strong> Pneumococcal Disease: Recommendations <strong>of</strong> the Advisory<br />
Committee on Immunization Practices (ACIP). MMWR 46(RR-08);1-24. Centers for<br />
Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
176
www.cdc.gov/mmwr/PDF/RR/RR4608.pdf<br />
Prevention and Control <strong>of</strong> Influenza: Recommendations <strong>of</strong> the Advisory Committee<br />
on Immunization Practices (ACIP). MMWR 50(RR-04);1-46. Centers for Disease<br />
Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/mmwr/PDF/RR/RR5004<br />
177
TRAINING PROBLEM #30: RHEUMATOLOGIC PROBLEMS<br />
RATIONALE:<br />
Rheumatologic diseases are an important part <strong>of</strong> the practice <strong>of</strong> internal medicine. This includes<br />
problems referring to specific joints as well as patients with systemic symptoms that are sometimes<br />
difficult to unify into a single diagnosis.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Anatomy, physiology, and pathophysiology <strong>of</strong> the musculoskeletal system.<br />
Basic course work in immunology.<br />
Pharmacology <strong>of</strong> acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs),<br />
glucocorticoids, disease-modifying antirheumatic drugs (DMARDs), drugs use in the treatment<br />
<strong>of</strong> gout.<br />
Basic bone radiograph interpretation.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. A systematic approach to joint pain based on an understanding <strong>of</strong> pathophysiology to classify<br />
potential causes. (MK)<br />
2. The effect <strong>of</strong> the time course <strong>of</strong> symptoms on the potential causes <strong>of</strong> joint pain (acute vs.<br />
subacute vs. chronic). (MK)<br />
3. The difference between and pathophysiology <strong>of</strong> arthralgia vs. arthritis and mechanical vs.<br />
inflammatory joint pain. (MK)<br />
4. The distinguishing features <strong>of</strong> intra-articular and periarticular complaints (joint pain vs. bursitis<br />
and tendonitis). (MK)<br />
5. The effect <strong>of</strong> the features <strong>of</strong> joint involvement on the potential causes <strong>of</strong> joint pain<br />
(monoarticular vs. oligoarticular vs. polyarticular, symmetric vs. asymmetric, axial and/or<br />
appendicular, small vs. large joints, additive vs. migratory vs. intermittent). (MK)<br />
6. Indications for performing an arthrocentesis and the results <strong>of</strong> synovial fluid analysis. (MK)<br />
7. The pathophysiology and common signs and symptoms <strong>of</strong>:<br />
Osteoarthritis. (MK)<br />
Crystalline arthropathies. (MK)<br />
Septic arthritis. (MK)<br />
8. Indications for and effectiveness <strong>of</strong> intra-articular steroid injections. (MK)<br />
9. Treatment options for gout (e.g. colchicine, NSAIDs, steroids, uricosurics, xanthine oxidase<br />
inhibitors). (MK)<br />
10. The pathophysiology and common signs and symptoms <strong>of</strong> common periarticular disorders:<br />
Sprain/stain. (MK)<br />
Tendonitis. (MK)<br />
Bursitis. (MK)<br />
11. The basic pathophysiology <strong>of</strong> autoimmunity and autoimmune diseases. (MK)<br />
12. The basic role <strong>of</strong> genetics in autoimmune disorders. (MK)<br />
178
13. Typical clinical scenarios when systemic rheumatologic disorders should be considered:<br />
Diffuse aches and pains. (MK)<br />
Generalized weakness/fatigue. (MK)<br />
Myalgias with or without weakness. (MK)<br />
Arthritis with systemic signs (e.g. fever, weight loss). (MK)<br />
Arthritis with disorders <strong>of</strong> other systems (e.g. rash, cardiopulmonary symptoms,<br />
gastrointestinal symptoms, eye disease, renal disease, neurologic symptoms). (MK)<br />
14. The common signs and symptoms <strong>of</strong> and diagnostic approach to:<br />
Rheumatoid arthritis. (MK)<br />
Spondyloarthropathies (reactive arthritis/Reiter’s syndrome, ankylosing spondylitis,<br />
psoriatic arthritis). (MK)<br />
Systemic lupus erythematosus. (MK)<br />
Systemic sclerosis. (MK)<br />
Raynaud’s syndrome/phenomenon. (MK)<br />
Sjögren’s syndrome. (MK)<br />
Temporal arteritis and polymyalgia rheumatica. (MK)<br />
Other systemic vasculitides. (MK)<br />
Polymyositis and dermatomyositis. (MK)<br />
Fibromyalgia. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history that differentiates among etiologies <strong>of</strong> disease, including:<br />
Eliciting features <strong>of</strong> joint complaints:<br />
o Pain. (PC, CS)<br />
o Stiffness. (PC, CS)<br />
o Location. (PC, CS)<br />
o Mode <strong>of</strong> onset. (PC, CS)<br />
o Duration. (PC, CS)<br />
o Severity. (PC, CS)<br />
o Exacerbating and alleviating factors. (PC, CS)<br />
o Warmth, redness, and tenderness. (PC, CS)<br />
o Associated nonarticular symptoms. (PC, CS)<br />
Determining when in the course <strong>of</strong> acute arthritis it is necessary to obtain a sexual history.<br />
(PC, CS)<br />
Determining the impact <strong>of</strong> rheumatologic complaints on a patient's activities <strong>of</strong> daily living.<br />
(PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
A systematic examination <strong>of</strong> all joints identifying the following abnormal findings:<br />
o Erythema, warmth, tenderness, and swelling. (PC)<br />
o Effusion. (PC)<br />
o Crepitus. (PC)<br />
o Altered range <strong>of</strong> motion. (PC)<br />
o Ulnar deviation. (PC)<br />
o Synovial thickening. (PC)<br />
o Joint alignment deformities (e.g. varus and valgus). (PC)<br />
o Podagra. (PC)<br />
179
Muscular bulk, strength, and tenderness. (PC)<br />
Examination <strong>of</strong> the skin identifying the following abnormal findings:<br />
o Rheumatoid and tophaceous nodules. (PC)<br />
o Alopecia. (PC)<br />
o Malar rash. (PC)<br />
o Sclerodactyly. (PC)<br />
o Telangiectasias. (PC)<br />
o Raynaud’s phenomenon. (PC)<br />
o Psoriasis. (PC)<br />
o Cutaneous manifestations <strong>of</strong> vasculitis (e.g. palpable purpura). (PC)<br />
3. Differential diagnosis: Students should be able to generate a prioritized differential diagnosis<br />
recognizing specific history and physical exam findings that suggest a specific etiology:<br />
Osteoarthritis. (PC, MK)<br />
Crystalline arthropathies. (PC, MK)<br />
Septic arthritis. (PC, MK)<br />
Rheumatoid arthritis. (PC, MK)<br />
Spondyloarthropathies (reactive arthritis/Reiter’s syndrome, ankylosing spondylitis,<br />
psoriatic arthritis). (PC, MK)<br />
Systemic lupus erythematosus. (PC, MK)<br />
Systemic sclerosis. (PC, MK)<br />
Raynaud’s syndrome/phenomenon. (PC, MK)<br />
Sjörgren’s syndrome. (PC, MK)<br />
Temporal arteritis and polymyalgia rheumatica. (PC, MK)<br />
Other systemic vasculitides. (PC, MK)<br />
Polymyositis and dermatomyositis. (PC, MK)<br />
Fibromyalgia. (PC, MK)<br />
5. Laboratory interpretation: Students should be able to recommend when to order diagnostic and<br />
laboratory tests and be able to interpret them, both priorto and after initiating treatment based<br />
on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
CBC with differential. (PC, MK)<br />
Synovial fluid analysis (Gram stain, culture, crystal exam, cell count with differential, and<br />
glucose). (PC, MK)<br />
Uric acid. (PC, MK)<br />
ESR. (PC, MK)<br />
Rheumatoid factor (RF). (PC, MK)<br />
Antinuclear antibody test (ANA) and anti-DNA test. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation)<br />
the results <strong>of</strong>:<br />
Plain radiographs <strong>of</strong> the shoulder, elbow, wrist, hand, hip, knee, ankle, and foot. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to patients. (PC,<br />
CS)<br />
Elicit questions from the patient about the management plan. (PC, CS)<br />
6. Basic and advanced procedure skills: Students should be able to:<br />
Assist in the performance <strong>of</strong> an arthrocentesis and intra-articular corticosteroid<br />
injection. (PC)<br />
7. Management skills: Students should able to develop an appropriate evaluation and<br />
180
treatment plan for patients that includes:<br />
Selecting appropriate medications for the relief <strong>of</strong> joint pain. (PC, MK)<br />
Prescribing acute and preventative treatment for crystalline arthropathies. (PC, MK)<br />
Prescribing basic treatment options for septic arthritis. (PC, MK)<br />
Prescribing basic treatment options for systemic rheumatologic conditions. (PC, MK)<br />
Determining when to obtain consultation from a rheumatologist and orthopedic surgeon.<br />
(PC, SBP)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to rheumatologic problems. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection diagnostic and therapeutic interventions for rheumatologic<br />
problems. (PLI, P)<br />
2. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic and<br />
therapeutic options for rheumatologic problems. (P)<br />
3. Respond appropriately to patients who are nonadherent to treatment for rheumatologic<br />
problems. (CS, P)<br />
4. Demonstrate ongoing commitment to self-directed learning regarding rheumatologic problems.<br />
(PLI, P)<br />
5. Appreciate the impact rheumatologic problems have on a patient’s quality <strong>of</strong> life, well-being,<br />
ability to work, and the family. (P)<br />
6. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization<br />
<strong>of</strong> other healthcare pr<strong>of</strong>essions in the treatment <strong>of</strong> rheumatologic problems. (P, SBP)<br />
D. REFERENCES:<br />
Evaluation <strong>of</strong> the patient – history and physical examination, laboratory assessment,<br />
arthrocentesis and synovial fluid analysis. In Schumacher HR, Klippel JH, Koopman<br />
WJ, eds. Primer on the Rheumatic Diseases. 12 th Ed. Atlanta, GA: Arthritis Foundation;<br />
2001.<br />
Management Guidelines<br />
American College <strong>of</strong> Rheumatology<br />
www.rheumatology.org/publications/guidelines/index.asp<br />
Arthritis Foundation<br />
www.arthritis.org<br />
National Institute <strong>of</strong> Arthritis and Musculoskeletal and Skin Diseases<br />
National Institutes <strong>of</strong> Health<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.niams.nih.gov<br />
181
TRAINING PROBLEM #31: SMOKING CESSATION<br />
RATIONALE:<br />
Smoking is a major public health issue because it causes or aggravates many serious illnesses.<br />
Effective intervention strategies for chronic smokers have been developed using principals <strong>of</strong><br />
behavioral counseling. These principals are applicable to other risky health behaviors. Health<br />
behavior risk assessment and intervention is now expected <strong>of</strong> physicians as part <strong>of</strong> the<br />
comprehensive care <strong>of</strong> adults. Selecting and performing an appropriate smoking cessation<br />
intervention is an important training problem for the third year medical student.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> the anatomy, physiology, and pathophysiology <strong>of</strong> the cardiopulmonary system.<br />
Knowledge <strong>of</strong> the pharmacology <strong>of</strong> addictive drugs.<br />
Knowledge <strong>of</strong> the risks <strong>of</strong> smoking, passive smoke, and smokeless tobacco.<br />
Appreciation <strong>of</strong> the reasons for or against discontinuing smoking.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The pharmacologic effects <strong>of</strong> nicotine. (MK)<br />
2. Nicotine withdrawal symptoms. (MK)<br />
3. Intervention strategies physicians can use for those patients willing and not willing to quit. (MK)<br />
4. The stages <strong>of</strong> change, including:<br />
Precontemplation. (MK)<br />
Contemplation. (MK)<br />
Preparation. (MK)<br />
Action. (MK)<br />
Maintenance. (MK)<br />
5. The “five A’s” <strong>of</strong> smoking cessation:<br />
Ask. (MK)<br />
Advise. (MK)<br />
Assess. (MK)<br />
Assist. (MK)<br />
Arrange. (MK)<br />
6. The “five R’s” <strong>of</strong> smoking cessation:<br />
Relevance. (MK)<br />
Risks. (MK)<br />
Rewards. (MK)<br />
Roadblocks. (MK)<br />
Repetition. (MK)<br />
7. The common barriers preventing patients from undertaking smoking cessation. (MK)<br />
8. The principles <strong>of</strong> at least one theory <strong>of</strong> behavior modification. (MK)<br />
9. Common medical diseases associated with chronic smoking and the effects <strong>of</strong> stopping on<br />
182
future risk. (MK)<br />
10. The indications for nicotine replacement therapy, pharmacotherapy (i.e. bupropion) or both.<br />
(MK)<br />
11. The association between smoking cessation and weight gain. (MK)<br />
12. The fact that tobacco dependence is considered a chronic relapsing disorder. (MK)<br />
13. The Centers for Medicare & Medicaid Services (CMS) and the Joint Commission on the<br />
Accreditation <strong>of</strong> Healthcare Organizations (JCAHO) quality measures for smoking cessation<br />
advice (i.e. all smoking patients admitted with pneumonia, HF, or an acute MI are given<br />
smoking cessation advice or counseling during hospital stay). (MK, PLI, SBP)<br />
B. SKILLS: Students should demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an ageappropriate<br />
medical history, including:<br />
Ask the patient if he or she uses tobacco. (PC, CS)<br />
Determine the length and magnitude <strong>of</strong> tobacco use. (PC, CS)<br />
Ask if the patient is interested in stopping.<br />
Ask about the patient’s past experiences with smoking cessation. (PC, CS)<br />
Ask relevant questions regarding the symptoms <strong>of</strong> diseases associated with long-term<br />
smoking (e.g. CAD, COPD, PVD, CVA, lung cancer). (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Identification <strong>of</strong> nicotine stains. (PC)<br />
Identification <strong>of</strong> lesions with malignant potential on the lips and in the oral cavity. (PC)<br />
Identification <strong>of</strong> chest findings consistent with chronic obstructive lung disease and lung<br />
cancer. (PC)<br />
Examination <strong>of</strong> the heart and vascular system. (PC)<br />
3. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences. Laboratory and diagnostic tests should include,<br />
when appropriate:<br />
Complete blood count to detect erythrocytosis. (PC, MK)<br />
Lipid pr<strong>of</strong>ile to aid in cardiovascular stratification. (PC, MK)<br />
4. Communication skills: Students should be able to:<br />
1. Ask every patient if he or she uses tobacco. (PC, CS)<br />
2. Advise every patient who smokes to stop in a nonjudgmental manner. (PC, CS)<br />
3. Assess the patient’s willingness to make attempt to quit. (PC, CS)<br />
4. Assist those who are willing to make a quit attempt through counseling. (PC, CS)<br />
5. Respond positively and non-judgmentally to the patient’s excuses or concerns about<br />
cessation. (PC, CS)<br />
6. Get the patient to commit to a specific action plan that can lead to complete<br />
cessation. (PC, CS)<br />
7. For those unwilling to quit, use <strong>of</strong> “5 R’s” to motivate the patient:<br />
o Relevance. (PC, CS)<br />
o Risks. (PC, CS)<br />
o Rewards. (PC, CS)<br />
183
o Roadblocks. (PC, CS)<br />
o Repetition. (PC, CS)<br />
5. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patient, including:<br />
Designing an intervention that matches the stage <strong>of</strong> behavior change demonstrated by the<br />
patient. (PC, CS)<br />
Explaining how to use nicotine patch, nasal spray or inhaler, and/or bupropion therapy.<br />
(PC, CS)<br />
Negotiating a follow-up plan with the patient. (PC, CS)<br />
Encouraging the patient to increase physical activity to lessen weight gain, if medically<br />
appropriate. (PC, CS)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues/resources related to aiding smoking cessation. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Student should be able to:<br />
1. Demonstrate a commitment to meeting national quality standards for smoking cessation. (P,<br />
PLI, SBP)<br />
2. Maintain a non-judgmental attitude at all times regarding smoking cessation. (P)<br />
3. Demonstrate a commitment to deliver a non-judgmental "stop smoking" message to every<br />
patient who smokes. (P)<br />
4. Promote problem-solving by the patient. (P)<br />
5. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for smoking<br />
cessation. (PLI, P)<br />
6. Respond appropriately to patients who are non-adherent to treatment for smoking cessation.<br />
(P)<br />
7. Demonstrate ongoing commitment to self-directed learning regarding smoking cessation. (PLI,<br />
P)<br />
8. Appreciate the impact smoking cessation has on a patient’s quality <strong>of</strong> life, well-being, ability to<br />
work, and the famRecognize the importance and demonstrate a commitment to the utilization<br />
<strong>of</strong> other healthcare pr<strong>of</strong>essions in the treatment <strong>of</strong> smoking cessation. (P, SBP)<br />
D. RESOURCES:<br />
Public Health Service<br />
<strong>Department</strong> <strong>of</strong> Health and Human Services<br />
Tobacco Cessation Guideline<br />
www.surgeongeneral.gov/tobacco/default.htm<br />
Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for<br />
smoking cessation. Cochrane Database <strong>of</strong> Syst Rev. 2004;(3):CD000146.<br />
Schroeder SA. What to do with a patient who smokes. JAMA. 2005;294:482-7.<br />
Talwar A, Jain M, Vijayan VK. Pharmacotherapy <strong>of</strong> tobacco dependence. Med Clin<br />
North Am. 2004;88:1517-34.<br />
184
TRAINING PROBLEM #32: SUBSTANCE ABUSE<br />
RATIONALE:<br />
Substance abuse is a prevalent problem that intersects with patient care on a variety <strong>of</strong> different<br />
levels and in patients from every socio-economic status. Being able to recognize it, counsel<br />
patients appropriately, and devise an appropriate treatment plan is integral to the practice <strong>of</strong><br />
internal medicine.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experiences should<br />
include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> drug and alcohol metabolism and physiology.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Presenting signs and symptoms <strong>of</strong> abuse <strong>of</strong> the following substances:<br />
Alcohol. (MK)<br />
Opioids. (MK)<br />
Cocaine. (MK)<br />
Amphetamines.(MK)<br />
Hallucinogens. (MK)<br />
Barbiturates. (MK)<br />
Marijuana. (MK)<br />
Anabolic steroids. (MK)<br />
Benzodiazepines. (MK)<br />
2. Signs, symptoms, risk factors for, and major causes <strong>of</strong> morbidity and mortality secondary to<br />
alcohol and drug abuse, intoxication, overdose, and withdrawal. (MK)<br />
3, Diagnostic criteria for substance abuse, dependency and addiction. (MK)<br />
4. Questions in the CAGE questionnaire:<br />
Cut down. (MK)<br />
Annoyed/angry. (MK)<br />
Guilty. (MK)<br />
Eye opener. (MK)<br />
5. Health benefits <strong>of</strong> substance abuse cessation. (MK)<br />
6. The potential role <strong>of</strong> genetics in substance abuse vulnerability. (MK)<br />
B. SKILLS: Students should demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document, and present an<br />
age-appropriate medical history, that differentiates among etiologies <strong>of</strong> disease,<br />
including:<br />
Social history that is elicited in a nonjudgmental, supportive manner, using appropriate<br />
questioning (e.g. CAGE questions, etc.). (PC, CS)<br />
185
Use <strong>of</strong> injection drugs and shared needles. (PC, CS)<br />
Relevant medication history. (PC, CS)<br />
Immune status. (PC, CS)<br />
Family history <strong>of</strong> substance abuse. (PC, CS)<br />
Lifestyle factors that will influence patient’s access to illicit substances and interfere with<br />
ability to enable effective treatment. (PC, CS)<br />
Screening for depression and other psychiatric disease. (PC, CS)<br />
2. Physical exam skills: Students should be able to perform a physical exam to establish the<br />
diagnosis and severity <strong>of</strong> disease, including:<br />
Accurate recognition <strong>of</strong> signs that may indicate intoxication or withdrawal (e.g. behavioral or<br />
speech changes, changes in pupil size, conjunctival or nasal injection, tachycardia,<br />
sweating, piloerection, yawning, unsteady gait, etc.). (PC, MK)<br />
Examination <strong>of</strong> the nose for septal perforation as complication <strong>of</strong> cocaine use. (PC, MK)<br />
Examination <strong>of</strong> the skin for track marks or signs <strong>of</strong> needle use. (PC, MK)<br />
Identification <strong>of</strong> stigmata <strong>of</strong> secondary disease states (e.g. cirrhosis – splenomegaly,<br />
gynecomastia, telangiectasias, caput medusa, etc.) (PC, MK)<br />
Assessing for signs <strong>of</strong> endocarditis (e.g., fever, murmur, rash, etc). (PC, MK)<br />
Obtaining full mental status examination. (PC, MK)<br />
3. Differential diagnosis: Students should be able to generate a differential diagnosis<br />
recognizing history, physical exam and/or laboratory findings to determine the diagnosis <strong>of</strong><br />
abuse <strong>of</strong> drugs or alcohol and their sequelae. (PC, MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on the differential diagnosis, including consideration <strong>of</strong> test cost and performance<br />
characteristics as well as patient preferences.<br />
Laboratory and diagnostic tests should include, when appropriate:<br />
Blood alcohol level. (PC, MK)<br />
Urine and serum toxicology screens. (PC, MK)<br />
Hepatic function panel. (PC, MK)<br />
Amylase and lipase levels. (PC, MK)<br />
Tests for HIV, hepatitis B and hepatitis C. (PC, MK)<br />
CBC. (PC, MK)<br />
Blood cultures. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the evaluation, treatment plan, and subsequent follow up to the patient and<br />
his or her family in a non-judgmental manner. (PC, CS)<br />
Elicit questions from the patient and his or her family about the disease process and<br />
management plan. (PC, CS)<br />
Counsel patients regarding cessation and available community referral resources. (PC, CS,<br />
SBP)<br />
6. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan that includes:<br />
Assessing the patient’s motivation for achieving sobriety/abstinence. (PC, MK)<br />
Understanding the principles <strong>of</strong> acute management <strong>of</strong> drug/alcohol intoxication and<br />
withdrawal versus long-term treatment planning. (MK, PC)<br />
Using Clinical Institute Withdrawal Assessment for Alcohol. (CIWA-Ar) scale in acute<br />
alcohol withdrawal to prevent seizures or delirium tremens (MK, PC)<br />
Recommending appropriate use <strong>of</strong> benzodiazepines for alcohol withdrawal. (MK, PC)<br />
186
Determining when to obtain consultation from a psychiatrist. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to substance abuse. (PC, PLI)<br />
Incorporating patient preferences and understanding limitations <strong>of</strong> treatment. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for substance abuse. (PLI,<br />
P)<br />
2. Respond appropriately to patients who are non-adherent to treatment for substance abuse.<br />
(CS, P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding substance abuse. (PLI,<br />
P)<br />
4. Appreciate the impact substance abuse has on a patient’s as well as a family’s quality <strong>of</strong> life,<br />
well-being, and ability to work. (P)<br />
5. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> substance abuse. (P, SBP)<br />
D. REFERENCES:<br />
U.S. Preventive Services Task Force. Screening and behavioral counseling<br />
interventions in primary care to reduce alcohol misuse recommendation statement. Ann<br />
Intern Med. 2004;140:554-6.<br />
Kosten TR, O'Connor PG. Management <strong>of</strong> drug and alcohol withdrawal. N Engl J Med.<br />
2003;348:1786-95.<br />
Mersy DJ. Recognition <strong>of</strong> alcohol and substance abuse. Am Fam Physician.<br />
2003;67:1529-32.<br />
187
TRAINING PROBLEM #33: VENOUS THROMBOEMBOLISM<br />
RATIONALE:<br />
Venous thromboembolic disease (DVT and PE) is a very common problem in internal medicine and<br />
one that can have devastating consequences if not appropriately diagnosed and treated. Diagnosis <strong>of</strong><br />
DVT and PE can be especially challenging. Prophylactic measures are very effective but do not<br />
eliminate the risk.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam (with particular attention to the<br />
cardiac, pulmonary, and venous systems).<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> the anatomy, physiology, and pathophysiology <strong>of</strong> the cardiac, pulmonary, and<br />
venous systems.<br />
Physiology and pathophysiology <strong>of</strong> the hemostatic system.<br />
Pharmacology <strong>of</strong> antithrombotic agents.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe and discuss:<br />
1. Risk factors for developing DVT, including:<br />
Prior history <strong>of</strong> DVT/PE. (MK)<br />
Immobility/hospitalization. (MK)<br />
Increasing age. (MK)<br />
Obesity. (MK)<br />
Trauma. (MK)<br />
Smoking. (MK)<br />
Surgery. (MK)<br />
Cancer. (MK)<br />
Acute MI. (MK)<br />
Stroke and neurologic trauma. (MK)<br />
Coagulopathy. (MK)<br />
Pregnancy. (MK)<br />
Oral estrogens. (MK)<br />
2. Genetic considerations predisposing to venous thrombosis. (MK)<br />
3. The symptoms and signs <strong>of</strong> DVT and PE. (MK)<br />
4. The differential diagnosis <strong>of</strong> DVT including the many causes <strong>of</strong> unilateral leg pain and swelling:<br />
Venous stasis and the postphlebitic syndrome. (MK)<br />
Lymphedema. (MK)<br />
Cellulitis. (MK)<br />
Superficial thrombophlebitis. (MK)<br />
Ruptured popliteal cyst. (MK)<br />
Musculoskeletal injury. (MK)<br />
Arterial occlusive disorders. (MK)<br />
5. The differential diagnosis <strong>of</strong> PE including the many causes <strong>of</strong> chest pain and dyspnea:<br />
188
MI/unstable angina. (MK)<br />
Congestive heart failure. (MK)<br />
Pericarditis. (MK)<br />
Pneumonia/bronchitis/COPD exacerbation. (MK)<br />
Asthma. (MK)<br />
Pulmonary hypertension. (MK)<br />
Pneumothorax. (MK)<br />
Musculoskeletal pain (e.g. rib fracture, costochondritis). (MK)<br />
6. Treatment modalities for DVT/PE, including:<br />
Unfractionated heparin. (MK)<br />
Low-molecular-weight heparin. (MK)<br />
Warfarin. (MK)<br />
Thrombolytics. (MK)<br />
7. The risks, benefits, and indications for inferior vena cava filters. (MK)<br />
8. The long-term sequelae <strong>of</strong> DVT and PE. (MK)<br />
9. Methods <strong>of</strong> DVT/PE prophylaxis, their indications and efficacy, including:<br />
Ambulation. (MK)<br />
Graded compression stockings. (MK)<br />
Pneumatic compression devices. (MK)<br />
Unfractionated heparin. (MK)<br />
Low-molecular-weight heparin. (MK)<br />
Warfarin. (MK)<br />
B. SKILLS: Students should demonstrate specific skills, including:<br />
1. History-taking skills: Students should be able to obtain, document and present an ageappropriate<br />
medical history that suggests the diagnosis <strong>of</strong> DVT or PE, including:<br />
The presence or absence <strong>of</strong> known risk factors. (PC, CS)<br />
Presence or absence <strong>of</strong> leg pain, swelling, warmth, discoloration, and palpable cord. (PC,<br />
CS)<br />
The presence or absence <strong>of</strong> dyspnea, chest pain, palpitations, cough, hemoptysis. (PC,<br />
CS)<br />
2. Physical exam skills: Students should be able to perform a physical examination to<br />
establish the diagnosis and severity <strong>of</strong> disease, including:<br />
Assessment <strong>of</strong> vital signs (i.e. hypotension, tachycardia, tachypnea, fever) and general<br />
appearance (i.e. degree <strong>of</strong> respiratory distress, anxiety). (PC)<br />
Accurate identification <strong>of</strong> leg swelling, erythema, warmth, and tenderness. (PC)<br />
Inspection for signs <strong>of</strong> lower extremity trauma, arthritis, or joint effusion. (PC)<br />
Identification <strong>of</strong> pleural friction rubs, wheezes, rales, rhonchi, and signs <strong>of</strong> pneumothorax.<br />
(PC)<br />
3. Differential diagnosis: Students should be able to generate a differential diagnosis<br />
for a patient suspected <strong>of</strong> having DVT/PE, recognizing specific history, physical examination<br />
and laboratory findings which suggest DVT/PE, including the disease states noted above. (PC,<br />
MK)<br />
4. Laboratory interpretation: Students should be able to recommend when to order diagnostic<br />
and laboratory tests and be able to interpret them, both prior to and after initiating treatment<br />
based on<br />
189
the differential diagnosis, including consideration <strong>of</strong> test cost and performance characteristics<br />
as well as patient preferences.<br />
Laboratory and diagnostic tests should include, where appropriate:<br />
Pulse oximetry. (PC, MK)<br />
12-lead ECG. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
ABG. (PC, MK)<br />
D-dimer. (PC, MK)<br />
Students should be able to define the indications for and interpret (with consultation)<br />
the results <strong>of</strong>:<br />
Duplex venous ultrasonography. (PC, MK)<br />
Ventilation perfusion (V/Q) scan. (PC, MK)<br />
CT angiography. (PC, MK)<br />
Pulmonary angiography. (PC, MK)<br />
Echocardiography. (PC, MK)<br />
5. Communication skills: Students should be able to:<br />
Communicate the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
his or her family. (PC, CS)<br />
Elicit questions from the patient and his or her family about the management plan. (PC, CS)<br />
6. Basic and advanced procedural skills: Students should be able to:<br />
Perform a 12-lead ECG. (PC)<br />
Obtain an ABG. (PC)<br />
7. Management skills: Students should be able to develop an appropriate evaluation and<br />
treatment plan for patients that includes:<br />
Outlining the acute and long-term treatment <strong>of</strong> isolated calf vein phlebitis, superficial<br />
thrombophlebitis, DVT, and thromboembolism, including appropriate use and monitoring <strong>of</strong><br />
heparin and warfarin. (MK,<br />
PC)<br />
Understanding the indications for placement <strong>of</strong> inferior vena cava filter, indications and<br />
complications <strong>of</strong> thrombolytic therapy, as well as indications for performing a<br />
hypercoaguability work-up. (PC, MK)<br />
Determining when to obtain consultation from a pulmonologist or interventional radiologist.<br />
(PC, MK)<br />
Using a cost-effective approach based on the differential diagnosis. (PC, SBP)<br />
Accessing and utilizing appropriate information systems and resources to help delineate<br />
issues related to venous thromboembolism. (PC, PLI)<br />
Incorporating patient preferences. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for venous<br />
thromboembolic disease. (PLI, P)<br />
2. Respond appropriately to patients who are non-adherent to treatment for venous<br />
thromboembolic disease. (CS, P)<br />
3. Demonstrate ongoing commitment to self-directed learning regarding venous thromboembolic<br />
disease. (PLI, P)<br />
4. Appreciate the impact venous thromboembolic disease has on a patient’s quality <strong>of</strong> life, well-<br />
190
eing, ability to work, and the family. (P)<br />
5. Recognize the importance and demonstrate a commitment to the utilization <strong>of</strong> other healthcare<br />
pr<strong>of</strong>essions in the treatment <strong>of</strong> venous thromboembolic disease. (P, SBP)<br />
D. REFERENCES:<br />
American College <strong>of</strong> Chest Physicians. The seventh ACCP conference on<br />
antithrombotic and thrombolytic therapy: evidence-based guidelines. Chest. 2004;126<br />
(Number 3 Supplement)<br />
www.chestjournal.org/content/vol126/3_suppl<br />
Spyropoulos AC. Emerging strategies in the prevention <strong>of</strong> venous thromboembolism in<br />
hospitalized medical patients. Chest. 2005;128:958-69.<br />
Stein PD, Hull RD, Patel KC, Olson RE, Ghali WA, Brant R, Biel RK, Bharadia V, Kalra<br />
NK. D-dimer for the exclusion <strong>of</strong> acute venous thrombosis and pulmonary embolism: a<br />
systematic review. Ann Intern Med. 2004;140:589-602.<br />
Bates SM, Ginsberg JS. Clinical practice. Treatment <strong>of</strong> deep-vein thrombosis. N Engl J<br />
Med. 2004;351:268-77.<br />
Fedullo PF. Tapson VF. Clinical practice. The evaluation <strong>of</strong> suspected pulmonary<br />
embolism. N Engl J Med. 2003;349:1247-56.<br />
191
GENERAL CLINICAL CORE COMPETENCIES IN INTERNAL MEDICINE<br />
#1 DIAGNOSTIC DECISION MAKING<br />
RATIONALE:<br />
Physicians are responsible for directing and conducting the diagnostic evaluation <strong>of</strong> a broad range <strong>of</strong><br />
patients, including patients seeking advice on prevention <strong>of</strong> and screening for disease and patients<br />
with acute and chronic illnesses. In a time <strong>of</strong> rapidly proliferating tests, medical students must learn<br />
how to design safe, expeditious, and cost-effective diagnostic evaluations. This requires welldeveloped<br />
diagnostic decision-making skills that incorporate probability-based thinking.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Required course in pathophysiology.<br />
Required course in clinical epidemiology and biostatistics.<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Key history and physical examination findings pertinent to the differential diagnosis. (MK)<br />
2. Information resources for determining diagnostic options for patients with common and<br />
uncommon medical problems. (MK, PLI)<br />
3. Key factors to consider when selecting from among diagnostic tests, including pretest<br />
probabilities, performance characteristics <strong>of</strong> tests (sensitivity, specificity, likelihood ratios), cost,<br />
risk, and patient preferences. (MK, P)<br />
4. The basics <strong>of</strong> the potential role <strong>of</strong> genetic information in diagnostic decision making. (MK)<br />
5. Relative cost <strong>of</strong> diagnostic tests. (MK)<br />
6. How critical pathways or practice guidelines can be used to guide diagnostic test ordering.<br />
(MK)<br />
7. The methods <strong>of</strong> deductive reasoning, forward thinking, and pattern recognition in clinical<br />
decision making. (MK)<br />
B. SKILLS: Students should demonstrate specific skills, including:<br />
1. Identifying problems with which a patient presents, appropriately synthesizing these into logical<br />
clinical syndromes. (PC)<br />
2. Identifying which problems are <strong>of</strong> highest priority. (PC)<br />
3. Formulating a differential diagnosis based on the findings from the history and physical<br />
examination. (PC)<br />
4. Using probability-based thinking and pattern recognition to identify the most likely diagnoses.<br />
(PC)<br />
5. Using the differential diagnosis to help guide diagnostic test ordering and sequencing. (PC)<br />
6. Using pretest probabilities and scientific evidence about performance characteristics <strong>of</strong> tests<br />
(sensitivity, specificity, likelihood ratios) to determine post-test probabilities according to the<br />
predictive value paradigm. (PC)<br />
7. Participating in selecting the diagnostic studies with the greatest likelihood <strong>of</strong> providing useful<br />
results at a reasonable cost. (PC)<br />
192
8. Communicating the prioritized differential diagnosis to the patient and his or her family. (CS)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Incorporate the patient’s perspective into diagnostic decision making. (P)<br />
2. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic tests. (P)<br />
3. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic tests. (PLI, P)<br />
4. Seek feedback regularly regarding diagnostic decision making and respond appropriately and<br />
productively. (P)<br />
5. Limit the chances <strong>of</strong> false positive/false negative results by demonstrating thoughtful test<br />
selection. (P)<br />
6. Appreciate the element <strong>of</strong> uncertainty in diagnostic testing, including the occurrence and<br />
causes <strong>of</strong> false positive and false negative results. (P)<br />
7. Appreciate the impact uncertainty may have on the patient. (P)<br />
8. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other health<br />
care pr<strong>of</strong>essionals in diagnostic decision making. (P, SBP)<br />
D. REFERENCES:<br />
Mark, DB. Decision-making in clinical medicine. In Kasper DL, Braunwald EB, Fauci AS, Hauser<br />
SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th ed. New York, NY:<br />
McGraw-Hill; 2005:6-13.<br />
Strauss SE, Richardson WS, Glasziou P, Haynes RB. Evidence Based <strong>Medicine</strong>: How to Practice<br />
and Teach EBM. 3rd ed. New York, NY: Churchill Livingstone; 2005.<br />
Primer to the Internal <strong>Medicine</strong> Clerkship A Guide Produced by the Clerkship Directors in Internal<br />
<strong>Medicine</strong> Clerkship Directors in Internal <strong>Medicine</strong><br />
www.im.org/CDIM/primer.htm<br />
Ferri FF. Differential diagnosis. In Ferri FF, ed. Practical Guide to the Care <strong>of</strong> the Medical Patient.<br />
6th ed. St. Louis, MO: Mosby; 2004:39-113.<br />
193
#2 CASE PRESENTATION<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
Communicating patient care information to colleagues and other health care pr<strong>of</strong>essionals is an<br />
essential skill regardless <strong>of</strong> specialty. Internists have traditionally given special attention to case<br />
presentation skills because <strong>of</strong> the comprehensive nature <strong>of</strong> patient evaluations and the various<br />
settings in which internal medicine is practiced. Students should develop facility with different types<br />
<strong>of</strong> case presentations: written and oral, new patient and follow-up, inpatient and outpatient.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Components <strong>of</strong> comprehensive and abbreviated case presentations (oral and written)<br />
and settings appropriate for each. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Prepare legible, comprehensive, and focused new patient workups that include the<br />
following features as clinically appropriate:<br />
Chief complaint. (PC, CS)<br />
Identifying data. (PC, CS)<br />
Concise history <strong>of</strong> the present illness organized chronologically, with minimal repetition,<br />
omission, or extraneous information, and including pertinent positives and negatives.<br />
(PC, CS)<br />
Past medical history, including relevant details. (PC, CS)<br />
Medications with dosages and frequencies, including herbals, supplements, and overthe-counter<br />
medications. (PC, CS)<br />
Allergies with specific details <strong>of</strong> the reaction. (PC, CS)<br />
Substance use, including tobacco, alcohol, and illicit drugs. (PC, CS)<br />
Family history. (PC, CS)<br />
Social history. (PC, CS)<br />
Review <strong>of</strong> symptoms. (PC, CS)<br />
A comprehensive physical examination with detail pertinent to the patient’s problem.<br />
(PC, CS)<br />
A succinct, prioritized, and where appropriate complete list <strong>of</strong> all problems identified by<br />
the history and physical examination. (PC, CS)<br />
A differential diagnosis (appropriate for the student’s level <strong>of</strong> training) for each problem<br />
that is neither over-inclusive or under-inclusive, addresses all reasonable possibilities,<br />
pays special attention to diagnoses that are potentially the most serious or lifethreatening,<br />
and is supported by the use <strong>of</strong> pertinent positives and negatives. (PC, CS)<br />
194
A diagnostic and treatment plan for each problem (appropriate for the student’s level <strong>of</strong><br />
training). (PC, CS)<br />
2. Orally present a new inpatient’s or outpatient’s case in a manner that includes the<br />
following characteristics:<br />
Logically and chronologically develops the history <strong>of</strong> the present illness and tells the<br />
patient’s “story.” (PC, CS)<br />
Summarizes the pertinent positives and negatives. (PC, CS)<br />
Succinctly presents past medical history, family history, social history, and review <strong>of</strong><br />
symptoms. (PC, CS)<br />
Includes a logical, organized, and prioritized differential diagnosis. (PC, CS)<br />
Includes diagnostic and therapeutic plans. (PC, CS)<br />
Can be made briefer when necessary. (PC, CS)<br />
Is presented as much from memory as possible with minimal reference to memory<br />
aids with the exception <strong>of</strong> highly important dates, diagnostic tests, laboratory values.<br />
(PC, CS)<br />
3. Orally present a follow-up inpatient’s or outpatient’s case in a manner that includes the<br />
following characteristics:<br />
Focused and very concise. (PC, CS)<br />
Problem-based. (PC, CS)<br />
Emphasizes pertinent new findings. (PC, CS)<br />
Includes diagnostic and therapeutic plans. (PC, CS)<br />
Can be made briefer when necessary. (PC, CS)<br />
Is presented as much from memory as possible with minimal reference to memory<br />
aids with the exception <strong>of</strong> highly important dates, diagnostic tests, laboratory values.<br />
(PC, CS)<br />
4. Produce inpatient or outpatient progress notes in a manner that includes the following<br />
characteristics:<br />
Is appropriately titled. (PC, CS)<br />
Includes a brief subjective that addresses new or changed patient symptoms. (PC,<br />
CS)<br />
Provides an accurate and succinct accounting <strong>of</strong> the objective data<br />
(e.g. vital signs, in/outs, telemetry monitoring, focused physical examination,<br />
laboratory results, and diagnostic tests). (PC, CS)<br />
Includes a prioritized problem list with a concise assessment and plan for each. (PC,<br />
CS)<br />
5. Select the mode <strong>of</strong> presentation that is most appropriate to the clinical situation (e.g.<br />
written vs. oral, long vs. short, etc.). (PC, CS)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate ongoing commitment to self-directed learning regarding case presentation<br />
skills by regularly seeking feedback on presentations. (PLI, P)<br />
2. Respond appropriately and productively to feedback regarding performance.<br />
(P)<br />
3. Accurately and objectively record and present all data. (P)<br />
195
4. Demonstrate respect for the patient’s privacy when dealing with protected health<br />
information and follow Health Information Portability and Accountability Act (HIPAA)<br />
standards. (P)<br />
D. REFERENCES:<br />
Primer to the Internal <strong>Medicine</strong> Clerkship A Guide Produced by the Clerkship Directors in<br />
Internal <strong>Medicine</strong> Clerkship Directors in Internal <strong>Medicine</strong><br />
www.im.org/CDIM/primer.htm<br />
Sobel RK. MSL – medicine as a second language. N Engl J Med. 2005;352:1945<br />
196
GENERAL CLINICAL CORE COMPETENCIES<br />
#3 HISTORY TAKING AND PHYSICAL EXAMINATION<br />
RATIONALE:<br />
The ability to obtain an accurate medical history and carefully perform a physical examination is<br />
fundamental to providing comprehensive care to adult patients. In particular, the internist must be<br />
thorough and efficient in obtaining a history and performing a physical examination with a wide variety<br />
<strong>of</strong> patients, including healthy adults (both young and old), adults with acute and chronic medical<br />
problems, adults with complex life-threatening diseases, and adults from diverse socioeconomic and<br />
cultural backgrounds. The optimal selection <strong>of</strong> diagnostic tests, choice <strong>of</strong> treatment, and use <strong>of</strong><br />
subspecialists, as well as the physician’s relationship and rapport with patients, all depend on welldeveloped<br />
history-taking and physical diagnosis skills. These skills, which are fundamental to<br />
effective patient care, should be a primary focus <strong>of</strong> the student’s work during the core <strong>clerkship</strong> in<br />
internal medicine.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience<br />
should include:<br />
Required pre-clinical courses in physical examination and physician-patient<br />
communication (should include instruction in breast, pelvic, rectal, and male genital exams).<br />
Ability to perform a complete medical history and physical exam on a wide variety <strong>of</strong><br />
patients including adolescents and older adults.<br />
Ability to effectively communicate with patients <strong>of</strong> diverse backgrounds.<br />
Basic skills for obtaining a history related to substance abuse, sexual, occupational,<br />
and mental health.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The significant attributes <strong>of</strong> a symptom, including: location and radiation, intensity, quality,<br />
temporal sequence (onset, duration, frequency), alleviating factors, aggravating factors,<br />
setting, associated symptoms, functional impairment, and patient’s interpretation <strong>of</strong> symptom.<br />
(MK)<br />
2. The four methods <strong>of</strong> physical examination (inspection, palpation, percussion, and<br />
auscultation), including where and when to use them, their purposes, and the findings they<br />
elicit. (MK)<br />
3. The physiologic mechanisms that explain key findings in the history and physical exam. (MK)<br />
4. The diagnostic value <strong>of</strong> the history and physical examination. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Using language appropriate for each patient. (PC, CS)<br />
2. Using non-verbal techniques to facilitate communication and pursue relevant inquiry. (PC, CS)<br />
3. Eliciting the patient’s chief complaint as well as a complete list <strong>of</strong> the patient’s concerns.<br />
(PC,CS)<br />
4. Obtaining a patient’s history in a logical, organized, and thorough manner, covering the<br />
following:<br />
197
History <strong>of</strong> present illness. (PC, CS)<br />
past medical history (including usual source <strong>of</strong> and access to health care, childhood and<br />
adult illnesses, injuries, surgical procedures, obstetrical history, psychiatric problems,<br />
sexual history, and hospitalizations). (PC, CS)<br />
Preventive health measures. (PC, CS)<br />
Medications with dosages and frequencies, including herbals, supplements, and overthe-counter<br />
medications. (PC, CS)<br />
Allergies with specific details <strong>of</strong> the reaction. (PC, CS)<br />
Substance use including tobacco, alcohol, and illicit drugs. (PC, CS)<br />
Family history. (PC, CS)<br />
Social history. (PC, CS)<br />
Occupational history. (PC, CS)<br />
Review <strong>of</strong> symptoms. (PC, CS)<br />
5. Obtaining, whenever necessary, supplemental historical information from collateral sources,<br />
such as significant others or previous physicians. (PC, CS)<br />
6. Demonstrating proper hygienic practices whenever examining a patient. (PC)<br />
7. Positioning the patient and self properly for each part <strong>of</strong> the physical examination. (PC)<br />
8. Performing a physical examination for a patient in a logical, organized, respectful, and<br />
thorough manner, including:<br />
The patient’s general appearance. (PC)<br />
Vital signs. (PC)<br />
Pertinent body regions/organ systems. (PC)<br />
When appropriate breast, pelvic, rectal, male genital exams. (PC)<br />
When appropriate fundoscopic exam. (PC)<br />
When appropriate full neurologic exam. (PC)<br />
9. Adapting the scope and focus <strong>of</strong> the history and physical exam appropriately to the medical<br />
situation and the time available. (PC)<br />
10. Being observant <strong>of</strong> the patient’s modesty as much as possible. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Appreciate the essential contribution <strong>of</strong> a pertinent and history and physical examination<br />
to patient care. (P)<br />
2. Demonstrate ongoing commitment to self-directed learning regarding history taking and<br />
physical examination skills. (PLI, P)<br />
3. Seek feedback regularly regarding history and physical examination skills and respond<br />
appropriately and productively. (P)<br />
4. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
health care pr<strong>of</strong>essions in obtaining a history and physical examination (e.g. interpreter<br />
services, advanced practice nurses, etc.). (P, SBP)<br />
5. Establish a habit <strong>of</strong> updating historical information and repeating important parts <strong>of</strong> the<br />
physical examination during follow-up visits. (P)<br />
6. Demonstrate consideration for the patient’s modesty, feelings, limitations, and<br />
sociocultural background whenever taking a history and performing a physical<br />
examination. (P)<br />
7. Appreciate that some patients will be very anxious about the physical examination,<br />
particularly the breast, pelvic, rectal, and male genital exams. (P)<br />
D. REFERENCES:<br />
198
McGee SR. Evidence-Based Physical Diagnosis. Philadelphia, PA: W. B. Saunders Company;<br />
2001.<br />
Bickley LS, Szilagyi PG. Bates’ Guide to Physical Examination and History Taking. 8th Edition.<br />
Philadelphia, PA: Lipincott Williams and Wilkens; 2002.<br />
The Auscultation Assistant<br />
www.med.ucla.edu/wilkes/intro.html<br />
Criley JM. The Physiologic Origin <strong>of</strong> Heart Sounds and Murmurs: The Unique Interactive Guide<br />
to Cardiac Diagnosis. Philadelphia, PA: Lippincott Williams and Wilkins; 1997.<br />
Heart Sounds and Cardiac Arrhythmias<br />
Medical Multimedia Laboratories<br />
www.blaufuss.org<br />
199
GENERAL CLINICAL CORE COMPETENCIES<br />
#4 COMMUNICATION AND RELATIONSHIPS WITH PATIENTS AND COLLEAGUES<br />
RATIONALE:<br />
The physician-patient relationship forms the core <strong>of</strong> the practice <strong>of</strong> internal medicine. Many<br />
physicians view it as the most satisfying aspect <strong>of</strong> their work. The medical interview and the<br />
relationship between physician and patient are important diagnostic and therapeutic tools. Effective<br />
communication skills are needed for a physician to serve as an effective patient advocate.<br />
Communication skills also are needed to address patient concerns and requests. Pr<strong>of</strong>iciency in<br />
communicating with patients results in increased patient and physician satisfaction, increased<br />
adherence to therapy, and reduced risk <strong>of</strong> malpractice claims. The student on the internal medicine<br />
<strong>clerkship</strong> interacts with a diverse array <strong>of</strong> patients, physicians, and other health team members,<br />
necessitating pr<strong>of</strong>iciency in communication and interpersonal skills. Students also witness how<br />
diversities <strong>of</strong> age, gender, race, culture, socioeconomic class, personality, and intellect require a<br />
sensitive and flexible approach. The result <strong>of</strong> pr<strong>of</strong>iciency in communication and interpersonal skills is<br />
increased satisfaction for both doctor and patient.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should<br />
include:<br />
Required pre-clinical courses in physician-patient communication.<br />
Ability to perform a complete medical history on a wide variety <strong>of</strong> patients, including adolescents<br />
and older adults.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Basic skills for obtaining a history related to substance abuse and sexual, occupational, and<br />
mental health.<br />
Basic skills for discussing issues relating to advance directives.<br />
Basic skills for breaking bad news.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. How patients’ and physicians’ perceptions, preferences, and actions are affected by<br />
cultural and psychosocial factors and how these factors affect the doctor-patient<br />
relationship. (MK, P)<br />
2. The role and contribution <strong>of</strong> each team member to the care <strong>of</strong> the patient. (MK, SBP)<br />
3. The role <strong>of</strong> psychosocial factors in team interactions. (MK)<br />
4. The role <strong>of</strong> the physician as patient advocate. (MK)<br />
5. Strategies for establishing positive patient-doctor relationships. (MK)<br />
6. Patient, physician, and system barriers to successfully negotiated treatment plans and<br />
patient adherence; strategies that may be used to overcome these barriers. (MK, SBP)<br />
6. Useful strategies when a communicating with patients via an interpreter. (MK)<br />
7. Basic techniques for breaking bad news. (MK)<br />
8. Basic tenants <strong>of</strong> genetic counseling. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
200
1. Demonstrating appropriate listening skills, including verbal and non-verbal techniques<br />
(e.g., restating, probing, clarifying, silence, eye contact, posture, touch) to communicate<br />
empathy and help educate the patient. (CS)<br />
2. Demonstrating effective verbal skills including appropriate use <strong>of</strong> open- and closedended<br />
questions, repetition, facilitation, explanation, and interpretation. (CS)<br />
3. Determining the information a patient has independently obtained about his or her<br />
problems. (CS)<br />
4. Identifying patients’ emotional needs. (CS)<br />
5. Respond to empathic opportunities by naming the emotions or feelings expressed. (CS)<br />
6. Eliciting the patient’s point <strong>of</strong> view and concerns about his or her illness and the medical<br />
care he or she is receiving. (CS)<br />
7. Discussing how the health problem affects the patient’s life. (CS)<br />
8. Determining the extent to which a patient wants to be involved in making decisions<br />
about his or her care. (CS)<br />
9. Providing basic information and an explanation <strong>of</strong> the diagnosis, prognosis, and<br />
treatment plan. (CS)<br />
10. Responding to patients’ concerns and expectations. (CS)<br />
11. With guidance and direct supervision, participating in breaking bad news to patients.<br />
(CS)<br />
12. With guidance and direct supervision, participating in discussing basic issues regarding<br />
advance directives with patients and their families. (CS)<br />
13. With guidance and direct supervision, participating in discussing basic end-<strong>of</strong> life issues<br />
with patients and their families. (CS)<br />
14. Assessing patient commitment and adherence to a treatment plan taking into account<br />
personal and economic circumstances. (CS)<br />
15. Working with a variety <strong>of</strong> patients, including multi-problem patients, angry patients,<br />
somatizing patients, and substance abuse patients. (CS)<br />
16. Working as an effective member <strong>of</strong> the patient care team, incorporating skills in interpr<strong>of</strong>essional<br />
communication and collaboration. (CS, SBP)<br />
17. Giving and receiving constructive feedback. (CS)<br />
18. Orally presenting a new inpatient’s or outpatient’s case in a manner that includes the<br />
following characteristics:<br />
Logically and chronologically develops the history <strong>of</strong> the present illness and tells<br />
the patient’s “story.” (PC, CS)<br />
Summarizes the pertinent positives and negatives. (PC, CS)<br />
Succinctly presents past medical history, family history, social history, and review<br />
<strong>of</strong> symptoms. (PC, CS)<br />
includes a logical, organized, and prioritized differential diagnosis (PC, CS)<br />
Includes diagnostic and therapeutic plans. (PC, CS)<br />
Can be made briefer when necessary. (PC, CS)<br />
Is presented as much from memory as possible with minimal reference to<br />
memory aids with the exception <strong>of</strong> highly important dates, diagnostic tests,<br />
laboratory values. (PC, CS)<br />
19. Orally presenting a follow-up inpatient’s or outpatient’s case in a manner that includes<br />
the following characteristics:<br />
Is focused, very concise, and problem-based. (PC, CS)<br />
Emphasizes pertinent new findings. (PC, CS)<br />
Includes diagnostic and therapeutic plans. (PC, CS)<br />
201
Can be made briefer when necessary. (PC, CS)<br />
Is presented as much from memory as possible with minimal reference to<br />
memory aids with the exception <strong>of</strong> highly important dates, diagnostic tests, and<br />
laboratory values. (PC, CS)<br />
20. Demonstrating the ability to make clear and concise presentations about topics<br />
assigned to research. (CS)<br />
21. Demonstrating basic strategies for conflict management and resolution. (CS)<br />
22. Demonstrating basic techniques <strong>of</strong> communication with non-English speaking patient<br />
via an interpreter. (PC, CS)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate ongoing commitment to self-directed learning regarding effective doctorpatient<br />
communication skills. (PLI, P)<br />
2. Seek feedback regularly regarding communication skills and respond appropriately and<br />
productively. (P)<br />
3. take into consideration in each case the patient’s psychosocial status (P)<br />
4. Demonstrate respect for patients. (P)<br />
5. Involve the patient actively in his or her health care whenever possible. (P)<br />
6. Demonstrate teamwork and respect toward all members <strong>of</strong> the health care team, as<br />
manifested by reliability, responsibility, honesty, helpfulness, selflessness, and initiative<br />
in working with the team. (SBP, P)<br />
7. Attend to or advocate for the patient’s interests and needs in a manner appropriate to<br />
the student’s role. (P)<br />
8. Maintain confidentiality when dealing with protected health information and follow Health<br />
Information Portability and Accountability Act (HIPAA) guidelines. (P, SBP)<br />
D. REFERENCES:<br />
Clinician-Patient Communication to Enhance Health Outcomes. Institute for Health Care<br />
communication, Inc., West Haven, Connecticut, 1998.<br />
www.healthcarecomm.org<br />
Contemporary Issues in <strong>Medicine</strong>: Communication in <strong>Medicine</strong> Medical School Objectives<br />
Project, October 1999 American Association <strong>of</strong> Medical Colleges<br />
www.aamc.org/meded/msop/msop3.pdf<br />
Kurtz S, Silverman J, Draper J. Teaching and Learning Communication Skills in <strong>Medicine</strong>.<br />
Oxford: Radcliffe Medical Press Ltd; 1998.<br />
Kurtz S, Silverman J, Benson J, Draper J. Marrying content and process in clinical method<br />
teaching: enhancing the Calgary-Cambridge guides. Acad Med. 2003;78:802-9.<br />
Makoul G. The SEGUE Framework for teaching and assessing<br />
communication skills. Patient Educ Couns. 2001;45:23-34.<br />
Makoul G. Essential elements <strong>of</strong> communication in medical encounters: the Kalamazoo<br />
consensus statement. Acad Med. 2001;76:390-3.<br />
von Gunten CF, Ferris FD, Emanuel LL. Ensuring competency in end-<strong>of</strong>-life care:<br />
communication and relational skills. JAMA. 2000;284:3051-7.<br />
202
GENERAL CLINICAL CORE COMPETENCIES<br />
#5 INTERPRETATION OF CLINICAL INFORMATION<br />
RATIONALE:<br />
In the routine course <strong>of</strong> clinical practice, most physicians are required to order and interpret a wide<br />
variety <strong>of</strong> diagnostic tests and procedures. Determining how these test results will influence clinical<br />
decision making and communicating this information to patients in a timely and effective manner are<br />
core clinical skills that third-year medical students should possess.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Introductory course in clinical pathology and laboratory medicine.<br />
Introductory course in epidemiology and biostatistics.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to:<br />
1. Interpret specific diagnostic tests and procedures that are ordered to evaluate patients who<br />
present with common symptoms and diagnoses encountered in the practice <strong>of</strong> internal<br />
medicine. (PC, MK)<br />
2. Take into account:<br />
Important differential diagnostic considerations, including potential diagnostic<br />
emergencies. (PC, MK)<br />
Pre-test and post-test likelihood <strong>of</strong> disease (probabilistic reasoning). (PC, MK)<br />
Performance characteristics <strong>of</strong> individual tests. (sensitivity, specificity, positive and<br />
negative predictive value, likelihood ratios). (PC, MK)<br />
3. Define and describe for the tests and procedures listed:<br />
Indications for testing. (PC, MK)<br />
Range <strong>of</strong> normal variation. (PC, MK)<br />
Critical values that require immediate attention. (PC, MK)<br />
Pathophysiologic implications <strong>of</strong> abnormal results. (PC, MK)<br />
Relative cost. (MK, SBP)<br />
4. Independently interpret the results <strong>of</strong> the following laboratory tests:<br />
CBC with diff and blood smear. (PC, MK)<br />
UA. (PC, MK)<br />
Electrolytes. (PC, MK)<br />
BUN/Cr. (PC, MK)<br />
GLC. (PC, MK)<br />
Hepatic function panel. (PC, MK)<br />
Hepatitis serologies. (PC, MK)<br />
Cardiac biomarkers (e.g. myoglobin, CK-MB, and Troponin I/T). (PC, MK)<br />
Routine coagulation tests (e.g. PT/PTT and INR). (PC, MK)<br />
Thyroid function tests (e.g. T3, T4, and TSH). (PC, MK)<br />
ABG.(PC, MK)<br />
Body fluid cell counts and chemistries. (PC, MK)<br />
5. Independently interpret the results <strong>of</strong> the following diagnostic procedures:<br />
203
12-lead ECG. (PC, MK)<br />
Chest radiograph. (PC, MK)<br />
Plain abdominal films (e.g. obstructive series, KUB). (PC, MK)<br />
Pulmonary function tests. (PC, MK)<br />
6. Describe the basic electrophysiologic events that produce the surface ECG. (MK)<br />
7. Describe how errors in test interpretation can affect clinical outcomes and costs. (PC, MK)<br />
8. Describe the concept <strong>of</strong> a threshold as it relates to testing and treatment decisions. (PC, MK)<br />
9. Describe the basic principles <strong>of</strong> using genetic information in clinical decision making. (PC, MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Interpreting a blood smear, Gram stain, and UA. (PC)<br />
2. Approaching ECG interpretation in a systematic and logical fashion analyzing the following:<br />
rate, rhythm, P wave morphology, PR interval, QRS width, axis, voltage, QT interval, ST<br />
segment morphology, and T wave morphology. (PC)<br />
3. Recognizing the following on ECG:<br />
Sinus tachycardia, sinus bradycardia, sinus arrhythmia. (PC)<br />
Premature atrial beats, ectopic atrial rhythm/tachycardia, narrow complex supraventricular<br />
tachycardia. (PC)<br />
Multifocal atrial tachycardia, atrial flutter, atrial fibrillation (PC)<br />
First degree, second degree (Mobitz type I and II), and third degree (complete) heart<br />
block. (PC)<br />
Junctional rhythm. (PC)<br />
Premature ventricular beats. (PC)<br />
Typical ventricular tachycardia, ventricular fibrillation. (PC)<br />
Left and right atrial enlargement. (PC)<br />
Left ventricular hypertrophy. (PC)<br />
Left and right bundle branch block, left anterior and posterior fascicular block. (PC)<br />
The characteristic features <strong>of</strong> a properly functioning ventricular or dual chamber<br />
pacemaker. (PC)<br />
The delta wave in Wolf-Parkinson-White Syndrome. (PC)<br />
The classic features <strong>of</strong> myocardial ischemia and infarction and be able to localize the<br />
findings (i.e. inferior, anterior, lateral, posterior, right ventricular) and identify the probable<br />
culprit vessel. (PC)<br />
The classic features <strong>of</strong> pulmonary embolism. (PC)<br />
The characteristic effects <strong>of</strong> hypo- and hyperkalemia. (PC)<br />
4. Approaching chest radiography interpretation in a systematic and logical fashion analyzing the<br />
following: technique (e.g. view, rotation, exposure), visible abdomen, s<strong>of</strong>t tissues and bones <strong>of</strong><br />
the thorax, mediastinum/hila, and lungs. (PC)<br />
5. Recognizing the following on chest radiograph:<br />
Rib fracture. (PC)<br />
Cardiomegaly. (PC)<br />
Lobar pneumonia. (PC)<br />
Pleural effusion. (PC)<br />
Pneumothorax. (PC)<br />
Pulmonary nodule. (PC)<br />
204
Pulmonary edema/“congestive heart failure” (e.g. cardiomegaly, pulmonary vascular<br />
redistribution, Kerley’s B Lines, interstitial/alveolar edema). (PC)<br />
Hilar lymphadenopathy. (PC)<br />
Mediastinal widening. (PC)<br />
6. Recording the results <strong>of</strong> laboratory tests in an organized manner, using flow sheets when<br />
appropriate. (PC)<br />
7. Estimating the pre-test likelihood <strong>of</strong> a disease or condition. (PC, MK)<br />
8. Estimating the post-test probability <strong>of</strong> disease and stating the clinical significance <strong>of</strong> the results<br />
<strong>of</strong> laboratory tests and diagnostic procedures. (PC, MK)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for acute MI. (PLI, P,<br />
SBP)<br />
2. Regularly seek feedback regarding interpretation <strong>of</strong> clinical information and respond<br />
appropriately and productively. (P)<br />
3. Recognize the importance <strong>of</strong> patient preferences when selecting among diagnostic testing<br />
options. (P)<br />
4. Demonstrate ongoing commitment to self-directed learning regarding test interpretation. (PLI,<br />
P)<br />
5. Appreciate the implications <strong>of</strong> test results before ordering tests. (P)<br />
6. Appreciate the importance <strong>of</strong> follow-up on all diagnostic tests and procedures and timely<br />
communication <strong>of</strong> information to patients and appropriate team members. (P)<br />
7. Demonstrate a commitment to excellence by personally reviewing radiographs, ECGs, Gram<br />
stains, blood smears, etc. to assess the accuracy and significance <strong>of</strong> the results. (P)<br />
D. REFERENCES:<br />
Jaeschke R, Guyatt G, Sackett DL. Users’ guides to the medical literature.<br />
III. How to use an article about a diagnostic test. A. Are the results <strong>of</strong> the study valid? JAMA.<br />
1994; 271:389-91.<br />
Jaeschke R, Guyatt G, Sackett DL. Users’ guides to the medical literature.<br />
III. How to use an article about a diagnostic test. B. What are the results and will they help me<br />
in caring for my patients? JAMA. 1994; 271: 703-7.<br />
Dubin D. Rapid Interpretation <strong>of</strong> EKG's. 5th ed. Tampa, FL: Cover Publishing Company; 2000.<br />
Goodman LR. Felson’s Principles <strong>of</strong> Chest Roentgenology: A Programmed Text. 2nd ed.<br />
Philadelphia, PA: W. B. Saunders; 1999.<br />
Novelline RA. Squire's Fundamentals <strong>of</strong> Radiology. 6th ed. Cambridge, MA: <strong>University</strong> Press;<br />
2004.<br />
Mark, DB. Decision-making in clinical medicine. In Kasper DL, Braunwald EB, Fauci AS,<br />
Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th ed.<br />
New York: McGraw-Hill; 2005:6-13.<br />
Lab Test Online<br />
www.labtestsonline.org/<br />
RadQuiz: Your Gateway to Radiology Resources<br />
www.radquiz.com<br />
Introduction to Chest Radiology<br />
205
<strong>Department</strong> <strong>of</strong> Radiology<br />
<strong>University</strong> <strong>of</strong> Virginia Health Sciences Center<br />
www.med-ed.virginia.edu/courses/rad/cxr/index.html<br />
Ferri FF. Laboratory values and interpretation <strong>of</strong> results. In Ferri FF, ed. Practical Guide to<br />
the Care <strong>of</strong> the Medical Patient. 6th ed. St. Louis, MO: Mosby; 2004:935-976.<br />
206
#6 THERAPEUTIC DECISION MAKING<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
Internists are responsible for directing and coordinating the therapeutic management <strong>of</strong> patients with<br />
a wide variety <strong>of</strong> problems, including critically ill patients with complex medical problems and the<br />
chronically ill. To manage patients effectively, physicians need basic therapeutic decision-making<br />
skills that incorporate both pathophysiologic reasoning and evidence-based knowledge.<br />
PREREQUISITES:<br />
Introductory coursework in clinical epidemiology and biostatistics.<br />
Introductory coursework in physiology and pathology.<br />
Introductory coursework in pharmacology.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Information resources for determining medical and surgical treatment options for patients<br />
with common and uncommon medical problems. (MK)<br />
2. Key factors to consider in choosing among treatment options, including risk, cost, evidence<br />
about efficacy, and consistency with pathophysiologic reasoning (MK)<br />
3. How to use critical pathways and clinical practice guidelines to help guide therapeutic<br />
decision making. (MK)<br />
4. Factors that frequently alter the effects <strong>of</strong> medications, including drug interactions and<br />
compliance problems. (MK)<br />
5. Factors to consider in selecting a medication from within a class <strong>of</strong> medications. (MK)<br />
6. Factors to consider in monitoring a patient’s response to treatment, including potential<br />
adverse effects. (MK)<br />
7. Various ways that evidence about clinical effectiveness is presented to clinicians and the<br />
potential biases <strong>of</strong> using absolute or relative risk or number <strong>of</strong> patients needed to treat. (MK)<br />
8. Methods <strong>of</strong> monitoring therapy and how to communicate them in both written and oral form.<br />
(MK)<br />
9. The basics <strong>of</strong> the potential role <strong>of</strong> genetic information in therapeutic decision making. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Formulating an initial therapeutic plan. (PC)<br />
2. Changing the therapeutic plan when goals <strong>of</strong> care change (e.g. a shift toward palliative<br />
care). (PC)<br />
3. Accessing and utilizing, when appropriate, information resources to help develop an<br />
appropriate and timely therapeutic plan. (PC, PLI)<br />
4. Explaining the extent to which the therapeutic plan is based on pathophysiologic reasoning<br />
and scientific evidence <strong>of</strong> effectiveness. (PC)<br />
5. Beginning to estimate the probability that a therapeutic plan will produce the desired<br />
outcome. (PC)<br />
6. Writing prescriptions and inpatient orders safely and accurately. (PC)<br />
7. Counseling patients about how to take their medications and what to expect<br />
when doing so, including beneficial outcomes and potential adverse effects. (PC, CS)<br />
207
8. Monitoring response to therapy. (PC)<br />
9. Recognizing when to seek consultation for additional diagnostic and therapeutic<br />
recommendations. (PC, SBP)<br />
10. Recognizing when to screen for certain conditions based on age and risk factors and what<br />
to do with the results <strong>of</strong> the screening tests. (PC)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
consideration in the selection <strong>of</strong> therapeutic interventions. (PLI, P)<br />
2. Demonstrate ongoing commitment to self-directed learning regarding therapeutic<br />
interventions. (PLI, P)<br />
3. Seek feedback regularly regarding therapeutic decision making and respond appropriately<br />
and productively. (P)<br />
4. Appreciate the impact therapeutic decisions have on a patient’s quality <strong>of</strong> life (P)<br />
5. Incorporate the patient in therapeutic decision making, explaining the risks and benefits <strong>of</strong><br />
treatment. (CS, P)<br />
6. Respect patients’ autonomy and informed choices, including the right to refuse treatment.<br />
(P)<br />
7. Demonstrate an understanding <strong>of</strong> the importance <strong>of</strong> close follow-up <strong>of</strong> patients under active<br />
care. (P)<br />
8. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other<br />
health care pr<strong>of</strong>essionals in therapeutic decision making. (P, SBP)<br />
D. REFERENCES:<br />
Mark, DB. Decision-making in clinical medicine. In Kasper DL, Braunwald EB, Fauci AS,<br />
Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th ed.<br />
New York: McGraw-Hill; 2005:6-13.<br />
Roden DM. Principles <strong>of</strong> clinical pharmacology. In Kasper DL, Braunwald EB, Fauci AS,<br />
Hauser SL, Longo DL, Jameson JL, eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th ed.<br />
New York: McGraw-Hill; 2005:13-25.<br />
Users' guides to the medical literature. II. How to use an article about therapy or prevention. A.<br />
Are the results <strong>of</strong> the study valid? Evidence-Based <strong>Medicine</strong> Working Group. JAMA.<br />
1993;270:2598-601.<br />
Users' guides to the medical literature. II. How to use an article about therapy or prevention. B.<br />
What were the results and will they help me in caring for my patients? Evidence-Based<br />
<strong>Medicine</strong> Working Group. JAMA. 1994;271:59-63.<br />
#7 BIOETHICS OF CARE<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
A basic understanding <strong>of</strong> ethical principles and their application to patient care is essential for all<br />
physicians. During the internal medicine core <strong>clerkship</strong>, the student can put into practice some <strong>of</strong> the<br />
ethical principles learned in the preclinical years, especially by participating in discussions <strong>of</strong> informed<br />
208
consent and advance directives. Additionally, the student learns to recognize ethical dilemmas and<br />
respect different perceptions <strong>of</strong> health, illness, and health care held by patients <strong>of</strong> various religious<br />
and cultural backgrounds.<br />
PREREQUISITES:<br />
Introductory course on medical ethics providing a basic understanding <strong>of</strong> ethical principles and<br />
fiduciary relationships and their application in clinical medicine:<br />
Autonomy.<br />
Beneficence.<br />
Nonmaleficence.<br />
Truth-telling.<br />
Confidentiality.<br />
Respect for autonomy (informed choice).<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Basic ethical principles (autonomy, beneficence, nonmaleficence, truth-telling, confidentiality,<br />
and autonomy). (MK)<br />
2. The patient’s right to refuse care. (MK)<br />
3. The unique nature <strong>of</strong> a fiduciary relationship. (MK)<br />
4. Basic elements <strong>of</strong> informed consent. (MK)<br />
5. Circumstances under which informed consent is necessary and unnecessary (MK)<br />
6. Basic concepts <strong>of</strong> treatment efficacy, quality <strong>of</strong> life, and societal demands. (MK)<br />
7. Potential conflicts between individual patient preferences and societal demands (MK)<br />
8. The role <strong>of</strong> the physician in making decisions about the use <strong>of</strong> expensive or controversial tests<br />
and treatments. (MK)<br />
9. Bioethical concerns regarding genetic information, privacy issues in particular. (MK)<br />
10. The unique bioethical concerns regarding end-<strong>of</strong>-life care. (MK)<br />
11. Circumstances when withholding or withdrawing care is acceptable. (MK)<br />
12. The role <strong>of</strong> federal and state legislation in governing health care. (MK)<br />
13. Circumstances when it may be unavoidable or acceptable to breach the basic ethical<br />
principles. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Participating in a discussion about advance directives with a patient. (PC, CS)<br />
2. Participating in obtaining informed consent for a procedure. (PC, CS)<br />
3. Participating in explaining and obtaining informed consent for genetic testing (PC, CS)<br />
4. Participating in a preceptor’s discussion with a patient about a requested<br />
treatment that may not be considered appropriate (e.g., not cost-effective). (PC, CS)<br />
5. Participating in family and interdisciplinary team conferences discussing end<strong>of</strong>-life<br />
care and incorporating the patient’s wishes in that discussion. (PC, CS, SBP)<br />
6. Obtaining additional help from ethics experts in conflict resolution. (PC, SBP)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
209
1. Demonstrate ongoing commitment to self-directed learning regarding bioethics. (PLI)<br />
2. Recognize the importance <strong>of</strong> patient preferences, perspectives, and perceptions regarding<br />
health and illness. (P)<br />
3. Demonstrate a commitment to caring for all patients, regardless <strong>of</strong> the medical diagnosis,<br />
gender, race, socioeconomic status, intellect/level <strong>of</strong> education, religion, political affiliation,<br />
sexual orientation, ability to pay, or cultural background. (P)<br />
4. Recognize the importance <strong>of</strong> allowing terminally ill patients to die with comfort and dignity<br />
when that is consistent with the wishes <strong>of</strong> the patient and/or the patient’s family. (P)<br />
5. Recognize the potential conflicts between patient expectations and medically appropriate care.<br />
(P)<br />
6. Respond appropriately to patients who are nonadherent to treatment. (P)<br />
7. Demonstrate respect for the patient’s privacy and confidentiality when dealing with protected<br />
health information and follow HIPAA standards. (P)<br />
8. Appreciate the psychological impact genetic information may have on patients. (P)<br />
D. REFERENCES:<br />
Bioethics Resources on the Web<br />
Inter-Institute Bioethics Interest Group<br />
National Institutes <strong>of</strong> Health<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.nih.gov/sigs/bioethics/<br />
<strong>University</strong> <strong>of</strong> Pennsylvania Center for Bioethics<br />
www.bioethics.upenn.edu<br />
Snyder L, Leffler C, Ethics and Human Rights Committee, American College <strong>of</strong> Physicians.<br />
Ethics manual: fifth edition. Ann Intern Med. 2005;142:560-82.<br />
World Medical Association Ethics Unit<br />
www.wma.net/e/ethicsunit/resources.htm<br />
Ethics in <strong>Medicine</strong> <strong>University</strong> <strong>of</strong> Washington School <strong>of</strong> <strong>Medicine</strong><br />
eduserv.hscer.washington.edu/bioethics<br />
Program in Ethics In Science and <strong>Medicine</strong> <strong>University</strong> <strong>of</strong> Texas Southwestern Medical Center<br />
www3.utsouthwestern.edu/ethics/<br />
Virtual Mentor American Medical Association<br />
www.ama-assn.org/ama/pub/category/3040.html<br />
Bioethics Interest Group American Medical Student Association<br />
www.amsa.org/bio/index.cfm<br />
210
#8 SELF-DIRECTED LEARNING<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
Because <strong>of</strong> the breadth <strong>of</strong> the problems encountered in clinical practice, internists face an<br />
extraordinary challenge to keep up with the burgeoning amount <strong>of</strong> new information relevant to<br />
providing high quality care. Therefore, they must master and practice self-directed life-long learning,<br />
including the ability to access and utilize information systems and resources efficiently.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Basic library skills, including the ability to perform an electronic literature search.<br />
Critical appraisal skills.<br />
Understanding <strong>of</strong> basic concepts <strong>of</strong> biostatistics and clinical epidemiology including: sensitivity,<br />
specificity, positive predictive value, negative predictive value, absolute risk reduction, relative<br />
risk reduction, number needed to treat, likelihood/odds ratios, and tests <strong>of</strong> significance.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Key sources for obtaining updated information on issues relevant to the medical management<br />
<strong>of</strong> adult patients. (MK, PLI)<br />
2. A system for managing information from a variety <strong>of</strong> sources. (MK, PLI)<br />
3. The concept <strong>of</strong> the focused clinical question. (MK, PLI)<br />
4. Key questions to ask when critically appraising articles on diagnostic tests:<br />
Was there an independent, blind comparison with a reference (“gold”) standard? (MK,<br />
PLI)<br />
Was the diagnostic test evaluated in an appropriate spectrum <strong>of</strong> patients (like those in<br />
whom it would be used in practice)? (MK, PLI)<br />
Was the reference standard applied regardless <strong>of</strong> the diagnostic test result? (MK, PLI)<br />
What were the results <strong>of</strong> the study (e.g. sensitivity, specificity, likelihood ratios, and/or<br />
pre- and post-test probabilities)? (MK, PLI)<br />
5. Key questions to ask when critically appraising articles on medical therapeutics:<br />
Was the assignment <strong>of</strong> patients to treatments randomized? (MK, PLI)<br />
Were all patients who entered the trial properly accounted for at the conclusion <strong>of</strong> the<br />
study and analyzed in the group they were randomized to? (MK, PLI)<br />
Were patients and study personnel blind to the treatment? (MK, PLI)<br />
Were the groups similar at the start <strong>of</strong> the trial? (MK, PLI)<br />
Aside from the experimental intervention, were the groups treated equally? (MK, PLI)<br />
What were the results <strong>of</strong> the trial (e.g. relative risk reduction, absolute risk reduction, and<br />
“number needed to treat”)? (MK, PLI)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
211
1. Performing a computerized literature search to find articles pertinent to a focused clinical<br />
question. (PLI)<br />
2. Demonstrating critical review skills. (PLI)<br />
3. Reading critically about issues pertinent to their patients. (PLI)<br />
4. Assessing the limits <strong>of</strong> medical knowledge in relation to patient problems (PLI)<br />
5. Using information from consultants critically. (PLI)<br />
6. Recognizing when additional information is needed to care for the patient (PLI)<br />
7. Asking colleagues (students, residents, nurses, faculty) for help when needed (PLI, SBP)<br />
8. Making use <strong>of</strong> available instruments to assess one’s own knowledge base (PLI, P)<br />
9. Summarizing and presenting to colleagues what was learned from consulting the medical<br />
literature. (PLI, CS)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate self-directed learning in every case. (PLI, P)<br />
2. Acknowledge gaps in knowledge to both colleagues and patients and request help. (PLI, P)<br />
3. Seek feedback regularly and respond appropriately and productively. (P)<br />
4. Recognize the value and limitations <strong>of</strong> other health care pr<strong>of</strong>essionals when confronted with a<br />
knowledge gap. (PLI, P, SBP)<br />
D. REFERENCES:<br />
Users' guides to the medical literature. I. How to get started. The Evidence-Based <strong>Medicine</strong><br />
Working Group. JAMA. 1993;270:2093-5.<br />
Users' guides to the medical literature. II. How to use an article about therapy or prevention. A.<br />
Are the results <strong>of</strong> the study valid? Evidence-Based <strong>Medicine</strong> Working Group. JAMA.<br />
1993;270:2598-601.<br />
Users' guides to the medical literature. II. How to use an article about therapy or prevention. B.<br />
What were the results and will they help me in caring for my patients? Evidence-Based<br />
<strong>Medicine</strong> Working Group. JAMA. 1994;271:59-63.<br />
Users' guides to the medical literature. III. How to use an article about a diagnostic test. A. Are<br />
the results <strong>of</strong> the study valid? Evidence-Based <strong>Medicine</strong> Working Group. JAMA.<br />
1994;271:389-91.<br />
Users' guides to the medical literature. III. How to use an article about a diagnostic test. B.<br />
What are the results and will they help me in caring for my patients? The Evidence-Based<br />
<strong>Medicine</strong> Working Group. JAMA. 1994;271:703-7.<br />
Strauss SE, Richardson WS, Glasziou P, Haynes RB. Evidence Based <strong>Medicine</strong>: How to<br />
Practice and Teach EBM. 3rd ed. New York, NY: Churchill Livingstone; 2005.<br />
Advancing Education in Practice-Based Learning and Improvement An Educational Resource<br />
from the ACGME Outcome Project<br />
www.acgme.org/outcome/implement/complete_PBLIBooklet.pdf<br />
#9 PREVENTION<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
One <strong>of</strong> the most important responsibilities <strong>of</strong> primary care physicians is to promote health and prevent<br />
disease in a cost-effective manner. Appropriate care by internists includes not only recognition and<br />
212
treatment <strong>of</strong> disease but also the routine incorporation <strong>of</strong> the principles <strong>of</strong> preventive health care into<br />
clinical practice. All physicians should be familiar with the principles <strong>of</strong> preventive health care to<br />
ensure their patients receive appropriate preventive services.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should include:<br />
Introductory course in clinical epidemiology and biostatistics.<br />
Introductory course in health promotion and disease prevention.<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Primary, secondary, and tertiary prevention. (MK)<br />
2. Criteria for determining whether or not a screening test should be incorporated into the periodic<br />
health assessment <strong>of</strong> adults. (MK)<br />
3. General types <strong>of</strong> preventive health care issues that should be addressed on a routine basis in<br />
adult patients (i.e., cancer screening; prevention <strong>of</strong> infectious diseases, coronary artery<br />
disease, osteoporosis, and injuries; and identification <strong>of</strong> substance abuse). (MK)<br />
4. Vaccines that have been recommended for routine use in at least some adults (i.e., influenza,<br />
pneumococcal, measles, mumps, rubella, tetanus-diphtheria, hepatitis). (MK)<br />
5. Indications for endocarditis prophylaxis. (MK)<br />
6. Methods for counseling patients about risk-factor modification, including the “stages <strong>of</strong> change”<br />
approach to helping patients change behavior. (MK)<br />
7. Influence <strong>of</strong> age and clinical status on approach to prevention. (MK)<br />
8. General categories <strong>of</strong> high-risk patients in whom routine preventative health care must be<br />
modified or enhanced (e.g., family history, travel to an underdeveloped area, occupational<br />
exposures, etc.). (MK)<br />
9. The major areas <strong>of</strong> controversy in screening. (MK)<br />
10. The potential roles and limitations <strong>of</strong> genetic testing in disease<br />
prevention/early detection. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Obtaining a patient history, including a detailed family history, vaccination history, travel<br />
history, sexual history, and occupational exposures. (PC)<br />
2. Identifying patients at high risk for developing diabetes, dyslipidemia, coronary artery disease,<br />
cancer, osteoporosis, influenza, pneumonia, hepatitis, HIV infection, and tuberculosis by<br />
screening for major risk factors. (PC)<br />
3. Obtaining a Pap smear and interpreting its results. (PC)<br />
4. Performing a breast examination. (PC)<br />
5. Instructing patients to perform breast self-examination. (PC, CS)<br />
6. Interpreting the results <strong>of</strong> a mammogram. (PC)<br />
7. Performing a digital rectal examination. (PC)<br />
8. Interpreting the results <strong>of</strong> a PSA test and understand its limitations. (PC)<br />
9. Performing a testicular examination. (PC)<br />
10. Interpreting the results <strong>of</strong> a bone densitometry test. (PC)<br />
11. Interpreting the results <strong>of</strong> a fasting lipid pr<strong>of</strong>ile. (PC)<br />
213
12. Interpreting the results <strong>of</strong> a fasting glucose test. (PC)<br />
13. Counseling patients about safe-sex practices, smoking cessation, alcohol abuse, weight loss,<br />
healthy diet, exercise, and seat belt use. (PC, CS)<br />
14. place and interpret a PPD. (PC)<br />
15. Locating recently published recommendations as well as original data regarding measures that<br />
should be incorporated into the periodic health assessment <strong>of</strong> adults. (PLI)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Address preventive health care issues as a routine part <strong>of</strong> their assessment <strong>of</strong> patients. (P)<br />
2. Encourage patients to share responsibility for health promotion and disease prevention. (P)<br />
3. Recognize the importance <strong>of</strong> patient preferences when recommending preventive health<br />
measures. (P)<br />
4. Understand the patient’s right to refuse preventive health measures. (P)<br />
5. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection preventive health measures. (PLI, P)<br />
6. Demonstrate ongoing commitment to self-directed learning regarding preventive health<br />
measures. (PLI, P)<br />
D. REFERENCES:<br />
Pomrehn PR, Davis MV, Chen DW, Barker W. Prevention for the 21st century: setting the<br />
context through undergraduate medical education. Acad Med. 2000;75(7 Suppl):S5-13.<br />
Guide to Clinical Preventive Services<br />
U.S. Preventative Services Task Force (USPSTF)<br />
Agency for Healthcare Research and Quality<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
USPSTF Recommendation: Screening for Cancer<br />
www.ahrq.gov/clinic/cps3dix.htm#cancer<br />
USPSTF Recommendation: Screening for Lipid Disorders<br />
www.ahrq.gov/clinic/ajpmsuppl/lipidrr.htm<br />
USPSTF Recommendation: Screening for High Blood Pressure<br />
www.ahrq/clinic/3rduspstf/highbloodsc/hibloodrr.htm<br />
USPSTF Recommendations Statement: Counseling to prevent tobacco use and tobaccocaused<br />
disease<br />
www.ahrq.gov/clinic/3rduspstf/tobaccoun/tobcounrs.htm<br />
Screening for Prostate Cancer. American College <strong>of</strong> Physicians. Ann Int Med 1997; 126: 480-<br />
484.<br />
Summary <strong>of</strong> Recommendations for Adult Immunization Immunization Action Coalition Bulletin<br />
Adapted from the recommendations <strong>of</strong> the Advisory Commttee on Immunization Practices<br />
(ACIP), August 2005<br />
www.immunize.org/acip<br />
Martin GJ. Screening and prevention <strong>of</strong> disease. In Kasper DL, Braunwald EB, Fauci AS,<br />
Hauser SL, Longo DL, and Jameson JL eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th<br />
ed. New York, NY: McGraw-Hill; 2005:26-28.<br />
214
#10 COORDINATION OF CARE<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
The task <strong>of</strong> coordinating a patient’s care is central to the role <strong>of</strong> the internist, and involves<br />
communication with the patient and his or her family, colleagues, consultants, nurses, social workers,<br />
and community-based agencies. It is essential for the student to learn that the physician’s<br />
responsibility toward the patient does not stop at the end <strong>of</strong> the <strong>of</strong>fice visit or hospitalization but<br />
continues in collaboration with other pr<strong>of</strong>essionals to ensure that the patient receives optimal care.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-clinical experience should<br />
include:<br />
Ability to perform patient-centered interviewing to determine the patients’ needs and<br />
communicate about diagnostic and therapeutic plans, transitions <strong>of</strong> care, and end-<strong>of</strong>-life care.<br />
Ability to identify community resources for care and strategies for coordination <strong>of</strong> care.<br />
Health Information Portability and Accountability Act (HIPAA) training to promote patient<br />
privacy.<br />
Required introductory courses in interviewing/physical examination with emphasis on doctorpatient<br />
communication and health care delivery.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe and discuss:<br />
1. The role <strong>of</strong> consultants and their limits in the care <strong>of</strong> a patient. (MK, SBP)<br />
2. Key personnel and programs in and out <strong>of</strong> the hospital that may be able to contribute to the<br />
ongoing care <strong>of</strong> an individual patient for whom the student has responsibility (e.g. home health<br />
providers, social workers, case coordinators/managers, community health organizations, etc.).<br />
(MK, SBP)<br />
3. The role <strong>of</strong> the primary care physician in coordinating the comprehensive and longitudinal<br />
patient care plan, including communicating with the patient and family (directly, telephone, or<br />
email) and evaluating patient well-being through home health and other care providers. (MK,<br />
SBP)<br />
4. HIPAA guidelines to promote patient privacy. (MK, SBP)<br />
5. The role <strong>of</strong> the primary care physician in the coordination <strong>of</strong> care during key transitions<br />
(e.g. outpatient to inpatient, inpatient to skilled nursing facility, inpatient to hospice, etc.). (MK,<br />
SBP)<br />
6. The role <strong>of</strong> clinical nurse specialists, nurse practitioners, physicians assistants, and other<br />
allied health pr<strong>of</strong>essionals in co-managing patients in the outpatient and inpatient setting. (MK,<br />
SBP)<br />
7. The importance <strong>of</strong> reconciliation <strong>of</strong> medications at all transition points <strong>of</strong> patient care. (MK,<br />
SBP)<br />
8. The rationale for a standardized approach to all “hand <strong>of</strong>f” communications (MK, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Discussing with the patient and their family ongoing health care needs; using appropriate<br />
language, avoiding jargon, and medical terminology. (PC, CS)<br />
215
2. Participating in requesting a consultation and identifying the specific question to be<br />
addressed. (PC, CS, .SBP)<br />
3. Participating in the discussion <strong>of</strong> the consultant’s recommendations. (PC, CS, SBP)<br />
4. Participating in developing a coordinated, ongoing care plan in the community. (PC, SBP)<br />
5. Obtaining a social history that identifies potential limitations in the home setting which may<br />
require an alteration in the medical care plan to protect the patient’s welfare. (PC, CS)<br />
6. Reconciling patient medications at key transition points in care. (PC, SBP)<br />
7. Conveying accurately vital patient information at all care “hand-<strong>of</strong>f” points (PC, CS, SBP)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate teamwork and respect toward all members <strong>of</strong> the health care team. (P, SBP)<br />
2. Demonstrate responsibility for patients’ overall welfare. (P)<br />
3. Participate, whenever possible, in coordination <strong>of</strong> care and in the provision <strong>of</strong> continuity. (P,<br />
SBP)<br />
D. REFERENCES:<br />
Goldman L, Lee, T, Rudd P. Ten commandments <strong>of</strong> effective consultation. Arch Intern Med.<br />
1983;143:1753-5.<br />
Stille CJ, Jerant A, Bell D, Meltzer D, Elmore JG. Coordinating care across diseases, settings,<br />
and clinicians: a key role for the generalist in practice. Ann Intern Med. 2005;142:700-708.<br />
Haggerty JL, Reid RJ, Freeman GK, Starfield BH, Adair CE, McKendry R. Continuity <strong>of</strong> care:<br />
a multidisciplinary review. BMJ. 2003;327:1219-21.<br />
Wenger NS, Young R. Quality indicators <strong>of</strong> continuity and coordination <strong>of</strong> care for vulnerable<br />
elder persons. Rand Corporation, 2004.<br />
www.rand.org/pubs/working_papers/2004/RAND_WR176.pdf<br />
Building a Case for Medication Reconciliation Institute for Safe Medication Practices<br />
www.ismp.org/Newsletters/acutecare/articles/20050421.asp<br />
Reconcile Medications at All Transition Points Institute for Healthcare Improvement<br />
www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/Changes/Reco<br />
ncile+Medications+at+All+Transition+Points.htm<br />
Healthcare Communications Toolkit to Improve Transitions <strong>of</strong> Care <strong>Department</strong> <strong>of</strong> Defense<br />
Patient Safety Program<br />
https://patientsafety.satx.disa.mil/ ContentStore/2005_12-<br />
8%20Hand<strong>of</strong>f%20Toolkit%20FINAL.htm<br />
216
GENERAL CLINICAL CORE COMPETENCIES<br />
#11 GERIATRIC CARE<br />
RATIONALE:<br />
Geriatric patients <strong>of</strong>ten have multiple, chronic illnesses which may present with atypical symptoms.<br />
Management strategies need to take into account the effects <strong>of</strong> aging on multiple organ systems and<br />
socioeconomic factors faced by our elderly society. As the number <strong>of</strong> geriatrics patients steadily<br />
rises, the internist will devote more time to the care <strong>of</strong> these patients.<br />
PREREQUISITES:<br />
Required courses in anatomy, physiology, pathophysiology, physical examination, and nutrition<br />
with attention to specific considerations in the elderly.<br />
Ability to perform a complete medical history and physical.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Functional implications <strong>of</strong> aging on each major organ system. (MK)<br />
2. Nutritional needs <strong>of</strong> the elderly and adaptations needed in the presence <strong>of</strong> chronic illness.<br />
(MK)<br />
3. Key illnesses in the elderly, focusing on their <strong>of</strong>ten atypical presentation, including:<br />
Cardiovascular and cerebrovascular disease. (MK)<br />
Diabetes. (MK)<br />
Urinary tract infection. (MK)<br />
Pneumonia. (MK)<br />
Substance abuse. (MK)<br />
Depression. (MK)<br />
Thyroid disease. (MK)<br />
Fluid and electrolyte disturbances. (MK)<br />
Arthritis. (MK)<br />
Constipation. (MK)<br />
Acute abdomen. (MK)<br />
Depression. (MK)<br />
4. The common “geriatric syndromes” (i.e. symptoms and conditions common in the elderly and<br />
<strong>of</strong>ten multifactorial in origin), including:<br />
Immobility. (MK)<br />
Falls/gait and balance problems. ( MK)<br />
Dizziness. (MK)<br />
Incontinence. (MK)<br />
Weight loss/failure to thrive/malnutrition. (MK)<br />
Sleep disturbance. (MK)<br />
Dementia/delirium. (MK)<br />
Osteoporosis. (MK)<br />
Hearing and visual impairment. (MK)<br />
Pressure ulcers. (MK)<br />
217
5. Basic treatment plans for illness in the elderly, with an awareness <strong>of</strong> the pharmacokinetic and<br />
pharmacodynamic changes seen as we age. (MK)<br />
6. Principles <strong>of</strong> screening in the elderly, including immunizations, cardiovascular risk, cancer,<br />
substance abuse, mental illness, osteoporosis, and functional assessment. (MK)<br />
7. Factors that contribute to polypharmacy in the elderly. (MK)<br />
8. Principles <strong>of</strong> Medicare (including who and what services are covered) and prescription drug<br />
coverage (who and what drugs are covered). (MK, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Taking a complete and focused history from a geriatric patient with attention to current<br />
symptoms, chronic illnesses, and physical and mental functioning (PC, CS)<br />
2. Always obtaining historical information from collateral source, whenever possible. (PC, CS)<br />
3. Performing a physical examination and functional assessment on an elderly patient, adapting it<br />
to a patient's symptoms, chronic illness, and possible conditions <strong>of</strong> frailty, immobility, hearing<br />
loss, memory loss, and other impairments. (PC)<br />
4. Performing a mental status examination to evaluate confusion and/or memory loss in an<br />
elderly patient. (PC)<br />
5. Identifying patients at high risk for falling. (PC)<br />
6. Developing a diagnostic and management plan for patients with the with symptoms/conditions<br />
common in the geriatric population. (PC, MK)<br />
7. Communicating the diagnosis, treatment plan, and subsequent follow-up to the patient and<br />
their family. (PC, CS)<br />
8. Eliciting input and questions from the patient and their family about the diagnostic and<br />
management plan. (PC, CS)<br />
9. With guidance and direct supervision, participating in discussing basic issues regarding<br />
advance directives with patients and their families. (CS)<br />
10. With guidance and direct supervision participating in discussing basic end-<strong>of</strong>-life issues with<br />
patients and their families. (CS)<br />
11. Actively attempting to limit polypharmacy whenever possible. (PC)<br />
12. Participating in an interdisciplinary approach to management and rehabilitation <strong>of</strong> elderly<br />
patients. (PC, SBP)<br />
13. Determine when to obtain consultation from a geriatric specialist. (PC, SBP)<br />
14. Accessing and using appropriate information systems and resources to help delineate issues<br />
related to the common geriatric syndromes. (PC, PLI)<br />
15. Incorporating patient needs and preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Respect the increased risk for iatrogenic complications among elderly patients by always<br />
taking into account risks and monitoring closely for complications (P)<br />
2. Demonstrate respect to older patients, particularly those with disabilities, by making efforts to<br />
preserve their dignity and modesty. (P)<br />
3. Always treat cognitively impaired patients and patients at the end <strong>of</strong> their lives with utmost<br />
respect and dignity. (P)<br />
4. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for the common<br />
geriatric syndromes. (PLI, P)<br />
5. Recognize the importance <strong>of</strong> patient needs and preferences when selecting among diagnostic<br />
and therapeutic options for the common geriatric syndromes. (P)<br />
218
6. Demonstrate ongoing commitment to self-directed learning regarding care <strong>of</strong> the geriatric<br />
patient. (P, PLI)<br />
7. Appreciate the impact the common geriatric syndromes have on a patient’s quality <strong>of</strong> life, wellbeing,<br />
and the family. (P)<br />
8. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other health<br />
care pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> geriatric patients. (P, SBP)<br />
D. REFERENCES:<br />
The American Geriatrics Society<br />
www.americangeriatrics.org/<br />
Guidelines and Position Statements<br />
www.americangeriatrics.org/products/positionpapers/<br />
Portal <strong>of</strong> Geriatric Online Education (POGOe)<br />
In association with AAMC MedEdPORTAL<br />
www.pogoe.org<br />
Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med.<br />
2003;348(1):42-9.<br />
Fuller GF. Falls in the elderly. Am Fam Physician. 2000;61:2159-68, 2173-4<br />
Miller KE, Zylstra RG, Standridge JB. The geriatric patient: a systematic approach to<br />
maintaining health. Am Fam Physician. 2000;61:1089-104.<br />
Willlams CM. Using medications appropriately in older adults. Am Fam Physician.<br />
2002;66:1917-24.<br />
Huffman GB. Evaluating and treating unintentional weight loss in the elderly. Am Fam<br />
Physician. 2002;65:640-50.<br />
Sloane PD, Coeytaux RR, Beck RS, Dallara J. Dizziness: state <strong>of</strong> the science. Ann Intern<br />
Med. 2001;134:823-32.<br />
Cummings JL. Alzheimer's disease. N Engl J Med. 2004;351:56-67.<br />
Lembo A, Camilleri M. Chronic constipation. N Engl J Med. 2003;349:1360-8.<br />
Resnick NM, Dosa D. Geriatric medicine. In Kasper DL, Braunwald EB, Fauci AS, Hauser SL,<br />
Longo DL, Jameson JL eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th ed. New York,<br />
NY: McGraw-Hill; 2005:43-53.<br />
219
#12 BASIC PROCEDURES<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
For many students, the internal medicine <strong>clerkship</strong> is where the basic procedural skills required in<br />
other <strong>clerkship</strong>s, subinternships, and residencies are learned.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Pertinent anatomic considerations, including venous anatomy <strong>of</strong> the extremities (for<br />
venipuncture and IV placement), arterial anatomy <strong>of</strong> the wrist and groin (for blood gases),<br />
vaginal/vulvar anatomy (for urethral catheterization in women as well as pap smear) and<br />
prostate anatomy in men (for prostate exam), rectal anatomy (for digital rectal exam) and<br />
surface anatomy and electrical vector orientation <strong>of</strong> the heart (for EKG placement).<br />
The fundamental tenants <strong>of</strong> informed consent.<br />
Basic training in body substance isolation procedures and sterile technique.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Key indications, contraindications, risks to patients and health care providers, benefits, and<br />
techniques for each <strong>of</strong> the following basic procedures:<br />
Venipuncture. (MK)<br />
Blood culture. (MK)<br />
ABG. (MK)<br />
ECG. (MK)<br />
Chest radiography. (MK)<br />
Nasogastric tube placement. (MK)<br />
Urethral catheterization. (MK)<br />
Peripheral intravenous catheter insertion. (MK)<br />
Throat culture. (MK)<br />
PAP smear. (MK)<br />
Digital rectal examination. (MK)<br />
Urine dipstick. (MK)<br />
Stool occult blood testing. (MK)<br />
Subcutaneous injection. (MK)<br />
Intramuscular injection. (MK)<br />
Wound culture. (MK)<br />
Dressing change. (MK)<br />
PPD placement. (MK)<br />
2. Alternatives to a given procedure. (MK)<br />
3. The patient’s experience <strong>of</strong> the procedure. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
220
1. Obtaining informed consent, when necessary, for basic procedures, including the explanation<br />
<strong>of</strong> the purpose, possible complications, alternative approaches, and conditions necessary to<br />
make the procedure as comfortable, safe, and interpretable as possible. (PC, CS)<br />
2. Explaining what the patient’s experience is likely to be in understandable terms. (CS)<br />
3. Demonstrating step-by-step performance <strong>of</strong> basic procedures with technical pr<strong>of</strong>iciency. (PC)<br />
4. Demonstrating proper sterile technique and body substance isolation procedures. (PC)<br />
5. Appropriately documenting, when required, how the procedure was done, any complications,<br />
and results. (CS)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Appreciate the fear and anxiety many patients have regarding even simple procedures. (P)<br />
2. Make efforts to maximize patient comfort during a procedure. (P)<br />
3. Appreciate the patient’s right to refuse procedures. (P)<br />
4. Regularly seek feedback regarding procedural skills and respond appropriately and<br />
productively. (P)<br />
D. REFERENCES:<br />
Guide to procedures. In Lin GA, Lin TL, Sakurai KA, De Fer TM, eds. The Washington Manual<br />
Internship Survival Guide. 2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2005:178-<br />
210.<br />
Chen H, Sonneday CJ, Lillemoe KD eds. Manual <strong>of</strong> Common Bedside Surgical Procedures.<br />
2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2000.<br />
Ferri FF. Procedures and interpretation <strong>of</strong> results. In Ferri FF, ed. Practical Guide to the Care<br />
<strong>of</strong> the Medical Patient. 6th ed. St. Louis, MO: Mosby; 2004:903-934.<br />
221
GENERAL CLINICAL CORE COMPETENCIES<br />
#13 NUTRITION<br />
RATIONALE:<br />
Despite the importance <strong>of</strong> nutritional factors in health and illness, physicians frequently have been<br />
criticized for giving these factors inadequate attention. Internists, by virtue <strong>of</strong> their dedication to<br />
providing comprehensive care to their patients, must assess nutritional factors on a routine basis.<br />
Medical students should be prepared to provide patients with basic advice regarding ways to optimize<br />
their nutritional status. Students also need to have at least a basic working knowledge <strong>of</strong> the<br />
principles <strong>of</strong> nutritional assessment and intervention.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Ability to perform a complete medical history.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
Knowledge <strong>of</strong> body metabolism, the respective roles <strong>of</strong> dietary fats, carbohydrates, and<br />
protein, and the need for vitamins and minerals for maintenance <strong>of</strong> health.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Each student should be able to define, describe, and discuss:<br />
1. The relationship between diet and disease. (MK)<br />
2. Common medical problems that can cause nutritional deficiencies. (MK)<br />
3. Contributions <strong>of</strong> nutrition to medical problems such as obesity,<br />
hyperlipidemia, diabetes, and hypertension. (MK)<br />
4. How to perform a nutritional assessment and assist the patient in setting goals for dietary<br />
improvement. (MK)<br />
5. Daily caloric, fat, carbohydrate, protein, mineral, and vitamin requirements; adequacy <strong>of</strong> diets<br />
in providing such requirements; evidence <strong>of</strong> need for and potential risks <strong>of</strong> supplements (e.g.<br />
calcium, antioxidants). (MK)<br />
6. Common dietary supplements and their known adverse and beneficial effects on health. (MK)<br />
7. The consequences <strong>of</strong> poor nutrition on a critically ill patient, such as poor wound healing,<br />
increased risk <strong>of</strong> infection, and increased mortality. (MK)<br />
8. Nutritional needs <strong>of</strong> the elderly and adaptations needed in the presence <strong>of</strong> chronic illness.<br />
(MK)<br />
9. The indications for enteral and parenteral nutrition. (MK)<br />
B. SKILLS: Student should be able to demonstrate specific skills, including:<br />
1. Obtaining a nutritional history for all patients, with additional focus on those with chronic<br />
disease (obesity, hyperlipidemia, diabetes mellitus, hypertension, alcoholism, cancer, COPD,<br />
CHF, renal, and GI disease), giving attention to weight change, appetite, eating habits,<br />
digestive problems, dental problems, physical handicaps, psychiatric problems, socioeconomic<br />
factors, alcohol use, medications, and physical activity. (PC, CS)<br />
2. Identifying physical exam abnormalities that may suggest malnutrition, such as muscle<br />
wasting, decreased adipose stores, as well as stigmata <strong>of</strong> vitamin/mineral or protein-calorie<br />
222
malnutrition (e.g. alopecia, ecchymoses, angular chelosis, glossitis, peripheral neuropathy,<br />
edema, etc.). (PC)<br />
3. Calculating a patient’s body mass index (BMI) and measuring waist circumference. (PC)<br />
4. Ordering appropriate tests for evaluating a patient’s nutritional status, including albumin,<br />
prealbumin, serum chemistries and coagulation pr<strong>of</strong>ile(PC)<br />
5. Performing basic nutritional counseling with patients with obesity, diabetes mellitus,<br />
hyperlipidemia, hypertension, heart failure, and coronary artery disease. (PC, CS)<br />
6. Identifying barriers that prevent a patient from successfully adhering to a recommended diet.<br />
(PC, CS)<br />
7. Determining when to obtain consultation from a dietician. (PC, SBP)<br />
8. Incorporating patient needs and preferences. (PC, P)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for malnutrition. (PLI,<br />
P)<br />
2. Recognize the importance <strong>of</strong> patient preferences and cultural factors when selecting nutritional<br />
counseling. (PLI, P)<br />
3. Respond to patients who are non-adherent to recommendations for appropriate nutritional<br />
intake. (CS, P)<br />
4. Demonstrate ongoing commitment to self-directed learning regarding nutrition. (PLI, P)<br />
5. Appreciate the impact malnutrition has on a patient’s quality <strong>of</strong> life, wellbeing, ability to work,<br />
and the family. (P)<br />
6. Recognize the importance <strong>of</strong> involving other healthcare pr<strong>of</strong>essionals when appropriate. (P,<br />
SBP)<br />
D. REFERENCES:<br />
Division <strong>of</strong> Nutrition and Physical Activity National Center for Chronic Disease Prevention and<br />
Health Promotion<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Serviced<br />
www.cdc.gov/nccdphp/dnpa/<br />
Dietary Guidelines for Americans<br />
U.S. <strong>Department</strong> <strong>of</strong> Agriculture<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.health.gov/dietaryguidelines/<br />
American Dietetic Association<br />
www.eatrigh.org<br />
Food and Nutrition Information Center<br />
U.S. <strong>Department</strong> <strong>of</strong> Agriculture<br />
www.nal.usda.gov/fnic/<br />
Dwyer J. Nutritional requirements and dietary assessment. In Kasper DL, Braunwald EB,<br />
Fauci AS, Hauser SL, Longo DL, Jameson JL eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>.<br />
16th ed. New York, NY: McGraw-Hill; 2005:399-403.<br />
Halsted CH. Malnutrition and nutritional assessment. In Kasper DL, Braunwald EB, Fauci AS,<br />
Hauser SL, Longo DL, Jameson JL eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th ed.<br />
New York, NY: McGraw-Hill; 2005:411-415.<br />
Howard L. Enteral and parenteral nutrition therapy. In Kasper DL, Braunwald EB, Fauci AS,<br />
223
Hauser SL, Longo DL, Jameson JL eds. Harrison’s Principles <strong>of</strong> Internal <strong>Medicine</strong>. 16th ed.<br />
New York, NY: McGraw-Hill; 2005:415-422.<br />
224
#14 COMMUNITY HEALTH CARE<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
The increasing number <strong>of</strong> physicians practicing under managed care and in community-oriented<br />
primary care practices necessitates expanding medical education to prepare graduates for<br />
population-based clinical practice. In a managed care setting, population-based clinical practice<br />
includes the health <strong>of</strong> an enrolled population. In a community-based setting, population-based clinical<br />
practice includes the health <strong>of</strong> a population in addition to the health <strong>of</strong> the individual patient through<br />
concern with resource allocation, epidemiology, and the care <strong>of</strong> patients whose needs are not<br />
currently met by the health care system.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should<br />
include:<br />
Required introductory coursework in health care delivery (with an emphasis on medical<br />
sociology and health care delivery to at risk populations).<br />
Required introductory course in clinical epidemiology and biostatistics.<br />
Required introductory coursework in population health (with an emphasis on differences<br />
between individuals and populations).<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The concepts <strong>of</strong> rate, incidence, and prevalence to characterize the health <strong>of</strong> a population.<br />
(MK)<br />
2. How to gather health information about a population. (MK)<br />
3. How disease epidemiology in a community differs from that experienced in an <strong>of</strong>fice or hospital<br />
practice. (MK)<br />
4. How health care financing and health care delivery systems affect individual physicians,<br />
patients, and communities. (MK, SBP)<br />
5. How community and individual responses to health problems may be affected by both<br />
individual and community socio-cultural characteristics. (MK)<br />
6. Local government, social service, or community organizations that provide links between the<br />
underserved members <strong>of</strong> the community and the medical care systems. (MK, SBP)<br />
7. barriers faced by his or her patients in the community setting. (MK)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Defining and describing a population, its demography, culture, socioeconomic makeup, and<br />
health status. (PC)<br />
2. Identifying the unique characteristics <strong>of</strong> a population that affect the health <strong>of</strong> the population and<br />
individuals within that population. (PC)<br />
3. Considering how the socio-cultural characteristics <strong>of</strong> a particular community may affect that<br />
population’s attitudes toward health care. (PC)<br />
4. Using, in daily patient care, an understanding <strong>of</strong> the community and sociocultural context that<br />
may affect an individual patient’s health care decisions and health-related behaviors. (PC)<br />
225
5. Identifying patients whose illnesses may put the community at risk. (PC, MK)<br />
6. Incorporating a population-based perspective in analyzing clinical problems (PC)<br />
7. Reading critically clinical studies and applying findings to health care decisions involving real<br />
patients and populations <strong>of</strong> patients. (PC, MK, PLI)<br />
8. Incorporating principles <strong>of</strong> disease prevention and behavioral change appropriate for specific<br />
populations <strong>of</strong> patients within a community. (PC, MK)<br />
9. Attempting to develop solutions for barriers to health care delivery (e.g. sociocultural, financial,<br />
and system-based) that affect individual patients. (PC, SBP)<br />
10. Functioning effectively as a member <strong>of</strong> a health care team. (PC, P, SBP)<br />
11. Using, when appropriate, local government, social service, and community organizations to<br />
improve the health <strong>of</strong> individuals and populations. (PC, SBP)<br />
12. Accessing and utilizing appropriate information systems and resources to help delineate issues<br />
related to population health. (PC, PLI)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate respect for cultural and socioeconomic diversity. (P)<br />
2. Show willingness to accept at least partial responsibility for the health <strong>of</strong> populations. (P)<br />
3. Respond non-judgmentally to an individual whose socio-cultural and community-based<br />
background result in seemingly counterproductive heath care decisions and health-related<br />
behaviors. (P)<br />
4. Value the unique contributions <strong>of</strong> all members <strong>of</strong> the health care team. (P)<br />
5. Demonstrate ongoing commitment to self-directed learning regarding population/community<br />
health issues. (PLI, P)<br />
D. REFERENCES:<br />
Contemporary Issues in Medical Education: Quality <strong>of</strong> Care<br />
Medical Informatics and Population Health, June, 1998<br />
American Association <strong>of</strong> Medical Colleges<br />
www.aamc.org/meded/msop/msop2.pdf<br />
Population Health Forum<br />
<strong>University</strong> <strong>of</strong> Washington<br />
School <strong>of</strong> Public Health and Community <strong>Medicine</strong><br />
depts.washington.edu/eqhlth/index.htm<br />
Behavioral Risk Factor Surveillance System Division <strong>of</strong> Adult and Community Health National<br />
Center for Chronic Disease Prevention and Health Promotion Centers for Disease Control and<br />
Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/brfss/index.htm<br />
Healthy People 2010 National Center for Health Statistics<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/nchs/hphome.htm<br />
Rhyne RL, Bogue R, Kukulka G, Fulmer H, eds. Community-Oriented Primary Care: Health<br />
Care for the 21st Century. Washington, DC: American Public Health Association; 1998.<br />
Strelnick AH. Community-oriented primary care: the state <strong>of</strong> an art. Arch Fam Med.<br />
1999;8:550-2.<br />
Fox DM. The relevance <strong>of</strong> population health to academic medicine. Acad Med. 2001;76:6-7.<br />
Kindig D, Stoddart G. What is population health?. Am J Public Health. 2003;93:380-3.<br />
226
GENERAL CLINICAL CORE COMPETENCIES<br />
#15 CONTINUOUS IMPROVEMENT IN SYSTEMS OF MEDICAL PRACTICE<br />
RATIONALE:<br />
In the past clinical education had emphasized the role <strong>of</strong> the physician as an individual decision<br />
maker. Problems with cost and quality <strong>of</strong> care had usually been attributed to errors in individual<br />
decision making. In recent years, it has become clear that the individual does not function in isolation<br />
but within the context <strong>of</strong> a health care system and a health care team whose structure ranges from<br />
simple to complex. The way the system functions is critical to achieving high quality patient care,<br />
ensuring patient safety, reducing sources <strong>of</strong> errors in medicine, and promoting an environment that<br />
respects disclosure without blame. Furthermore, we have begun to focus on the patient as the center<br />
<strong>of</strong> the health care delivery system and to assess quality from the perspectives <strong>of</strong> the patient and the<br />
physician. With the patient as the center <strong>of</strong> the health care delivery system, the physician becomes a<br />
collaborative partner with other health pr<strong>of</strong>essionals who share a common goal <strong>of</strong> providing safe,<br />
accessible, high quality, evidence-based care.<br />
PREREQUISITES:<br />
Prior knowledge, skills and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Required introductory course in clinical epidemiology and biostatistics.<br />
Required introductory course in health care delivery.<br />
Required introductory course in bioethics and pr<strong>of</strong>essionalism.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. The concept <strong>of</strong> systems-based practice. (MK, SBP)<br />
2. How patient care is affected by other pr<strong>of</strong>essionals, organizations, and society. (MK, SBP)<br />
3. The principles <strong>of</strong> clinical quality improvement, including the notion <strong>of</strong> variation in practice as a<br />
quality issue and the concept <strong>of</strong> medical care as a process which can be studied and<br />
improved. (MK, SBP)<br />
4. The analysis and improvement <strong>of</strong> systems to address common quality problems (e.g.,<br />
treatment delays, medication errors, failure to use evidence-based diagnostics/treatments,<br />
failure to provide preventive care, etc.). (MK, SBP)<br />
5. Principles <strong>of</strong> medical record organization in both inpatient and ambulatory settings. (MK, SBP)<br />
6. The importance <strong>of</strong> complete medical documentation in the context <strong>of</strong> measuring quality <strong>of</strong><br />
care, avoiding redundancy, preventing medical errors, and improving patient safety. (MK, SBP)<br />
7. The need for a multidimensional approach to the assessment <strong>of</strong> quality, including the patient’s<br />
perspective <strong>of</strong> quality. (MK, SBP)<br />
8. The relationship <strong>of</strong> quality and cost in health care from the standpoint <strong>of</strong> the individual, health<br />
care systems, and society. (MK, SBP)<br />
9. Major health care safety concerns (e.g., medication errors, wrong-site procedures, patient<br />
misidentification, miscommunication among health care givers, nosocomial infections, falls,<br />
use <strong>of</strong> restraints, etc.). (MK, SBP)<br />
10. Potential benefits and pitfalls <strong>of</strong> critical pathways/practice guidelines intended to improve the<br />
quality <strong>of</strong> care. (MK, SBP)<br />
11. Basic organizational structures and financing streams <strong>of</strong> the U.S. health care system. (MK,<br />
SBP)<br />
227
12. The fundamentals <strong>of</strong> the various type <strong>of</strong> health insurance (e.g., fee-for-service, preferred<br />
provider organization, health maintenance organization, point-<strong>of</strong>service). (MK, SBP)<br />
13. The fundamentals <strong>of</strong> Medicare and Medicaid. (MK, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Using hospital-based support systems to assist in making clinical decisions (e.g., antibiotic<br />
control program, critical pathways/practice guidelines, etc.). (PC, PLI, SBP)<br />
2. Recognizing system flaws in the delivery <strong>of</strong> care (e.g., inability to arrange a post-discharge<br />
appointment within a needed time frame, delays in obtaining test results, inaccessibility <strong>of</strong><br />
medical records, etc.). (SBP)<br />
3. Using patient education materials to facilitate patients’ participation in their own care. (CS,<br />
SBP)<br />
4. Using the medical records system efficiently to produce medical notes that communicate<br />
information clearly. (PC, CS, SBP)<br />
5. Maintaining accurate documentation <strong>of</strong> preventive health measures. (PC, CS, SBP)<br />
6. Working collaboratively with other health pr<strong>of</strong>essionals in the delivery <strong>of</strong> quality care. (PC, P,<br />
SBP)<br />
7. Assessing the patients’ needs from the standpoint <strong>of</strong> the individual, family, and community.<br />
(PC, SBP)<br />
8. Identifying resource available to patients within the health care system. (PC, SBP)<br />
9. Reporting patient safety concerns and medical errors to the appropriate individuals. (CS, SBP)<br />
10. Using resources, appropriate information systems, and the tenants <strong>of</strong> evidence-based<br />
medicine to assess systems-based practice issues. (PLI, SBP)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Recognize the importance <strong>of</strong> systems, particularly inter-pr<strong>of</strong>essional collaboration, in delivering<br />
high quality patient care. (P, SBP)<br />
2. Strive to improve the timeliness diagnostic and therapeutic decision making in order to improve<br />
quality <strong>of</strong> care, increase patient satisfaction, and reduce health care costs. (PLI, P, SBP)<br />
3. View the patient as the center <strong>of</strong> the health care delivery system. (P, SBP)<br />
4. Advocate for patients in the health care system. (P, SBP)<br />
5. Appreciate that medical error prevention and patient safety are the responsibility <strong>of</strong> all health<br />
care providers and systems and accept the appropriate degree <strong>of</strong> responsibility at the medical<br />
student level. (P, SBP)<br />
6. Appreciate the importance teamwork in delivering high quality care. (P, SBP)<br />
7. Respect other health care pr<strong>of</strong>essionals as colleagues on a patient-centered health delivery<br />
team and as mutual contributors to high quality patient care. (P, SBP)<br />
D. REFERENCES:<br />
GENERAL:<br />
Agency for Healthcare Research and Quality<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
ahrq.gov<br />
QUALITY OF CARE:<br />
Institute for Healthcare Improvement<br />
228
www.ihi.org/ihi<br />
Crossing the Quality Chasm: A New Health System for the 21st Century<br />
Committee on Quality Health Care in America<br />
Institute <strong>of</strong> <strong>Medicine</strong><br />
National Academies Press, 2001<br />
National Committee for Quality Assurance<br />
www.ncqa.org<br />
National Guideline Clearing House<br />
Agency for Healthcare Research and Quality<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.guideline.gov<br />
MEDIAL ERRORS AND PATIENT SAFETY:<br />
To Err Is Human: Building a Safer Health System<br />
Institute <strong>of</strong> <strong>Medicine</strong><br />
www.iom.edu/?id=4117&redirect=0<br />
Patient Safety Network<br />
Agency for Healthcare Research and Quality<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
psnet.ahrq.gov<br />
National Patient Safety Foundation<br />
www.npsf.org<br />
Facts About Patient Safety<br />
Joint Commission on Accreditation <strong>of</strong> Healthcare Organizations<br />
www.jcaho.org/accredited+organizations/patient+safety/facts+about+pati<br />
ent+safety.htm<br />
HEALTH INSURANCE AND FINANCE:<br />
Understanding Managed Care<br />
Institute for Health Care Studies<br />
Michigan State <strong>University</strong><br />
www.ihcs.msu.edu/modules/UMC2003/UMC2003.pdf<br />
The Official U.S. Government Site for People with Medicare<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.medicare.gov<br />
Checkup on Health Insurance Choices<br />
Agency for Healthcare Research and Quality<br />
www.ahrq.gov/consumer/insuranc.htm<br />
229
#16 OCCUPATIONAL HEALTH CARE<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
Despite increasing recognition <strong>of</strong> the health hazards found in living and working environments,<br />
physicians have traditionally received little formal training in the assessment and management <strong>of</strong><br />
occupational and environmental health problems.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should<br />
include:<br />
Required introductory course work in clinical epidemiology and biostatistics.<br />
Required introductory course work in the fundamental principles <strong>of</strong> public health.<br />
Ability to perform a complete medical history and physical exam.<br />
Ability to communicate with patients <strong>of</strong> diverse backgrounds.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Each student should be able to define, describe, and discuss :<br />
1. Common environmental diseases that are likely to be encountered by an internist and the<br />
principal etiologic agents associated with them. (MK)<br />
2. Pathogenesis <strong>of</strong> specific occupational diseases and the types <strong>of</strong> risks that may be encountered<br />
in the home or at the work site:<br />
Musculoskeletal/ergonomic or “repetitive stress” disorders (e.g. low back pain, carpal<br />
tunnel syndrome, etc.). (MK)<br />
Work related lung disorders (e.g. occupational asthma, particulate inhalation, etc.). (MK)<br />
Noise related hearing loss. (MK)<br />
Skin disorders (e.g. latex allergy and other forms <strong>of</strong> occupational dermatitis). (MK)<br />
Infectious disease exposure (e.g. hepatitis, HIV, TB, etc.). (MK)<br />
Psychological/stress related disorders (MK)<br />
3. Information sources for determining the risk <strong>of</strong> specific environmental and occupational health<br />
hazards. (MK)<br />
4. Purpose <strong>of</strong> Occupational Safety and Health Act (OSHA) regulations and the function <strong>of</strong> the<br />
National Institute for Occupational Safety and Health. (NIOSH). (MK, SBP)<br />
B. SKILLS: Students should be able to demonstrate specific skills, including:<br />
1. Obtaining an appropriate occupational history on all patients and identifying those patients<br />
whose health may have been adversely affected by their living conditions or work environment.<br />
(PC, CS)<br />
2. Considering the possibility that the patient’s illness may be related to their home or work<br />
environment. (PC)<br />
3. Providing patients with sound advice on the prevention <strong>of</strong> occupational and environmentalrelated<br />
diseases. (PC, CS)<br />
4. Accurately diagnosing and developing a cost-effective basic management plan for common<br />
occupational health problems (e.g. carpal tunnel syndrome, asthma, asbestosis). (PC, MK,<br />
SBP)<br />
230
5. Determining when to obtain consultation from an environmental and occupational medicine<br />
specialist. (PC, SBP)<br />
6. Accessing and utilizing appropriate information systems and resources to help delineate issues<br />
related to occupational health problems. (PC, PLI)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIORS: Students should be able to:<br />
1. Demonstrate an understanding that physicians have a duty and pr<strong>of</strong>essional responsibility to<br />
follow-up on conditions that are suspected <strong>of</strong> causing occupational or environmental-related<br />
illnesses. (P, SBP)<br />
2. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> diagnostic and therapeutic interventions for occupational<br />
health problems. (PLI, P)<br />
3. Recognize the importance <strong>of</strong> patient needs and preferences when selecting among diagnostic<br />
and therapeutic options for occupational health problems. (P)<br />
4. Demonstrate ongoing commitment to self-directed learning regarding occupational health<br />
problems. (PLI, P)<br />
5. Appreciate the impact occupational health problems have on a patient’s quality <strong>of</strong> life, wellbeing,<br />
ability to work, and the family. (P)<br />
6. Recognize the importance <strong>of</strong> and demonstrate a commitment to the utilization <strong>of</strong> other health<br />
care pr<strong>of</strong>essionals in the diagnosis and treatment <strong>of</strong> occupational health problems. (P, SBP)<br />
D. REFERENCES:<br />
Occupational Safety and Health Administration<br />
U.S. <strong>Department</strong> <strong>of</strong> Labor<br />
www.osha.gov<br />
National Institute for Occupational Safety and Health<br />
Centers for Disease Control and Prevention<br />
U.S. <strong>Department</strong> <strong>of</strong> Health and Human Services<br />
www.cdc.gov/niosh/homepage.html<br />
231
#17 ADVANCED PROCEDURES<br />
GENERAL CLINICAL CORE COMPETENCIES<br />
RATIONALE:<br />
A number <strong>of</strong> advanced procedures may be performed by general internists, and occasionally thirdyear<br />
medical students under their supervision. In either case, knowledge <strong>of</strong> the key indications,<br />
contraindications, risks, and benefits <strong>of</strong> these procedures is essential for high quality patient care.<br />
Physicians, regardless <strong>of</strong> specialty, must be able to explain to their patients, in understandable terms,<br />
what will be experienced during a procedure.<br />
PREREQUISITES:<br />
Prior knowledge, skills, and attitudes acquired during the pre-<strong>clerkship</strong> experience should include:<br />
Pertinent anatomic considerations, including vascular anatomy <strong>of</strong> the extremities, wrist/hand,<br />
neck, subclavian area and groin.<br />
Pertinent anatomic landmarks important for the safe performance <strong>of</strong> thoracentesis,<br />
paracentesis, lumbar puncture, and arthrocentesis.<br />
Required introductory course in interviewing and physical examination.<br />
The fundamental tenants <strong>of</strong> informed consent.<br />
Basic training in body substance isolation procedures and sterile technique.<br />
SPECIFIC LEARNING OBJECTIVES:<br />
A. KNOWLEDGE: Students should be able to define, describe, and discuss:<br />
1. Key indications, contraindications, risks, benefits, techniques <strong>of</strong> each <strong>of</strong> the following advanced<br />
procedures:<br />
Arthrocentesis. (MK)<br />
o Elbow (olecranon bursa). (MK)<br />
o Wrist. (MK)<br />
o Knee. (MK)<br />
o Ankle. (MK)<br />
Central venous catheterization. (MK)<br />
o Internal jugular vein. (MK)<br />
o Subclavian vein. (MK)<br />
o Femoral vein. (MK)<br />
Arterial line placement. (MK)<br />
o Radial artery. (MK)<br />
o Femoral artery. (MK)<br />
Lumbar puncture. (MK)<br />
Thoracentesis. (MK)<br />
Paracentesis. (MK)<br />
2. Potential alternatives to the listed procedures. (MK)<br />
3. The patient’s probable experience during these procedures. (MK)<br />
4. Indications for and efficacy <strong>of</strong> intra-articular corticosteroid injections. (MK)<br />
B. SKILLS: Each student should be able to demonstrate specific skills, including:<br />
232
1. Participating in obtaining informed consent for advanced procedures, including the explanation<br />
<strong>of</strong> the purpose, possible complications, alternative approaches, and conditions necessary to<br />
make the procedure as comfortable, safe, and interpretable as possible. (PC, CS)<br />
2. Explaining the patient’s probable experience during the procedure in understandable terms.<br />
(PC, CS)<br />
3. Helping to position the patient and make them as comfortable as possible during the<br />
procedure. (PC)<br />
4. Assisting (under supervision, when appropriate) in the performance <strong>of</strong> the procedure. (PC)<br />
5. Demonstrating proper sterile technique and body substance isolation procedures. (PC)<br />
6. Appropriately documenting, when required, how the procedure was done as well as any<br />
complications and results. (CS)<br />
7. Ordering and interpreting appropriate diagnostic tests on fluids removed from the patient (e.g.<br />
synovial fluid, cerebrospinal fluid, pleural fluid, and ascitic fluid). (PC, MK)<br />
C. ATTITUDES AND PROFESSIONAL BEHAVIOR: Students should be able to:<br />
1. Demonstrate commitment to using risk-benefit, cost-benefit, and evidence-based<br />
considerations in the selection <strong>of</strong> procedures to be performed. (PLI, P)<br />
2. Appreciate the fear and anxiety many patients have regarding these procedures. (P)<br />
3. Make efforts to maximize patient comfort during a procedure. (P)<br />
4. Appreciate the patient’s right to refuse procedures. (P)<br />
5. Seek feedback regularly regarding procedural skills and respond appropriately and<br />
productively. (P)<br />
D. REFERENCES:<br />
Guide to procedures. In Lin GA, Lin TL, Sakurai KA, De Fer TM, eds. The Washington Manual<br />
Internship Survival Guide. 2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2005:178-<br />
210.<br />
Chen H, Sonneday CJ, Lillemoe KD eds. Manual <strong>of</strong> Common Bedside Surgical Procedures.<br />
2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2000.<br />
Ferri FF. Procedures and interpretation <strong>of</strong> results. In Ferri FF, ed. Practical Guide to the Care<br />
<strong>of</strong> the Medical Patient. 6th ed. St. Louis, MO: Mosby; 2004:903-934.<br />
233
LIST OF ERROR-PRONE ABBREVIATIONS, SYMBOLS, AND DOSE<br />
DESIGNATIONS<br />
234
November 27, 2003 Volume 8 Issue 24<br />
ISMP List <strong>of</strong> Error-Prone Abbreviations, Symbols, and<br />
Dose Designations<br />
It’s been over 2 years since we published a list <strong>of</strong> abbreviations, symbols, the organization’s list, we’ve highlighted these items with a<br />
double and dose designations that have contributed to medication errors. Now, asterisk (**). Also, effective April 1, 2004, each<br />
organization must include with the 2004 JCAHO National Patient Safety Goals calling for organiza-at least three additional items on<br />
their list. However, we hope that you tional compliance with a list <strong>of</strong> prohibited “dangerous” abbreviations, will consider others<br />
beyond the minimum JCAHO requirement. Selections acronyms and symbols, we thought an updated list would be useful. can be<br />
made from the attached list. These items should be considered Since JCAHO has specified that certain abbreviations must appear on<br />
for handwritten, preprinted, and electronic forms <strong>of</strong> communication.<br />
Abbreviations Intended Meaning Misinterpretation Correction<br />
µg Microgram Mistaken as “mg” Use “mcg”<br />
AD, AS, AU<br />
Right ear, left ear, each Mistaken as OD, OS, OU (right eye, left eye, each Use “right ear,” “left ear,” or<br />
ear<br />
eye)<br />
“each ear”<br />
OD, OS, OU<br />
Right eye, left eye, each Mistaken as AD, AS, AU (right ear, left ear, each Use “right eye,” “left eye,” or<br />
eye<br />
ear)<br />
“each eye”<br />
BT Bedtime Mistaken as “BID” (twice daily) Use “bedtime”<br />
cc Cubic centimeters Mistaken as “u” (units) Use “mL”<br />
D/C Discharge or<br />
discontinue<br />
Premature discontinuation <strong>of</strong> medications if D/C<br />
(intended to mean “discharge”) has been<br />
misinterpreted as “discontinued” when followed by<br />
a list <strong>of</strong> discharge medications<br />
235<br />
Use “discharge” and<br />
“discontinue”<br />
IJ Injection Mistaken as “IV” or “intrajugular” Use “injection”<br />
IN Intranasal Mistaken as “IM” or “IV” Use “intranasal” or “NAS”<br />
HS hs Half-strength At Mistaken as bedtime Mistaken as half-strength Use “half-strength” or “bedtime”<br />
bedtime, hours <strong>of</strong> sleep<br />
IU** International unit Mistaken as IV (intravenous) or 10 (ten) Use “units”<br />
o.d. or OD Once daily Mistaken as “right eye” (OD-oculus dexter), leading Use “daily”<br />
to oral liquid medications administered in the eye<br />
OJ Orange juice Mistaken as OD or OS (right or left eye); drugs Use "orange juice"<br />
meant to be diluted in orange juice may be given in<br />
the eye<br />
Per os By mouth, orally<br />
The “os” can be mistaken as “left eye” (OS-oculus Use “PO,” “by mouth,” or<br />
sinister)<br />
“orally”<br />
q.d. or QD** Every day Mistaken as q.i.d., especially if the period after the Use “daily”<br />
“q” or the tail <strong>of</strong> the “q” is misunderstood as an “i”<br />
qhs At bedtime Mistaken as “qhr” or every hour Use “at bedtime”<br />
qn Nightly Mistaken as “qh” (every hour) Use “nightly”<br />
q.o.d. or QOD** Every other day Mistaken as “q.d.” (daily) or “q.i.d. (four times Use “every other day”<br />
daily) if the “o” is poorly written<br />
q1d Daily Mistaken as q.i.d. (four times daily) Use “daily”<br />
q6PM, etc. Every evening at 6 PM Mistaken as every 6 hours<br />
Use “6 PM nightly” or “6 PM<br />
daily”<br />
SC, SQ, sub q Subcutaneous SC mistaken as SL (sublingual); SQ mistaken as “5<br />
every;” the “q” in “sub q” has been mistaken as<br />
Use “subcut” or<br />
“subcutaneously”<br />
“every” (e.g., a heparin dose ordered “sub q 2 hours<br />
before surgery” misunderstood as every 2 hours<br />
before surgery)<br />
ss Sliding scale (insulin) or<br />
½ (apothecary)<br />
Mistaken as “55”<br />
Spell out “sliding scale;” use<br />
“one-half” or “½”<br />
SSRI SSI<br />
Sliding scale regular<br />
insulin Sliding scale<br />
insulin<br />
Mistaken as selective-serotonin reuptake inhibitor<br />
Mistaken as Strong Solution <strong>of</strong> Iodine (Lugol's)<br />
Spell out “sliding scale (insulin)”<br />
i/d One daily Mistaken as “tid” Use “1 daily”<br />
TIW or tiw 3 times a week Mistaken as “3 times a day” or “twice in a week” Use “3 times weekly”
U or u** Unit Mistaken as the number 0 or 4, causing a 10-fold Use “unit”<br />
overdose or greater (e.g., 4U seen as “40” or 4u seen<br />
as “44”); mistaken as “cc” so dose given in volume<br />
instead <strong>of</strong> units (e.g., 4u seen as 4cc)<br />
Dose Designations<br />
and Other<br />
Information<br />
Intended Meaning Misinterpretation Correction<br />
Trailing zero<br />
after decimal<br />
point (e.g., 1.0<br />
mg)**<br />
No leading zero<br />
before a decimal<br />
dose (e.g., .5<br />
mg)**<br />
1 mg Mistaken as 10 mg if the decimal point is not seen<br />
0.5 mg Mistaken as 5 mg if the decimal point is not seen<br />
Do not use trailing zeros for<br />
doses expressed in whole<br />
numbers<br />
Use zero before a decimal point<br />
when the dose is less than a<br />
whole unit<br />
_ ISMP 2003<br />
ISMP MedicationSafetyAlert!<br />
November 27, 2003 Volume 8 Issue 24<br />
Dose Designations Intended Meaning Misinterpretation Correction<br />
and Other Information<br />
Drug name and dose<br />
run together<br />
(especially<br />
Inderal 40 mg Tegretol<br />
300 mg<br />
Mistaken as Inderal 140 mg Mistaken as<br />
Tegretol 1300 mg<br />
Place adequate space between the<br />
drug name, dose, and unit <strong>of</strong><br />
measure<br />
problematic for drug<br />
names that end in<br />
“L” such as<br />
Inderal40 mg;<br />
Tegretol300 mg)<br />
Numerical dose and<br />
The “m” is sometimes mistaken as a zero or Place adequate space between the<br />
unit <strong>of</strong> measure run<br />
two zeros, risking a 10- to 100-fold overdose dose and unit <strong>of</strong> measure<br />
10 mg 100 mL<br />
together (e.g., 10mg,<br />
100mL)<br />
Abbreviations such<br />
The period is unnecessary and could be Use mg, mL, etc. without a<br />
as mg. or mL. with a<br />
mistaken as the number 1 if written poorly terminal period<br />
mg mL<br />
period following the<br />
abbreviation<br />
Large doses without<br />
properly placed<br />
commas (e.g., 100000<br />
units; 1000000 units)<br />
100,000 units 1,000,000<br />
units<br />
100000 has been mistaken as 10,000 or<br />
1,000,000; 1000000 has been mistaken as<br />
100,000<br />
Use commas for dosing units at<br />
or above 1,000, or use words<br />
such as 100 "thousand" or 1<br />
"million" to improve readability<br />
Drug Name<br />
Abbreviations<br />
Intended Meaning Misinterpretation Correction<br />
ARA A vidarabine Mistaken as cytarabine (ARA C) Use complete drug name<br />
AZT zidovudine (Retrovir) Mistaken as azathioprine or aztreonam Use complete drug name<br />
CPZ<br />
Compazine<br />
(prochlorperazine)<br />
Mistaken as chlorpromazine<br />
Use complete drug name<br />
DPT<br />
Demerol-Phenergan- Mistaken as diphtheria-pertussis-tetanus<br />
Thorazine<br />
(vaccine)<br />
Use complete drug name<br />
DTO Diluted tincture <strong>of</strong> opium, Mistaken as tincture <strong>of</strong> opium<br />
Use complete drug name<br />
or deodorized tincture <strong>of</strong><br />
opium (Paregoric)<br />
HCl hydrochloric acid or<br />
hydrochloride<br />
Mistaken as potassium chloride (The “H” is<br />
misinterpreted as “K”)<br />
Use complete drug name unless<br />
expressed as a salt <strong>of</strong> a drug<br />
HCT hydrocortisone Mistaken as hydrochlorothiazide Use complete drug name<br />
HCTZ hydrochlorothiazide<br />
Mistaken as hydrocortisone (seen as HCT250<br />
mg)<br />
Use complete drug name<br />
MgSO4** magnesium sulfate Mistaken as morphine sulfate Use complete drug name<br />
MS, MSO4** morphine sulfate Mistaken as magnesium sulfate Use complete drug name<br />
MTX methotrexate Mistaken as mitoxantrone Use complete drug name<br />
PCA procainamide Mistaken as Patient Controlled Analgesia Use complete drug name<br />
236
PTU propylthiouracil Mistaken as mercaptopurine Use complete drug name<br />
T3<br />
Tylenol with codeine No.<br />
3<br />
Mistaken as liothyronine<br />
Use complete drug name<br />
TAC triamcinolone Mistaken as tetracaine, Adrenalin, cocaine Use complete drug name<br />
TNK TNKase Mistaken as “TPA” Use complete drug name<br />
ZnSO4 zinc sulfate Mistaken as morphine sulfate Use complete drug name<br />
Stemmed Drug Names Intended Meaning Misinterpretation Correction<br />
“Nitro” drip nitroglycerin infusion Mistaken as sodium nitroprusside infusion Use complete drug name<br />
“Norflox” norfloxacin Mistaken as Norflex Use complete drug name<br />
“IV Vanc” intravenous vancomycin Mistaken as Invanz Use complete drug name<br />
Symbols Intended Meaning Misinterpretation Correction<br />
Dram Minim<br />
Symbol for dram mistaken as “3” Symbol for Use the metric system<br />
minim mistaken as “mL”<br />
x3d For three days Mistaken as “3 doses” Use “for three days”<br />
> and < Greater than and less than Mistaken as opposite <strong>of</strong> intended; mistakenly Use “greater than” or “less than”<br />
use incorrect symbol; “< 10” mistaken as “40”<br />
/ (slash mark) Separates two doses or<br />
indicates “per”<br />
Mistaken as the number 1 (e.g., “25 units/10<br />
units” misread as “25 units and 110” units)<br />
Use “per” rather than a slash<br />
mark to separate doses<br />
@ At Mistaken as “2” Use “at”<br />
& And Mistaken as “2” Use “and”<br />
+ Plus or and Mistaken as “4” Use “and”<br />
° Hour Mistaken as a zero (e.g., q2° seen as q 20) Use “hr,” “h,” or “hour”<br />
_ ISMP 2003<br />
** Identified abbreviations above are also included on the JCAHO's "minimum list" <strong>of</strong> dangerous abbreviations, acronyms and symbols<br />
that must be included on an organization's "Do NotUse" list, effective January 1, 2004. An updated list <strong>of</strong> frequently asked questions<br />
about this JCAHO requirement can be found on their website at www.jcaho.org.<br />
ISMP MedicationSafetyAlert!<br />
237
COMPREHENSIVE WRITE-UPS<br />
Definition <strong>of</strong> Comprehensive Write-up<br />
A Comprehensive Write-up is a complete history and physical or a problem-focused note in<br />
standard Problem-Oriented Medical Record form (see following examples) and includes:<br />
a) a complete Problem List, with problems designated as “active” or<br />
“inactive/resolved” with dates <strong>of</strong> onset and resolution, respectively<br />
b) a comprehensive Assessment <strong>of</strong> at least three (3) problems from the Problem<br />
List, with discussion <strong>of</strong> differential diagnoses <strong>of</strong> undiagnosed problems (including rationale for<br />
including/excluding diagnoses) or discussion <strong>of</strong> diagnosed problems (such as course,<br />
complications, control and compliance)<br />
c) Plans, divided into Diagnostic, Therapeutic and Education Plans<br />
d) Resources and References<br />
e) Student’s name, printed and signed, followed by “MS3”<br />
f) Abbreviations: Since medical records communicate important information and<br />
may be scrutinized, abbreviations should not be used because their meaning is not universal<br />
among all readers <strong>of</strong> the medical records. Specifically, students should not use error-prone<br />
abbreviations, symbols, and dose designations (see Appendix).<br />
Submission Requirements <strong>of</strong> Comprehensive Write-ups<br />
a) 6B and 6L students on Inpatient <strong>Medicine</strong> are required to submit 3 write-ups by halfway<br />
through the inpatient rotation (averaging 1 write-up each week). The Hospital Site Coordinator<br />
will decide whether these 3 write-ups are satisfactory. If they are deemed satisfactory, then<br />
the student will not be required to submit any more write-ups. If, however, they are deemed<br />
unsatisfactory, then the student will be required to submit 1 – 3 additional write-ups, as<br />
determined by the Hospital Site Coordinator, up to a maximum <strong>of</strong> 6 write-ups.<br />
b) 6B students on Ambulatory <strong>Medicine</strong> are required to submit 2 write-ups each week for a<br />
total <strong>of</strong> 10 write-ups to their Ambulatory Preceptor.<br />
c) 6L students on Ambulatory <strong>Medicine</strong> are required to submit 2 write-ups each month for<br />
a total <strong>of</strong> 10 write-ups to their Ambulatory Preceptor.<br />
d) All write-ups, either originals with corrections/comments from the preceptor or copies <strong>of</strong><br />
the originals with corrections/comments, must be turned in by the last day <strong>of</strong> the respective<br />
inpatient or ambulatory component <strong>of</strong> the <strong>clerkship</strong>.<br />
238
Example <strong>of</strong> Inpatient History and Physical<br />
Date <strong>of</strong> Admission: 11/01/02<br />
Date <strong>of</strong> Exam: 11/01/02<br />
ID: 78-yo Japanese woman who is a widow and a retired hotel worker<br />
S/R: Patient and her daughter, who are fair historians. Medical records not available.<br />
RE: Admission to Progressive Care Unit at Kuakini Medical Center<br />
CC: Three episodes <strong>of</strong> "Bloody stools" since last night<br />
HPI: The patient is a 78-year old woman with history <strong>of</strong> hypertension, hypercholesterolemia and two<br />
previous "mild strokes", who was in her usual state <strong>of</strong> health until October 29, 2002, three days prior<br />
to admission, when she began passing bright red blood per rectum along with "dark black clots" and<br />
"black stools", The patient claims to have had more than 10 bowel movements <strong>of</strong> this kind within 10<br />
hours. She admits to feeling weak at this time with a "near-fainting" episode after which she found<br />
herself drenched with sweat, as if "someone dumped a bucket <strong>of</strong> water over my head". The patient's<br />
daughter claims that the patient may have experienced a brief loss <strong>of</strong> consciousness (less than 30<br />
seconds.) during this "near-fainting" episode, as she stopped talking for a short period <strong>of</strong> time. On the<br />
morning <strong>of</strong> October 30, 2002, the patient went in to see her physician, Dr. Shozo Ogawa. At this time<br />
the bleeding had ceased and her only complaint was weakness. Dr. Ogawa found her to be stable,<br />
and found her hemoglobin to be 12.2, and arranged for her to follow-up with a gastroenterologist. On<br />
October 31 st , at around 5:00pm, the patient again began to pass bright red blood per rectum, but<br />
without black clots. She says she passed 3 bloody bowel movements since that time until she<br />
presented to the Emergency Room on the morning <strong>of</strong> November 1st. She admits to feeling weak and<br />
"lousy" and again feeling faint, but not actually fainting.<br />
The patient denies any prior episodes <strong>of</strong> rectal bleeding. She had experienced some constipation the<br />
week before, and had used Metamucil, which had given relief. She denies fever, nausea, vomiting,<br />
diarrhea, sick contacts, chest pain, shortness <strong>of</strong> breath, recent weight changes or changes in<br />
appetite. She claims to have a chronic mild right lower quadrant abdominal pain which she attributes<br />
to her degenerative vertebral disc disease. She also admits to having "sour stomach" every few<br />
months, but no history <strong>of</strong> previously diagnosed GERD or peptic ulcer disease.<br />
In 2000, the patient was diagnosed with "degenerative disc disease" in her lower spine. She claims to<br />
have had back pain since age 17, and utilizes a back brace and cane to assist in mobilization. She<br />
has been using aspirin for the pain, with her last dose taken 10 days ago. She was told by her<br />
physician at the <strong>of</strong>fice visit three days ago that "aspirin wasn't good for her stomach" and so she has<br />
since been taking Extra-Strength Tylenol, with gives her only partial relief.<br />
PMH:<br />
Childhood illnesses: Not asked<br />
Immunizations: Not asked<br />
Adult illnesses: Two "mild strokes" (Had slurred speech) in 1970s<br />
Cervical cancer – had possible cone biopsy in 1970s<br />
Hypertension- first aware <strong>of</strong> diagnosis in 1970s<br />
Degenerative disc disease- told <strong>of</strong> diagnosis in 2000; uses back brace, cane, occasional<br />
acupuncture<br />
Cataracts bilaterally- date <strong>of</strong> diagnosis unknown<br />
Hypercholesterolemia- date <strong>of</strong> diagnosis unknown<br />
The patient has no history <strong>of</strong> bleeding disorder, liver disease, diabetes mellitus, myocardial infarction<br />
or renal disease.<br />
Hospitalizations/Surgeries:<br />
1950s Kapiolani Medical Center- birth <strong>of</strong> her children<br />
239
1960s Kapiolani Medical Center- Hysterectomy, reason for surgery unknown.<br />
1998 Queens Medical Center- "surgery for the insides coming out the vagina"<br />
Transfusions: Not asked<br />
Current medications: Covera HS (verapamil) 240mg qd<br />
Tylenol 1 tab every 4-6 hrs pm back pain, last dose taken 1 day ago<br />
Aspirin- dosage unknown, last dose taken 10 days ago<br />
Allergies: Penicillin reaction unknown; told by doctor not to take penicillin<br />
Sulfa acute onset <strong>of</strong> "red rash and skin peeling in sheets" (1960s)<br />
Cortisone face swelling<br />
FH: Patient's father died in his 40s from “stomach cancer." Mother died in her 90s <strong>of</strong> a "stroke, and<br />
had diabetes mellitus. The patient has numerous siblings, some <strong>of</strong> whom are step-siblings. One sister<br />
has diabetes. Two <strong>of</strong> the step-siblings have died, causes unknown. Health status <strong>of</strong> the other siblings<br />
are unknown. There is no family history <strong>of</strong> bleeding disorders.<br />
40s<br />
“Stomach ca”<br />
90<br />
“Stroke”<br />
“DM”<br />
Personal Pr<strong>of</strong>ile/SH: The patient is a retired hotel worker and widow. She now lives with her<br />
daughter. She denies the use <strong>of</strong> cigarettes, alcohol or illicit drugs. Her diet consists mostly <strong>of</strong> cereals,<br />
oatmeal and bread. She doesn't each much fruit or vegetables.<br />
ROS:<br />
General: See HPI. Denies weight loss, fever.<br />
Skin: Has no rash, itching, bruising.<br />
Eyes: Reports no blurry vision, other visual disturbances.<br />
Ears: Reports no hearing loss, tinnitus, pain, discharge, vertigo.<br />
Nose: Has "allergies” which cause runny nose, sneezing, cough.<br />
Mouth: Has no gingivitis, sore tongue, taste changes, dental problems<br />
Throat: Reports no pain, voice changes<br />
Pulmonary: Reports no chest pain, pneumonia, SOB, DOE, wheezing, sputum, hemoptysis<br />
Circulatory system: Has no chest pain, palpitations, dyspnea, PND, orthopnea, edema, syncope<br />
GI: See HPI; has no change in appetite, dysphagia, nausea, vomiting, rectal pain, hematemesis,<br />
diarrhea, peptic ulcer disease<br />
GU: Reports no frequency, nocturia, polyuria, urgency, dysuria, hematuria, hesitancy, urinary flow<br />
240
changes, retention, incontinence; has no history <strong>of</strong> kidney problems<br />
Female genitalia: See PMH.<br />
Breast: Not asked<br />
Sexual Hx: Not asked<br />
Endocrine system: Reports no neck mass, thyroid problems, exophthalmos, heat/cold intolerance,<br />
thirst changes<br />
Hemopoietic system: Has no lymph node enlargement, excessive bleeding, bruising, anemia<br />
Musculoskeletal system: See HPI and PMH. Has other joint or muscle pain.<br />
Nervous system: Has no history <strong>of</strong> head trauma, headaches, numbness, paralysis, convulsions,<br />
seizures, tremor, gait disturbances, coordination changes<br />
Mood: Not asked.<br />
PE:<br />
General Appearance: Patient appears well-nourished, appearing her stated age. She is lying<br />
comfortably in bed, in no evident distress. She is alert, oriented and cooperative.<br />
Vital Signs: Temp 96.0; Respirations 11; Oxygen sat 99% on Room Air; Supine- HR 89, BP 147/64;<br />
Standing- HR 110, BP 131/54<br />
Skin: Warm, dry, pale<br />
Head: Nontender over scalp<br />
Eyes: Acuity not tested. PERRL. Extraocular mucles function intact. Fundi not visualized due to<br />
cataracts.<br />
Ears: Acuity not tested. Pinna- no lesions, nontender. Canals- no bleeding. TMs not visualized due to<br />
cerumen obscuring view. Nose: normal pink mucosa nontender. no discharge.<br />
Mouth: Mucosa pink, moist, slightly pale. No lesions or bleeding. No tonsillar erythema or exudates.<br />
Neck: Supple. No thyromegaly, enlarged lymph nodes, jugular venous distention; no carotid bruits.<br />
Pulmonary: Lungs clear to percussion and ausculatation bilaterally, anteriorly and posteriorly<br />
Cardiac: No thrills, lifts or heaves. PMI palpated in left 5th ICS at the midclavicular line, non-bounding.<br />
Rate and rhythm are regular, normal S1 and S2. No murmurs, extra heart sounds heard.<br />
Abdomen: S<strong>of</strong>t, non-tender, non-distended. Normoactive bowel sounds in four quadrants. No<br />
hepatosplenomegaly by palpation..<br />
Rectal (done by ER physician- reported as showing no masses, with “pink stool”. Bright red blood on<br />
glove which tested positive with hemoccult.<br />
Extremities: Full motion in all extremities. No clubbing, cyanosis, edema. Patient was slow to stand,<br />
and had an antalgic gait she attributed to back pain.<br />
Neuro: Alert and oriented x 3. Cranial Nerves: II - XII grossly intact. Speech slightly slurred, difficult to<br />
comprehend at times. Sensation normal to light touch and 10 gram mon<strong>of</strong>ilament; motor 5/5 in all<br />
extremities. DTRs 2+ in biceps, triceps, knees and ankles. No Babinski response is noted.<br />
Admission lab results:<br />
CBC: WBC 7.9, differential: Bands 7, Segs 50, Lymphs 37, Monocytes 5, Eos O, Baso 1<br />
Hgb 9.8 (was noted to have been 12.2, 2 days PTA),<br />
Hct 28.4<br />
MCV 93.9<br />
Platelet count 238<br />
BMP: Na 140 BUN 20 PT 12.3<br />
K 3.6 Creatinine 0.7 INR 1.0<br />
Cl 110 Glucose 135 PTT 22<br />
Bicarb 25<br />
241
Problem List<br />
Problem<br />
No.<br />
Date Onset Active Problems Date Resolved Inactive/Resolved<br />
Problems<br />
1. 1960s Allergic reaction to sulfa (rash,<br />
peeling skin)<br />
2. 1970s 1970s Hx <strong>of</strong> cervical cancer<br />
s/p TAHBSO<br />
3. 1970s Hx <strong>of</strong> “mild stroke x2<br />
slurred speech<br />
4. 1970s Hypertension<br />
5. 1998 Bladder prolapse s/p<br />
corrective surgery<br />
6. 2000 Degenerative disc disease <br />
chronic lower back pain<br />
7. 10-29-02 GI bleed<br />
8. 11-01-02 Anemia<br />
9. Unknown Hypercholesterolemia<br />
10. Unknown Unknown Bilateral cataracts<br />
s/p cataract surgery<br />
11. Unknown Allergy to penicillin<br />
(unknown reaction), cortisone<br />
(facial swelling)<br />
Problem #1: Bleeding per rectum<br />
Assessment: The patient has experienced 2 episodes <strong>of</strong> bloody stools in the past three days, during<br />
which time she has had more many bloody bowel movements. During the first episode, she describes<br />
bright red blood as well as “black clots.” In the most recent episode, she reports only bright red<br />
blood. She has been feeling weak since these episodes. In addition, there is evidence that this patient<br />
has had substantial blood loss including: (1) a decrease in hemoglobin from 12.2 to 9.8 in two days<br />
with normal MCV, which suggest an acute bleed; (2) orthostatic changes with an increase in HR <strong>of</strong><br />
>20 and decrease in Systolic BP > 15mmHg suggest that the patient is hypovolemic, with a blood<br />
loss <strong>of</strong> greater than 1 Liter. In trying to identify the source <strong>of</strong> the bleed we must attempt to differentiate<br />
an upper GI bleed from a lower GI bleed, as well as confirm that the bleeding is from the rectum and<br />
not from the vagina or urethral orifice. Because the rectal exam confirms that there is blood in the<br />
rectum, we can assume the patient does have a GI bleed. With the reports <strong>of</strong> “bright red blood", it is<br />
likely that the patient is having a lower GI bleed, although a brisk upper GI bleed could also present<br />
as bright red blood per rectum. The “black clots” seen in the first episode suggest a possible upper GI<br />
bleed, in which the “clots” may have been melenic stool.<br />
The differential diagnosis <strong>of</strong> lower GI bleed include diverticulosis, colon cancer or polyps, ulcerative<br />
colitis, angiodysplasia, and hemorrhoids. Diverticulosis is likely as it most common in the elderly and<br />
can present<br />
with painless bright red blood per rectum that can result in massive hemorrhage. A diverticular<br />
242
hemorrhage is usually caused by erosion <strong>of</strong> a blood vessel by a fecalith within the diverticular sac.<br />
The patient did have some recent constipation which could have lead to the development <strong>of</strong> a<br />
fecolith. She took Metamucil for relief. It is unknown if the patient then had diarrhea, which can occur<br />
with Metamucil; but if she did, it is possible that the<br />
diarrhea in its rapid transit through the colon could have dislodged the fecalith resulting in injury to a<br />
blood<br />
vessel and hemorrhage. Diverticular bleeding stops spontaneously in the majority <strong>of</strong> patients. This<br />
was not the case for this patient. This could be due to the rupture <strong>of</strong> a large blood vessel in the colon,<br />
or it could be due to the patient's chronic use <strong>of</strong> aspirin (which can inhibit platelet aggregation<br />
resulting in decreased clotting ability for about 7-10 days, however, she claims to have not had<br />
aspirin for 10 days prior to admission).<br />
Colon cancer is also possible. Like diverticular disease, it is more common in the elderly. The patient<br />
displays signs and symptoms that are characteristic <strong>of</strong> a left colonic cancer- change in bowel habits<br />
(constipation, diarrhea) and bright red blood per rectum. Intestinal obstruction is also common with a<br />
left colon cancer, however the patient did not complain <strong>of</strong> abdominal pain or tenderness which would<br />
be expected with obstruction. A right colon carcinoma would present with an iron deficiency anemia<br />
due to chronic blood loss, which can be occult and thus unknown to the patient, and a dull vague<br />
abdominal pain. The patient did have a chronic dull lower right quadrant abdominal pain. She also<br />
had anemia (Hgb 9.8), however this anemia appears to be due to the acute blood loss and not iron<br />
deficiency as her Hgb was 12.2 two days prior to admission, and her MCV was normal.<br />
Ulcerative colitis should also be considered, although more commonly diagnosed in younger adults,<br />
there is also a small peak incidence among the elderly, ages 50-65. Although the patient is beyond<br />
this peak, UC must still be considered given that it's hallmark is bloody diarrhea. Most patients with<br />
UC will also have fever and weight loss, which this patient did not have. Angiodysplasia/AVM is also<br />
possible as it is most commonly seen in the elderly and presents with painless bright red blood per<br />
rectum. Hemorrhoids can be a cause <strong>of</strong> rectal bleeding, however there is usually associated pain<br />
and a palpable rectal mass, which this patient did not have. Infectious colitis is less likely in this<br />
patient as she is has no fever, abdominal pain or leukocytosis, all <strong>of</strong> which would be expected with an<br />
infectious process. The patient also denies any sick contacts.<br />
A brisk Upper GI bleed could also be responsible for this patient's rectal bleeding, however with such<br />
a large amount <strong>of</strong> blood loss, one would also expect some hematemesis, which did not occur. The<br />
differential would include gastritis, vascular ectasia, peptic ulcer disease and ruptured varices.<br />
Gastritis is very likely given the patient's chronic use <strong>of</strong> aspirin. However, she does not have<br />
abdominal pain which might be expected if it were severe enough to have caused this patient's<br />
bleeding. Peptic ulcer disease is less likely as pain is its predominant symptom, and the patient<br />
denied any abdominal or chest pain. It is important to rule-out a gastric ulcer in this patient, or to<br />
diagnose and treat it, as an untreated ulcer can increase her risk <strong>of</strong> developing gastric cancer. She is<br />
already at risk given her Japanese ethnicity and positive family history <strong>of</strong> gastric cancer. Ruptured<br />
varices is unlikely as the patient has no hematemesis and no history <strong>of</strong> liver disease which would<br />
cause the formation <strong>of</strong> varices. Her normal coagulation studies make liver disease unlikely. Given the<br />
numerous possible diagnoses for this patient's GI bleed it is imperative to have the patient to undergo<br />
both upper endoscopy and colonoscopy, especially given her history <strong>of</strong> both bright red blood per<br />
rectum and “black clots".<br />
Plan: Admit to acute care hospital with careful monitoring <strong>of</strong> vital signs.<br />
Plans:<br />
Diagnostic:<br />
-Place NG tube to assess for gastric bleeding<br />
243
-Consult a gastroenterologist for upper endoscopy and colonoscopy<br />
Treatment:<br />
-Type and crossmatch. Transfuse 2 units packed red blood cells to replace blood loss, since she is at<br />
risk to cntinue bleeding<br />
-No food or drink in preparation for endoscopy according to gastroenterologist instructions<br />
-Further treatment dependent on endoscopic findings. Consider initiate gastric acid blocking regimen<br />
prophylactically<br />
Patient education:<br />
-Inform patient <strong>of</strong> the possible diagnoses and the need for careful monitoring and testing<br />
-Inform patient <strong>of</strong> endoscopic procedures, explain risks and benefits, obtain informed consent<br />
-Inform patient <strong>of</strong> need for transfusion, explain risks and benefits, obtain informed consent<br />
Problem #2: Anemia<br />
Assessment: The patient has developed an acute anemia. Her hemoglobin had dropped 2.4 G/dL<br />
(from 12.2 to 9.8), which correlates with a decrease in hematocrit <strong>of</strong> approximately 7%. Hematocrit<br />
generally falls 2-3 points for every 500 mL <strong>of</strong> blood lost, making the estimated blood loss in this<br />
patient 3.5L. The normal MCV also suggests that the anemia is due to an acute blood loss. The<br />
normal coagulation studies rule-out a coagulopathy that may complicate the patient's GI bleed,<br />
although platelet dysfunction due to the patient's chronic aspirin use may exacerbate the bleed. The<br />
patient's orthostatic changes in heart rate and systolic BP is consistent with blood loss <strong>of</strong> greater than<br />
1 liter resulting in hypovolemia. The patient appears pale with pale mucous membranes and has<br />
complaints <strong>of</strong> weakness and light-headedness, which are all due to her anemia. It is important to<br />
transfuse this patient and increase her hemoglobin in order to avoid the complications associated with<br />
anemia and hypovolemia, such as high output cardiac failure and organ hypoperfusion, which may be<br />
<strong>of</strong> greater risk in the elderly.<br />
Plans:<br />
Diagnostic:<br />
-Monitor blood count every 4 hrs for continued bleeding and decrease in hemoglobin<br />
Treatment:<br />
- Place adequate intravenous access (2 large bore peripheral catheters)<br />
-Type and crossmatch. Transfuse 1 unit packed red cellss now.<br />
-Intravenous fluids: normal saline at 100cc/hour<br />
-Transfuse packed red cells to keep hemoglobin > 10 G/dL<br />
Patient education:<br />
-Inform patient <strong>of</strong> need for transfusion, explain risks and benefits, obtain informed consent<br />
-Inform patient <strong>of</strong> signs and symptoms <strong>of</strong> worsening anemia that she should be aware <strong>of</strong>, such as<br />
worsening orthostatic hypotension, weakness, faintness, pallor, tachycardia.<br />
Problem #3: Back pain<br />
Assessment: The patient has been previously diagnosed with degenerative disc disease and suffers<br />
from chronic back pain. She regularly uses a back brace and cane to assist with mobilization. She<br />
occasionally has acupuncture treatments to relieve the pain. She had been taking aspirin on a regular<br />
basis for pain, and recently changed to Extra-Strength Tylenol which gives only partial relief. Given<br />
the possibility <strong>of</strong> gastritis, it is best for the patient to avoid aspirin and any other NSAID, especially<br />
with an active GI bleed. Once the bleeding has resolved, a specific COX-2 inhibitor could be<br />
considered, although there is still a risk <strong>of</strong> GI irritation with COX2 inhibitors, the risk is less than that <strong>of</strong><br />
nonspecific NSAIDs. Given the patient's allergic reaction to sulfa, celecoxib is contraindicated;<br />
however, r<strong>of</strong>ecoxib can be used. In clinical trials with r<strong>of</strong>ecoxib, 3.9% <strong>of</strong> the patients had a reported<br />
sulfa sensitivity, none developed anaphylactic reactions. Another option would be to administer<br />
misoprostol along with the NSAID, in order to further protect the gastric mucosa. In order to<br />
244
completely avoid NSAIDs but still provide complete relief, tramadol could be considered. tramadol is<br />
a centrally acting analgesic which acts as an opiate agonist, although it is not opioid-derived.<br />
Tramadol does not irritate gastric mucosa, thus not causing an increased risk for GI bleed. Side<br />
effects reported for tramadol include constipation, dizziness, nausea, dry mouth, sweating and<br />
minimal cardiovascular effects including hypotension, tachycardia and syncope. Given the patients<br />
current gastritis, recent GI bleed and sulfa allergy, tramadol might be the best choice for pain relief in<br />
this patient should she request more complete relief than she is currently receiving with Tylenol; while<br />
being aware <strong>of</strong> possible hypotensive effects <strong>of</strong> this drug.<br />
Plans:<br />
Diagnostic: No further diagnostic studies at this time.<br />
Treatment:<br />
-Continue Tylenol 1 gram every 4-6 hrs as needed for back pain, not to exceed 4g daily<br />
-If better pain control is desired, consider starting tramadol 25 mg daily<br />
Patient education:<br />
-Inform patient <strong>of</strong> the need to avoid NSAIDs<br />
-Inform patient <strong>of</strong> the daily maximum dose <strong>of</strong> Tylenol (4 G per day) and the adverse effects that could<br />
occur in the event <strong>of</strong> toxicity<br />
-Inform patient that a trial <strong>of</strong> tramadol could be started, with attention to added side effects, if better<br />
pain control is needed<br />
--------------------------------------------------------------------------------------<br />
Resources:<br />
AHFS Drug Information, 2002<br />
Ferri. Practical Guide to the Care <strong>of</strong> the Medical Patient, 5th ed., 2001<br />
Myers. NMS <strong>Medicine</strong>, 4th ed" 2001<br />
<br />
Toby Best, MS 3<br />
245
Example <strong>of</strong> Ambulatory Note<br />
Problem List<br />
Problem<br />
#<br />
Date <strong>of</strong><br />
onset<br />
Active Problems Date<br />
resolved<br />
Inactive/Resolved<br />
Problems<br />
1. 9/14/04 Pharyngitis<br />
2. 1998 Hypertension<br />
3. 1994 Obesity<br />
4. 1973 S/P Appendectomy<br />
Date <strong>of</strong> Examination: September 17, 2004<br />
ID: 40 year old Part <strong>Hawaii</strong>an woman<br />
SR: History obtained from the patient and medical records, which are reliable.<br />
RE: Scheduled <strong>of</strong>fice visit<br />
CC: Sore throat and fever x3 days<br />
Problem #1: Pharyngitis<br />
S: This 40 year old woman presents to the <strong>of</strong>fice per chief complaint. 3 days ago patient began<br />
having fever, chills, sore throat, rhinorrhea, myalgia, and fatigue. She denies cough, dyspnea,<br />
wheezing, otalgia, dysphagia, abdominal pain, nausea, vomiting, diarrhea or constipation. She has<br />
taken Advil, which improves symptoms. There are no sick contacts. Patient is able to swallow solids<br />
and liquids.<br />
Patient is taking oral contraceptives, and has no medication allergies.<br />
O:<br />
General: Well-groomed, cheerful woman who appears stated age.<br />
Not in acute distress.<br />
VS: T 97.5°F; P 78; R 12; BP 112/68; Wt 159 lbs.; Ht. 61 in.<br />
Skin: Warm, dry, intact. No rashes, petechiae, or bruising noted.<br />
Ears: Symmetrical auricles, canals nontender. Auditory canals clear and<br />
non-erythematous bilaterally. Tympanic membrane intact and pearly with clear cone <strong>of</strong> light<br />
bilaterally.<br />
Nose:<br />
Nares patent, septum midline, clear discharge.<br />
Mouth/Throat: Erythema and yellowish exudate present on posterior pharynx and<br />
tonsils bilaterally. Mucous membranes moist. Lips without cyanosis or lesions. Uvula midline.<br />
Tongue pink, moist. Parotids<br />
nonpalpable.<br />
Neck:<br />
Supple, no lymphadenopathy, no masses, non-tender to palpation.<br />
Trachea midline.<br />
Lungs: Clear to percussion and auscultation bilaterally. No wheezes, rales or coarse breath<br />
sounds.<br />
Heart:<br />
No thrills or heaves felt. RRR. S1 and S2 <strong>of</strong> equal intensity. No<br />
murmurs or rubs heard.<br />
246
A: While the differential diagnosis <strong>of</strong> acute pharyngitis in adults includes a number <strong>of</strong> bacterial and<br />
viral pathogens, the objective in evaluating a patient with pharyngitis is to identify those with group A<br />
streptococcus (GAS) pharyngitis. The patient’s symptoms and physical findings suggest possible<br />
group A streptococcal pharygitis. Although viruses are the most common cause <strong>of</strong> acute pharyngitis,<br />
Group A strep pharyngitis accounts for approximately 10% <strong>of</strong> acute pharyngitis in adults. It presents<br />
with the sudden onset <strong>of</strong> sore throat, tonsillar exudate, tender cervical adenopathy, and fever.<br />
Malaise, headache, abdominal pain and vomiting may also occur. The absence <strong>of</strong> fever or presence<br />
<strong>of</strong> cough, conjunctivitis, hoarseness, coryza, viral exanthem, and diarrhea strongly suggest a viral<br />
rather than a streptococcal etiology. The Centor criteria for predicting GAS have been the most widely<br />
used and accepted and include, 1) tonsillar exudate; 2) tender anterior cervical adenopathy; 3) fever<br />
by history; 4) absence <strong>of</strong> cough. If three or four <strong>of</strong> these criteria are met, the positive predictive value<br />
is 40% to 60%. However, the presence <strong>of</strong> less than three has a negative predictive value <strong>of</strong> 80%. By<br />
these criteria, this patient has a 40-60% probability <strong>of</strong> having GAS pharyngitis.<br />
Throat cultures have always been the "gold standard" for diagnosing GAS pharyngitis with a<br />
sensitivity <strong>of</strong> 90% and specificity <strong>of</strong> 95-99% if collected properly. However, cultures take 24 to 48<br />
hours to grow, therefore cannot be used to decide which patients merit antibiotic therapy. Thus, rapid<br />
antigen detection test (RADT) has assumed greater importance in managing acute pharyngitis.<br />
RADT uses enzyme or acid extraction <strong>of</strong> antigen from throat swabs followed by latex agglutination,<br />
co-agglutination, or enzyme linked immunoabsorbent assay (ELISA) procedures to demonstrate<br />
antigen-antibody complexes. The majority <strong>of</strong> RADTs that are currently available have a sensitivity <strong>of</strong><br />
80-90% and specificity <strong>of</strong> >95%. It is also advantageous because it can yield results within<br />
approximately 10 minutes. Rapid identification and treatment <strong>of</strong> those with strep pharyngitis can<br />
reduce the risk <strong>of</strong> its spread, allowing the patient to return to school or work sooner, result in faster<br />
resolution <strong>of</strong> signs and symptoms (by 1-2 days), and can reduce the risk <strong>of</strong> suppurative complications<br />
and acute rheumatic fever. A positive result <strong>of</strong> either throat culture or RADT provides adequate<br />
confirmation <strong>of</strong> the presence <strong>of</strong> GAS in the pharynx. In children, a negative RADT should be<br />
confirmed with a throat culture result while in adults a negative RADT is sufficient to exclude this<br />
diagnosis, because the risk for acute rheumatic fever in adults is extremely low. Serologic tests for<br />
antistreptococcal antibody titers reflect past and not present immunologic events and are <strong>of</strong> no value<br />
in the diagnosis <strong>of</strong> acute pharyngitis.<br />
The major goal <strong>of</strong> identifying patients with GAS pharyngitis is to prescribe antibiotics to these patients<br />
and not treat the others, especially those with pharyngitis caused by a virus in order to limit antibiotic<br />
resistance. Recent guidelines from the Infectious Diseases Society <strong>of</strong> America (IDSA) regarding<br />
principles <strong>of</strong> management in cases <strong>of</strong> sore throat include: (1) use <strong>of</strong> clinical and epidemiologic<br />
features to distinguish patients who may have GAS pharyngitis; and (2) antibacterial treatment only<br />
for cases confirmed with a laboratory test (culture or rapid test). In contrast, a position paper by the<br />
American College <strong>of</strong> Physicians–American Society <strong>of</strong> Internal <strong>Medicine</strong>/American Academy <strong>of</strong> Family<br />
Physicians/US Centers for Disease Control and Prevention, while endorsing the IDSA approach in<br />
children, recommends a departure from the principle <strong>of</strong> laboratory confirmation <strong>of</strong> all adult cases. The<br />
suggested strategies are: empirically treat patients who have all four Centor clinical criteria (fever,<br />
tonsillar exudate, tender anterior cervical adenopathy, and absence <strong>of</strong> cough); do not treat nor<br />
perform diagnostic tests on patients with zero or one criterion; perform RADT on those with two or<br />
three criteria and use antibiotic treatment for patients with positive RADT results. Empiric treatment<br />
<strong>of</strong> all patients with 3 or 4 Centor criteria can result in unnecessary antibiotic exposure to at least 50<br />
percent <strong>of</strong> patients. Some authorities, including the Infectious Diseases Society <strong>of</strong> America, find this<br />
unacceptable and recommend antibiotics only if there is a positive RADT or culture. This criterion will<br />
result in undertreatment <strong>of</strong> 10-20%, but the consequences <strong>of</strong> undertreatment in adults are rare. This<br />
patient has three out <strong>of</strong> the four Centor criteria, so under both current recommendations patient<br />
should have a RADT done to determine if antibiotic therapy is warranted.<br />
247
Most oral antibiotics must be administered for the conventional 10-day regimen. Penicillin remains<br />
the treatment <strong>of</strong> choice in treating acute streptococcal pharyngitis because <strong>of</strong> its proven efficacy,<br />
safety, narrow spectrum, and low cost. Amoxicillin is <strong>of</strong>ten used in young children, while erythromycin<br />
is a suitable alternative for patients who are allergic to penicillin. First-generation cephalosporins are<br />
also acceptable for patients allergic to penicillin who do not manifest immediate-type hypersensitivity<br />
to beta-lactam antibiotics. Intramuscular benzathine penicillin G is preferred for patients who are<br />
unlikely to complete a full 10-day course <strong>of</strong> oral therapy. Antibiotics can affect the metabolism and/or<br />
efficacy <strong>of</strong> oral contraceptives, which the patient is using. Antibiotic therapy with penicillin should be<br />
started if patient’s RADT is positive.<br />
Symptomatic treatment, including antipyretics, fluids, and gargles, can be helpful. One study showed<br />
that herbal tea (Throat coat), containing ingredients such as licorice root that may relieve irritation,<br />
provided significant temporary relief to the intensity <strong>of</strong> sore throat with swallowing compared to<br />
placebo tea. However herbal teas should be used with caution in this patient because <strong>of</strong> her<br />
hypertension and potential medication interactions. Licorice may cause hypokalemia, so should<br />
probably not be used by a patient taking a thiazide diuretic. Regardless <strong>of</strong> RADT results, patient<br />
should be advised to use acetaminophen for pain and fever, drink increased amounts <strong>of</strong> fluid, and<br />
possibly gargle for symptomatic relief. Side effects <strong>of</strong> NSAIDs can worsen hypertension, and there<br />
are potential drug interactions with antihypertensive medications including β-blockers. Also, use<br />
caution in recommending a decongestant for this patient because <strong>of</strong> her hypertension. However, her<br />
hypertension is well-controlled, so it would probably be safe to use medications such as<br />
pseudephedrine.<br />
Although complications <strong>of</strong> GAS are rare in adults, they include acute rheumatic fever, acute<br />
glomerulonephritis, toxic shock syndrome, tonsillopharyngeal abscess, otitis media, sinusitis,<br />
necrotizing fasciitis, bacteremia, and meningitis. If patient tests positive for GAS, she should be<br />
educated on the possible complications and the signs and symptoms to watch for. She should also<br />
be reminded to return if her symptoms become worse or do not improve within a few days.<br />
P. Diagnostic<br />
Run a rapid antigen detection test to check for Group A Streptococcus pharyngitis.<br />
Therapeutic<br />
If RADT positive: oral penicillin 250 mg PO three times a day for 10 days. Pt should be cautioned use<br />
a back up method <strong>of</strong> contraception while taking the antibiotics because <strong>of</strong> the potential drug<br />
interactions.<br />
Acetaminophen 500 mg PO every 4-6 hours as needed for fever<br />
Salt gargles, tea to relieve sore throat.<br />
Patient Education<br />
If RADT negative: Explain rationale for not using antibiotics.<br />
If RADT positive: Stress importance <strong>of</strong> finishing the 10-day course <strong>of</strong> antibiotics, remind patient that<br />
she is still contagious until she has been on antibiotics for 24 hours, and educate her on the signs and<br />
symptoms <strong>of</strong> possible complications.<br />
Encourage patient to drink adequate amounts <strong>of</strong> fluid. Educate on “recipe” <strong>of</strong> NaCl solution for<br />
gargle- ¼ tsp table salt to a full cup <strong>of</strong> water, and remind her not to swallow this salty solution!.<br />
Reassure patient that asymptomatic household contacts do not need a routine culture <strong>of</strong> throat swab<br />
specimen, unless there is a “ping-pong” spreading <strong>of</strong> GAS pharyngitis within the family.<br />
Return for a follow-up visit if symptoms do not improve within a few days.<br />
Follow-up in 2-3 days if symptoms do not improve.<br />
248
Problem #2: Hypertension<br />
S. No chest pain, palpitations, dizziness, headaches, shortness-<strong>of</strong>-breath, wheezing, orthopnea,<br />
PND or edema. Pt is taking Ziac (bisoprolol/hydrochlorothiazide) 5 mg/6.25 mg, two tablets in the<br />
morning, and denies any symptomatic side effects from the medication. She exercises by walking for<br />
30 minutes three times a week. She eats a well-balanced diet and limits her sodium intake.<br />
O:<br />
VS: As above<br />
Eyes: Sclera clear, conjunctiva pink, no discharge. Extraocular muscles<br />
intact, pupils equal, round, reactive to light and accommodation.<br />
No papilledema, nicking, or cotton wool spots.<br />
Neck: No jugular venous distention<br />
Lungs:<br />
As above<br />
Heart: As above<br />
Circulation: Posterior tibial and pedal pulses 2+ bilaterally. No jugular venous<br />
distention.<br />
Extremities: No edema.<br />
A: Patient’s blood pressure is well-controlled with lifestyle modifications and Ziac. The JNC VII<br />
guidelines indicate that she is below goal blood pressure <strong>of</strong>
W., et al. JAMA. 2004 Apr 7;291(13):1587-95.<br />
“Principles <strong>of</strong> Appropriate Antibiotic Use for Acute Pharyngitis in Adults” Snow et al. Ann Intern<br />
Med.2001; 134: 506-508.<br />
Practice Guidelines for the Diagnosis and Management <strong>of</strong> Group A Streptococcal Pharyngitis,<br />
Infectious Disease Society <strong>of</strong> America.<br />
Harrison’s Online<br />
<br />
N.O. Itall, MS 3<br />
250
CLINICAL SKILLS EXAMINATION (CSE)<br />
STUDENT INSTRUCTIONS<br />
(Revised 6/12)<br />
DESCRIPTION<br />
The CSE is a practical examination consisting <strong>of</strong> 5 - 10 clinical problems including patient<br />
encounters and writing stations. The examination requires you to interact with standardized patients<br />
who volunteer for this exercise. These patients may have real clinical findings or are carefully trained<br />
to simulate patients with “real” medical problems. You should interview and examine these patients<br />
as if they are being seen in an actual patient care situation.<br />
GENERAL PROCEDURES<br />
You will have 15 minutes with each patient. You are responsible for pacing your visit with the patient.<br />
The timer will announce the beginning <strong>of</strong> each patient session. You will be warned when there are 5<br />
minutes remaining in each station, when to rotate to and begin the next station. Do not enter an exam<br />
room until told to begin. Each <strong>of</strong> you will start at a different point along the exam route and will<br />
continue to rotate until all stations are completed. If 2 (or more) students end up in the same station<br />
at the same time, notify the exam monitor immediately.<br />
Please knock before entering a patient's room. If you are finished evaluating the patient before the<br />
15 minutes are up, you may leave the station and begin answering questions in the writing station.<br />
Introduce yourself to the standardized patients as you would introduce yourself to any patient. End<br />
the encounter as you would end any encounter. On the door <strong>of</strong> every patient's room you will find<br />
student instructions in a RED FOLDER. Do not open the RED FOLDER until the timer says, “begin<br />
the encounter.” Reading the student instructions is considered part <strong>of</strong> your 15 minutes with the<br />
patient. In general, there will be enough time to review the instructions for 1 to 2 minutes and still<br />
complete your task with the patient.<br />
The instructions will give you the patient’s name, age, gender and reason for the visit. The<br />
instructions may also indicate where you are seeing the patient (outpatient clinic, emergency room,<br />
etc.), and the time <strong>of</strong> day (if it is different from the current time). The vital sign including the<br />
temperature, heart rate, blood pressure and respiratory rate may also be given. You should accept<br />
the vital signs as accurate and you do not need to repeat them unless you feel the case specifically<br />
requires it.<br />
Your task with the patient will be specifically defined. For example the instructions may tell you to<br />
take an appropriate history and counsel the patient . . . or take an appropriate history and perform a<br />
focused physical examination. You are to perform a focused examination <strong>of</strong> each patient that is<br />
consistent with the instructions provided. Hand washing is an essential practice when seeing patients<br />
and should be considered as a requirement during this examination. Facilities for washing your<br />
hands are available in each examining room.<br />
READ THE INSTRUCTIONS CAREFULLY BEFORE ENTERING EACH STATION. Do not take the<br />
RED FOLDER containing the student instructions into the examination room. A copy <strong>of</strong> the<br />
instructions will be placed in each room for your reference. If you feel it is necessary, you may take<br />
notes on the blank sheets provided on your clipboard. PLEASE DO NOT WRITE ON THE STUDENT<br />
INSTRUCTIONS.<br />
251
You should not perform rectal, genital, breast or corneal reflex examinations on your patients. If you<br />
feel that one or more <strong>of</strong> these maneuvers should be included as part <strong>of</strong> the work up for the patient<br />
you should inform the patient (e.g. “Mrs. Smith, the next step would be to do a pelvic and rectal<br />
examination on you”) and/or include it as part <strong>of</strong> your proposed diagnostic evaluation. As part <strong>of</strong> the<br />
encounter, you should provide the patient with your initial impression and initial management plan.<br />
End the encounter with the patient as you would end any patient encounter.<br />
You will receive a supply <strong>of</strong> “BUSINESS CARDS” pre-printed with your Examinee Identification<br />
Number. Before leaving the patient's rooms please leave one card with the patient (e.g. "If you have<br />
any questions or need to get in touch with me, here is my card"). This will allow the standardized<br />
patient to complete your evaluation forms. If you forget to give your card to the patient please leave<br />
it with the monitor and he/she will bring it in to the patient. ONCE YOU LEAVE THE PATIENT'S<br />
ROOM, YOU ARE NOT ALLOWED TO RE-ENTER FOR ANY REASON.<br />
WRITING STATIONS (PATIENT NOTE):<br />
Immediately after each patient encounter will begin a “writing station” where you will answer specific<br />
questions related to the encounter. Depending on the station, you will be writing your answers on<br />
paper or entering them on a computer.<br />
For stations requiring paper and pen, take one TEST BOOKLET from the blue folder located at the<br />
writing station. WRITE IN YOUR ASSIGNED STUDENT EXAMINEE ID# ON YOUR TEST<br />
BOOKLET and then begin answering the questions. You will have 10 minutes to answer the<br />
questions and complete any evaluation forms. Remember to write clearly, as we must be able to<br />
read your writing to grade it. When you have finished, turn your paper faced down on the desk. A<br />
proctor will pick up these forms.<br />
For stations requiring computer entry, log on to the computer using your UH USERNAME AND<br />
PASSWORD. Enter the Patient’s ID Number (located in a blue folder next to the computer monitor)<br />
to access the entry form for the station and begin answering the questions. You will have 10 minutes<br />
to answer the questions and complete any evaluation forms. When you have finished, remember to<br />
LOGOUT.<br />
In most stations, you will be asked to describe the significant positive and negative clinical findings<br />
uncovered during your interaction with the patient that will allow you to make clinical decisions, your<br />
differential diagnosis in the order <strong>of</strong> likelihood, and/or your INITIAL DIAGNOSTIC management plan<br />
(See Attached Sample Patient Note form). LIST only one item for each numbered blank line. Be as<br />
specific as possible.<br />
BREAKS<br />
You are asked not to leave the examination area during the break times and to refrain from<br />
discussing the cases with each other.<br />
CONTENT OF EXAM<br />
The clinical situations for this examination reflect the “General Core Clinical Competencies and<br />
“Training Problems” described in the <strong>Medicine</strong> 531/532 Student Handbook. You are being evaluated<br />
based on checklists and rating scales completed by the patient and by the responses you provide in<br />
the test booklet regarding your findings (writing stations). You are not allowed to consult any medical<br />
references during the exam.<br />
252
PAGERS/CELLULAR PHONES<br />
Cellular phones and pagers will not be allowed inside the examination area. We can hold<br />
them for you while you take the examination, but we will not be responsible for loss or damages.<br />
Please plan accordingly.<br />
EQUIPMENT<br />
1. STETHOSCOPE<br />
2. REFLEX HAMMER<br />
3. PENS with black ink<br />
4. NAME TAG<br />
5. PROPER ATTIRE. You should dress as you would to see patients.<br />
6. Otoscopes, ophthalmoscopes, sphygmomanometers, tongue blades, reflex hammers, drapes, clip<br />
boards and other supplies will be available in each examination room.<br />
GRADING AND FEEDBACK<br />
Student performance on each station is scored based on the following component scores, weighted<br />
as follows:<br />
Communication/Interpersonal Skills 30-40%<br />
Hx-Taking/Physical Exam/Counseling 40-50%<br />
Problem Solving (writing stations) 10-30%<br />
The Total Examination Score is calculated based on the average <strong>of</strong> the scores on each station.<br />
Students must achieve Clerkship Level Competency on this examination to receive credit for Med<br />
531, and Graduation Level Competency to receive credit for Med 541.<br />
Each student will receive a feedback letter with their Total Score and breakdown <strong>of</strong> their component<br />
scores. In addition, the average ratings by the standardized patients on specific communication skills<br />
(introducing self, active listening, showing interest etc), will also be provided. Unfortunately, we<br />
cannot return the actual checklists and written test materials without compromising the cases which<br />
may be used on future examinations.<br />
IMPORTANT REMINDER:<br />
You must have your UH Login and Password to complete this examination.<br />
253
FREQUENTLY ASKED QUESTIONS:<br />
Q1: How can I best prepare for this examination?<br />
A1: Review the Training Problems and General Core Clinical Competencies sections <strong>of</strong> your<br />
Med531/532 Student Handbook. For each <strong>of</strong> the Training Problems listed, be able take an<br />
appropriate history and focused physical examination. Understand how specific signs and symptoms<br />
relate to the differential diagnosis for each problem. Most importantly, review and practice good<br />
communication and interpersonal skills when seeing patients during the rotation.<br />
Q2: Are all the stations equal in length and difficulty?<br />
A2: Some stations, especially those requiring both a focused history and focused physical<br />
examination, seem to take everyone longer than other stations, although there is great variability<br />
among students. All <strong>of</strong> the stations are designed to be completed in the time allotted. The more<br />
difficult stations require students to focus their examination on obtaining the most relevant clinical<br />
information. The passing score for each station is adjusted for case difficulty.<br />
Q3: What does the interstation exercise (writing station or patient note) look like?<br />
A3: See example below.<br />
254
JOHN DOE -- PATIENT NOTE<br />
EXAMINEE ID # ____ ____<br />
DATE: __/__/__<br />
HISTORY: Include significant positives and negatives from history <strong>of</strong> present illness, past medical<br />
history, review <strong>of</strong> system(s), social history and family history.<br />
PHYSICAL EXAMINATION: Indicate only pertinent positive and negative findings related to the<br />
patient’s chief complaint.<br />
DIFFERENTIAL DIAGNOSES: In order <strong>of</strong><br />
likelihood (with 1 being most likely), list up to<br />
5 potential or possible diagnoses for this<br />
patient’s presentation (in many cases, fewer<br />
than 5 diagnoses are likely).<br />
1.<br />
2.<br />
3.<br />
4.<br />
5.<br />
DIAGNOSTIC WORK UP: List immediate<br />
plans (up to 5) for further diagnostic workup.<br />
1.<br />
2.<br />
3.<br />
4.<br />
5.<br />
255
NBME SUBJECT EXAM IN INTERNAL MEDICINE<br />
256
MEDICINE<br />
General Principles 1%-5%<br />
Organ Systems 95%-99%<br />
Immunologic Disorders 5%-10%<br />
Diseases <strong>of</strong> the Blood and Blood-forming Organs<br />
5%-10% Diseases <strong>of</strong> the Nervous System and Special Senses<br />
5%-10% Cardiovascular Disorders<br />
15%-20% Diseases <strong>of</strong> the Respiratory System<br />
15%-20% Nutritional and Digestive Disorders<br />
10%-15% Gynecologic Disorders<br />
1%-5%<br />
Renal, Urinary, and Male Reproductive System<br />
10%-15% Disorders <strong>of</strong> the Skin and Subcutaneous Tissues<br />
5%-10% Diseases <strong>of</strong> the Musculoskeletal System and Connective<br />
Tissue 5%-10% Endocrine and Metabolic Disorders<br />
Physician Tasks 5%-10%<br />
Promoting Health and Health Maintenance<br />
10%-15% Understanding Mechanisms <strong>of</strong> Disease<br />
20%-25% Establishing a Diagnosis<br />
40%-45% Applying Principles <strong>of</strong> Management<br />
20%-25%<br />
1. A 22-year-old woman with a 10-year history <strong>of</strong><br />
asthma comes to the physician because she has had to<br />
increase her use <strong>of</strong> her albuterol inhaler during the past 6<br />
weeks. Her asthma was previously well controlled with<br />
inhaled glucocorticoids. She has a 2-year history <strong>of</strong><br />
generalized anxiety disorder controlled with fluoxetine and a<br />
5-year history <strong>of</strong> migraines. The migraines were well<br />
controlled with sumatriptan until 4 months ago when she<br />
began to have headaches twice weekly; propranolol was<br />
added to her regimen at that time. She has been taking an<br />
oral contraceptive for the past year. She says she has been<br />
under increased stress at graduate school and in her<br />
personal life during the past 3 months; during this period,<br />
she has been drinking an average <strong>of</strong> four cups <strong>of</strong> c<strong>of</strong>fee<br />
daily (compared with her usual one cup daily). She does not<br />
drink alcohol or use illicit drugs. She appears mildly anxious<br />
but is not in respiratory distress. Scattered end-expiratory<br />
wheezes are heard. The remainder <strong>of</strong> the examination<br />
shows no abnormalities. Which <strong>of</strong> the following is the most<br />
likely cause <strong>of</strong> the exacerbation <strong>of</strong> this patient's asthma?<br />
(A) Fluoxetine therapy<br />
(B) Increased caffeine intake<br />
(C) Oral contraceptive therapy<br />
(D) Propranolol therapy<br />
(E) Sumatriptan therapy<br />
2. A 28-year-old woman has palpitations that occur<br />
approximately once a week, last 1B5 minutes, and consist <strong>of</strong><br />
rapid, regular heart pounding. The episodes start and stop<br />
suddenly and have not been associated with chest discomfort<br />
or dyspnea. There is no history <strong>of</strong> heart problems. She drinks<br />
two to three cups <strong>of</strong> c<strong>of</strong>fee daily. She rarely drinks alcohol<br />
and does not smoke. Her pulse is 96/min and regular, and<br />
blood pressure is 120/88 mm Hg. A stare and lid lag are<br />
noted. The thyroid gland is firm and 1.5 times larger than<br />
normal. There is a midsystolic click at the apex and a grade<br />
2/6, early systolic murmur at the upper left sternal border. An<br />
ECG is normal except for evidence <strong>of</strong> sinus tachycardia.<br />
Which <strong>of</strong> the following is the most appropriate next step in<br />
diagnosis?<br />
(A) Ambulatory ECG monitoring<br />
(B) Measurement <strong>of</strong> serum thyroidstimulating<br />
hormone concentration<br />
(C) Measurement <strong>of</strong> urine<br />
catecholamine concentration<br />
(D) MUGA scan<br />
(E) Echocardiography<br />
257
3. A study is conducted to assess the benefits <strong>of</strong> a new drug to 5. Two days after receiving 3 units <strong>of</strong> packed red blood cells for<br />
reduce the recurrence <strong>of</strong> colonic polyps. The results postpartum hemorrhage, a 24-year-old woman has<br />
show a number needed to treat (NNT) <strong>of</strong> 16. Which <strong>of</strong> fatigue and slight jaundice. Laboratory studies show:<br />
the following is the most accurate interpretation <strong>of</strong> this<br />
result?<br />
Hemoglobin 8.8 g/dL<br />
(A) For every 16 patients treated, 1 would<br />
Hematocrit 28% Serum total<br />
benefit from the new drug<br />
bilirubin 5 mg/dL<br />
(B) For every 100 patients treated, 16 would<br />
benefit from the new drug<br />
(C) The new drug is 1.6 times more<br />
beneficial than a placebo<br />
(D) 93% <strong>of</strong> patients taking the new drug<br />
would benefit from it<br />
(E) 84% <strong>of</strong> patients taking the new drug<br />
would not have any benefit from it<br />
4. A previously healthy 57-year-old woman comes to<br />
the physician 1 week after noticing a lump under her right<br />
arm. She is concerned that it is breast cancer because both<br />
her mother and maternal aunt died <strong>of</strong> breast cancer. She<br />
does not smoke, drink alcohol, or use illicit drugs. She has<br />
avoided the sun for the past 10 years. She notes that her skin<br />
has never tanned but always burned and freckled when<br />
exposed to the sun. She exercises daily on a stationary<br />
bicycle and eats a well-balanced diet. Her temperature is<br />
37°C (98.6°F), pulse is 82/min and regular, respirations are<br />
14/min, and blood pressure is 130/74 mm Hg. There are<br />
numerous freckles over the entire body. Examination <strong>of</strong> the<br />
right breast shows a 0.6-cm, flat, brown lesion; the lesion is<br />
mottled with deep purple and black areas and has an irregular<br />
border. There are no breast masses, dimpling, peau d'orange,<br />
or nipple discharge. The patient says that the lesion has been<br />
present for 1 year, but she has never had it examined. There<br />
is a firm, nontender mass in the right axilla. Examination<br />
shows no other abnormalities. Which <strong>of</strong> the following is the<br />
most likely diagnosis?<br />
(A) Basal cell carcinoma<br />
(B) Fibrocystic changes <strong>of</strong> the<br />
breast (C) Malignant melanoma<br />
(D) Mastitis<br />
(E) Pigmented nevus<br />
(F) Port-wine stain<br />
(G) Squamous cell<br />
carcinoma (H) Superficial breast<br />
carcinoma<br />
Liver tests are otherwise within normal limits. Which <strong>of</strong><br />
the following is the most appropriate next step in<br />
diagnosis?<br />
(A) Cytomegalovirus antibody titer<br />
(B) Direct and indirect antiglobulin<br />
(Coombs) tests<br />
(C) Monospot test<br />
(D) Serology for hepatitis B<br />
markers (E) Ultrasonography <strong>of</strong> the<br />
gallbladder<br />
6. A 30-year-old man has had nausea, vomiting, and<br />
severe colicky right flank pain radiating into the thigh for 4<br />
hours. He is afebrile. There is right costovertebral angle<br />
tenderness. Urinalysis shows RBCs too numerous to count<br />
and no bacteria. Which <strong>of</strong> the following is the most likely<br />
diagnosis?<br />
(A) Acute glomerulonephritis<br />
(B) Bacterial cystitis<br />
(C) Benign prostatic hyperplasia<br />
(D) Bladder carcinoma<br />
(E) Renal cell carcinoma<br />
(F) Urinary tract tuberculosis<br />
(G) Urolithiasis<br />
7. A 66-year-old woman comes to the emergency<br />
department 1 hour after the sudden onset <strong>of</strong> retrosternal<br />
chest discomfort accompanied by nausea and diaphoresis.<br />
She has hypotension, jugular venous distention, and a<br />
murmur <strong>of</strong> tricuspid regurgitation. An ECG shows STsegment<br />
elevation in the right precordial leads. Which <strong>of</strong> the<br />
following is the most likely diagnosis?<br />
(A) Constrictive pericarditis<br />
(B) Dissecting aortic aneurysm<br />
(C) Pericardial tamponade<br />
(D) Pulmonary emboli<br />
(E) Right ventricular infarction<br />
258
8. A 20-year-old African American woman comes to the physician because <strong>of</strong> a 6-month history <strong>of</strong> diffuse joint pain,<br />
especially in her hips and knees. During this period, she occasionally has had a rash on her nose and cheeks. She has no<br />
history <strong>of</strong> serious illness and takes no medications. Her temperature is 38.1°C (100.5°F). Examination shows warmth and<br />
swelling <strong>of</strong> the knees. Laboratory studies show:<br />
Which <strong>of</strong> the following is the most likely diagnosis?<br />
(A) Ankylosing spondylitis<br />
(B) Gouty arthritis<br />
(C) Psoriatic arthritis<br />
(D) Reactive arthritis<br />
(E) Rheumatoid arthritis<br />
(F) Septic arthritis<br />
(G) Systemic lupus<br />
erythematosus<br />
Hemoglobin 10.5 g/dL Erythrocyte sedimentation rate 40 mm/h<br />
Serum<br />
Urea nitrogen 30 mg/dL Creatinine 1.8<br />
mg/dL<br />
9. A 37-year-old man with type 1 diabetes mellitus<br />
comes to the physician for a routine examination. His only<br />
medication is insulin. His pulse is 72/min, respirations are<br />
12/min, and blood pressure is 138/88 mm Hg. Funduscopic<br />
examination shows microaneurysms and hemorrhages.<br />
Sensation to vibration and light touch is decreased over the<br />
lower extremities. His serum creatinine concentration is 1.6<br />
mg/dL. A 24-hour urine collection shows 550 mg <strong>of</strong> protein.<br />
Treatment with which <strong>of</strong> the following is most likely to slow<br />
progression <strong>of</strong> this patient's renal disease?<br />
(A) Atenolol<br />
(B) Clonidine<br />
(C) Hydralazine<br />
(D) Hydrochlorothiazide<br />
(E) Lisinopril<br />
10. A 50-year-old man is admitted to the hospital within<br />
2 hours <strong>of</strong> the onset <strong>of</strong> nausea, vomiting, and acute<br />
crushing pain in the left anterior chest. He has a family<br />
history <strong>of</strong> early coronary artery disease. The pain does not<br />
subside with the administration <strong>of</strong> nitroglycerin, sublingually.<br />
An ECG shows ST-segment elevation in leads aVL and V2<br />
through V4. Which <strong>of</strong> the following is the most appropriate<br />
management to decrease myocardial damage and<br />
mortality?<br />
(A) Administration <strong>of</strong> digitalis<br />
(B) Administration <strong>of</strong> lidocaine<br />
(C) Administration <strong>of</strong> quinidine<br />
(D) Coronary artery bypass grafting within 1<br />
week<br />
(E) Thrombolytic therapy<br />
11. A previously healthy 67-year-old woman comes to<br />
the physician with her husband because <strong>of</strong> a 4-month history<br />
<strong>of</strong> a resting tremor <strong>of</strong> her right arm. Her husband reports that<br />
her movements have been slower and that she appears less<br />
stable while walking. Examination shows increased muscle<br />
tone in the upper extremities that is greater on the right than<br />
on the left. There is decreased right arm swing. Her gait is<br />
slow and shuffling. Which <strong>of</strong> the following is the most likely<br />
explanation for this patient's symptoms?<br />
(A) Bilateral frontal lobe<br />
degeneration<br />
(B) Decreased dopaminergic input to the<br />
(C) striatum Decreased serotonergic activity in the brain<br />
stem<br />
(D) Excessive output <strong>of</strong> oxytocin<br />
(E) Excessive thalamic output <strong>of</strong><br />
norepinephrine<br />
12. A 47-year-old man comes to the physician because<br />
<strong>of</strong> a 4week history <strong>of</strong> increased thirst and urination. He has<br />
had a 23-kg (50-lb) weight gain during the past 2 years. He<br />
has no history <strong>of</strong> serious illness and takes no medications.<br />
His mother and maternal grandfather have type 2 diabetes<br />
mellitus. The patient does not smoke and drinks one beer<br />
every night. He is 175 cm (5 ft 9 in) tall and now weighs 104<br />
kg (230 lb); BMI is 34 kg/m 2 . His pulse is 90/min, and blood<br />
pressure is 150/88 mm Hg. The remainder <strong>of</strong> the<br />
examination shows no abnormalities. His serum glucose<br />
concentration is 330 mg/dL. Which <strong>of</strong> the following is the<br />
most likely underlying cause <strong>of</strong> this patient's increased<br />
serum glucose concentration?<br />
(A) Autoimmune destruction <strong>of</strong> islet cells<br />
(B) Chronic pancreatitis<br />
(C) Exogenous production <strong>of</strong><br />
corticosteroids<br />
(D) Insulin resistance<br />
(E) Pancreatic cancer<br />
259
13. A previously healthy 39-year-old woman is brought<br />
to the physician because <strong>of</strong> a tingling sensation in her<br />
fingers and toes for 2 days and rapidly progressive<br />
weakness <strong>of</strong> her legs. She had an upper respiratory tract<br />
infection 2 weeks ago. She was unable to get up from bed<br />
this morning. Examination shows weakness <strong>of</strong> all four<br />
extremities, distal greater than proximal. Deep tendon<br />
reflexes are absent. Sensation is mildly decreased over the<br />
feet. Which <strong>of</strong> the following is the most likely diagnosis?<br />
(A) Guillain-Barré syndrome<br />
(B) Multiple sclerosis<br />
(C) Myasthenia gravis<br />
(D) Poliomyelitis<br />
(E) Tick paralysis<br />
14. A previously healthy 77-year-old woman who<br />
resides in a skilled nursing care facility is brought to the<br />
emergency department 6 hours after the onset <strong>of</strong> acute<br />
midback pain that began while lifting a box. The pain does<br />
not radiate, and she has no other symptoms. She continues<br />
to carry out her daily activities. She appears to be in mild<br />
distress. She is 157 cm (5 ft 2 in) tall and weighs 47 kg (104<br />
lb); BMI is 19 kg/m 2 . Examination shows mild tenderness<br />
over T11. There is no tremor. Serum studies show a calcium<br />
concentration <strong>of</strong> 9.1 mg/dL, a urea nitrogen concentration <strong>of</strong><br />
12 mg/dL, and a creatinine concentration <strong>of</strong> 0.5 mg/dL. An x-<br />
ray <strong>of</strong> the dorsal and lumbar spine shows an anterior wedge<br />
fracture <strong>of</strong> T11. In addition to treating the pain,<br />
supplementation with which <strong>of</strong> the following is most likely to<br />
improve this patient's underlying condition?<br />
(A) 25-Hydroxycholecalciferol<br />
(B) Levothyroxine<br />
(C) Selenium<br />
(D) Vitamin C<br />
(E) Vitamin E<br />
15. A 52-year-old woman comes to the physician<br />
because <strong>of</strong> a 3-month history <strong>of</strong> diarrhea and intermittent<br />
abdominal pain that radiates to her back. The pain is<br />
exacerbated by eating. She describes her stools as greasy,<br />
foul-smelling, and difficult to flush. She has had a 4.5-kg<br />
(10-lb) weight loss during the past 4 months. She has a<br />
history <strong>of</strong> chronic alcohol abuse. Examination shows mild<br />
epigastric tenderness. An x-ray <strong>of</strong> the abdomen shows<br />
calcifications in the epigastrium. Which <strong>of</strong> the following is<br />
the most likely diagnosis?<br />
(A) Bacterial overgrowth<br />
(B) Celiac disease<br />
(C) Lactose intolerance<br />
(D) Malabsorption <strong>of</strong> bile salts<br />
(E) Pancreatic insufficiency<br />
16. A 67-year-old woman comes to the physician<br />
because <strong>of</strong> an 8-month history <strong>of</strong> progressive shortness <strong>of</strong><br />
breath. The shortness <strong>of</strong> breath initially occurred only with<br />
walking long distances but now occurs after walking ¼ mile<br />
to her mailbox. She also has a daily morning cough<br />
productive <strong>of</strong> whitish tan sputum. She has had no chest pain,<br />
palpitations, orthopnea, or paroxysmal nocturnal dyspnea.<br />
She has smoked one pack <strong>of</strong> cigarettes daily for 52 years.<br />
Her pulse is 88/min, respirations are 20/min, and blood<br />
pressure is 144/90 mm Hg. Examination shows a barrelshaped<br />
chest. Breath sounds are decreased, and faint<br />
expiratory wheezes are heard in all lung fields. There is no<br />
peripheral edema. An x-ray <strong>of</strong> the chest shows no<br />
abnormalities except for hyperinflation. Which <strong>of</strong> the<br />
following is the most likely diagnosis?<br />
(A) Angina pectoris<br />
(B) Asthma<br />
(C) Chronic obstructive pulmonary<br />
disease<br />
(D) Chronic pulmonary embolism<br />
(E) Congestive heart failure<br />
(F) Panic disorder<br />
17. A 22-year-old woman comes to the physician<br />
because <strong>of</strong> a 10-day history <strong>of</strong> pain in multiple joints. She<br />
first had pain in her right elbow, and then her right shoulder,<br />
and now has pain, redness, and swelling in her left knee that<br />
began 2 days ago. She currently has no pain in the right<br />
shoulder and elbow. There is no history <strong>of</strong> trauma. She is<br />
sexually active, and she and her partner use condoms for<br />
contraception inconsistently. Examination <strong>of</strong> the left knee<br />
shows warmth, erythema, tenderness, and s<strong>of</strong>t-tissue<br />
swelling. Range <strong>of</strong> motion <strong>of</strong> the knee is limited to 10<br />
degrees <strong>of</strong> flexion. The remainder <strong>of</strong> the examination,<br />
including pelvic examination, shows no abnormalities.<br />
Arthrocentesis <strong>of</strong> the knee joint yields 10 mL <strong>of</strong> cloudy fluid<br />
with a leukocyte count <strong>of</strong> 18,300/mm 3 (97% segmented<br />
neutrophils). Microscopic examination <strong>of</strong> the leukocytes<br />
within the joint fluid is most likely to show which <strong>of</strong> the<br />
following?<br />
(A) Acid-fast bacteria<br />
(B) Cuboidal positively birefringent crystals<br />
(C) Gram-negative diplococci<br />
(D) Gram-positive cocci in clusters<br />
(E) Needle-shaped negatively birefringent<br />
crystals<br />
18. A 47-year-old woman comes to the physician for a<br />
routine health maintenance examination. She feels well and<br />
has no history <strong>of</strong> serious illness. Her mother, brother, and<br />
sister have hypertension. The patient's pulse is 84/min, and<br />
blood pressure is 138/85 mm Hg. Examination shows no<br />
abnormalities. The most appropriate recommendation is<br />
decreased intake <strong>of</strong> which <strong>of</strong> the following?<br />
(A) Calcium<br />
(B) Carbohydrates<br />
(C) Potassium<br />
(D) Protein<br />
(E) Sodium<br />
260
19. A 32-year-old man comes to the physician because<br />
<strong>of</strong> a 12day history <strong>of</strong> abdominal cramps and bloating,<br />
diarrhea, and flatulence. He says that he started a new<br />
exercise program 2 weeks ago and has been consuming a<br />
high quantity <strong>of</strong> yogurt bars, peanut butter, and protein- and<br />
calorie-enriched milk shakes to "bulk up." He has no history<br />
<strong>of</strong> serious illness and takes no medications. His temperature<br />
is 37°C (98.6°F). The abdomen is distended, nontender, and<br />
tympanitic to percussion. Bowel sounds are increased. The<br />
remainder <strong>of</strong> the examination shows no abnormalities. Which<br />
<strong>of</strong> the following is the most likely cause <strong>of</strong> this patient's<br />
symptoms?<br />
(A) Allergy to peanuts<br />
(B) Fungal overgrowth in the small<br />
bowel<br />
(C) Incarcerated hernia<br />
(D) Irritable bowel syndrome<br />
(E) Lactase deficiency<br />
20. A 22-year-old college student comes to student<br />
health services because <strong>of</strong> a 7-day history <strong>of</strong> low-grade<br />
fever, sore throat, fatigue, and general malaise. One month<br />
ago, she had a painless vulvar ulcer that resolved<br />
spontaneously; she has been otherwise healthy. Her last<br />
menstrual period was 3 weeks ago; she uses tampons<br />
regularly. She is sexually active and has had three partners<br />
since the age <strong>of</strong> 15 years; she uses an oral contraceptive.<br />
Her temperature is 38°C (100.4°F), pulse is 100/min, and<br />
blood pressure is 110/60 mm Hg. Examination shows a rash<br />
over the palms and soles and mild cervical<br />
lymphadenopathy. Pelvic examination shows no<br />
abnormalities. Which <strong>of</strong> the following is the most appropriate<br />
pharmacotherapy?<br />
(A) Acyclovir<br />
(B) Dexamethasone<br />
(C) Interferon<br />
(D) Penicillin<br />
(E) Zidovudine (AZT)<br />
261
Answer Form for <strong>Medicine</strong> Subject Test Sample Questions<br />
(Questions 1-20)<br />
1. _____<br />
2. _____<br />
3. _____<br />
4. _____<br />
5. _____<br />
6. _____<br />
7. _____<br />
8. _____<br />
9. _____<br />
10. _____<br />
11.<br />
12.<br />
13.<br />
14.<br />
15.<br />
16.<br />
17.<br />
18.<br />
19.<br />
20.<br />
262
Answer Key for <strong>Medicine</strong> Subject Test Sample Questions<br />
(Questions 1-20)<br />
1. D 11. B<br />
2. B 12. D<br />
3. A 13. A<br />
4. C 14. A<br />
5. B 15. E<br />
6. G 16. C<br />
7. E 17. C<br />
8. G 18. E<br />
9. E 19. E<br />
10. E 20. D<br />
263